
Abstract
Abstract
Peromelia or congenital transverse deficiency describes a truncation of the upper limb below various limb levels. Recommendations regarding treatment vary and are mainly based on expert opinions. This paper summarizes the current literature regarding the aetiology, pathogenesis and specifically treatment algorithms for children with peromelia. We performed a non-systematic review of the current literature from MEDLINE/PubMed to obtain comprehensive up-to-date information about peromelia, focusing on current recommendations for the treatment of peromelia (e.g. prosthetic fitting, external stump lengthening). The current literature lacks clear evidence as to whether prosthetic treatment is superior to prosthetic non-usage. However, based on the available studies, children with transradial or transhumeral peromelia should preferably be fitted with passive/cosmetic prostheses at the age between six and 24 months, followed by active/myoelectric devices at the age of 2.5 to four years. It remains controversial whether early myoelectric prosthetic fitting can reduce prosthesis rejection times; however, cognitive readiness and the ability to absolve a guided training programme are seen as important prerequisites for myoelectric fitting. Children with very short stumps may benefit from stump lengthening using external fixators and prosthetic modification. The treatment of children with peromelia generally requires a guided, multidisciplinary team approach. A training programme is essential to optimize individuals’ performance in the execution of activities of daily living and decrease rejection risks whenever a myoelectric device is prescribed. Myoelectric fitting should preferably be commenced at no later than four years of age. However, long-term reports on the benefits of prosthetic treatment are still pending.
Keywords
Introduction
Congenital transverse deficiency, transverse failure of formation, or peromelia, which is also incorrectly known as congenital above/below-elbow amputation, describes a truncation of the upper limb below various limb levels. Due to the paucity of literature on this topic we conducted a non-systematic MEDLINE/PubMed review in May 2018 to search for recent literature on peromelia, including e.g. its aetiology, pathogenesis and current treatment options thereof. Besides these up-to-date results, our report aims to present a standardized clinical and radiographic assessment plan for patients with this entity.
Aetiology and pathogenesis
Congenital transverse deficiencies have been estimated to account for 6% of all congenital hand differences, with an incidence of about one in 20 000 live births.1,2 It is almost universally non-hereditary and not associated with other organ anomalies or syndromes. Thus, special evaluation by paediatricians or geneticists is usually not necessary. 3
Agents with vasoconstriction effects such as misoprostol, cocaine and tobacco have been implicated as teratogenic factors, providing support for the vascular pathogenetic theory.4–6 However, a transverse deficiency is rarely related to exogenic teratogens. It should be suspected especially when multiple limbs are involved. 3 This condition has also been associated with alcohol consumption and recently with maternal trombophilia.7,8
The molecular pathogenesis of the transversal growth arrest of the limb is thought to be related to disruptive events affecting the apical ectodermal ridge (AER) after limb buds form. The AER, a condensed layer of ectoderm over the limb bud, is a signalling centre responsible for proximal to distal limb development. 9 Secretion of fibroblast growth factors guides the underlying mesoderm to differentiate into proper structures progressing from proximal to distal with the shoulder forming first. 10 Experimental animal models supported the role of the AER in proximo-distal limb formation. 9 For example, the removal of the AER results in a limb truncation which can be avoided by the application of fibroblast growth factors. 11
Classification
This disorder is classified according to the level of limb truncation. The most common level of truncation is the proximal forearm (below-the-elbow, Fig. 1), followed by transcarpal, distal forearm, and brachial above-the-elbow levels. 10 Congenital transverse deficiencies above or below the elbow have been traditionally classified as transverse deficiency (failure of formation of parts) by Swanson's classification. 12 However, before the introduction of the classification of Swanson, a different classification was already published by Frantz and O'Rahilly, which was later modified by Burtch.13–15

Two cases involving children with a short stump and below-elbow peromelia are shown. Both of them exhibit rudimentary digits and skin dimples, which can have detrimental effects on hygiene and prosthetic fitting.
This system introduced the concepts of ‘meromelia’ (partial absence of a free limb) and terminal transverse (T) absence both for upper and lower limb. Moreover, each part of a limb has been indicated using the first letter of the part's name in capital letters, for example, H, R, and U for humerus, radius, and ulna, respectively, as well as the first letter of the affected segment's name, for example, P, M, and D for proximal, medium and distal. Therefore, considering the upper limb above and below the elbow, two different clinical classifications are possible:
Meromelia T –; H (absence of humerus at the proximal, middle or distal level and all distal segments) Meromelia T –; RU (absence of forearm bone at the proximal, middle or distal level and all distal segments)
Although the modified Frantz and O'Rahilly classification seems to be very comprehensive and complete, the International Organization for Standardization/International Society for Prosthetics and Orthotics (IPO/ISPO) classification of congenital limb deficiency is probably easier to use in clinical practice.
16
The limb is described based on where it terminates and the different clinical presentations above or below the elbow:
Upper arm
Upper third Middle third Lower third Forearm
Upper third Middle third Lower third
In 2010, Oberg et al 17 published a new classification of hand and upper limb anomalies based on the new genetic and biological information about the development of upper limbs in the foetus. Following this new system, the congenital above/below elbow amputation has been classified as a malformation with an abnormal axis formation/differentiation affecting the proximal/distal axis of the upper limb.
Clinical and radiographic assessment
First, a careful history including obstetrical and genetic information as well as maternal exposure to teratogenic agents, although not common, should be acquired. Moreover, it is important to know whether a prenatal diagnosis has been performed because it may have implications on how well-prepared, informed and anxious the parents are. 18
A transverse deficiency is almost always unilateral. 19 Regarding the affected limb, the examination should be directed to understand the exact level of truncation, the state of the skin on the top of the stump and the function of the muscles proximal to the truncation. Commonly, nubbins and/or skin dimples are present at the distal end of the limb, which is usually well cushioned (Fig. 1). In the below-elbow deficiency, elbow flexion is usually present, whereas wrist flexion is present in the transcarpal type.
The child should then be examined entirely in order to identify other associated anomalies. Apart from the affected limb, assessment should take into consideration the contralateral upper limb, lower limbs, head, face, cranial and peripheral nerves, chest, abdomen, spine and anal structures. In case of a rare syndromic association, the orthopaedic examination should be followed by a genetic consultation.
In case of patients who wear a prosthesis, muscle strength and the range of movement should be examined with and without the prosthesis. After observing the function of the limb, clinical tests such as those listed below can help the physician assess function:
The Unilateral Below Elbow Test (UBET) The University of New Brunswick Test of Prosthetics Function (UNB) The Skill Index Ranking Scale (SIRS)
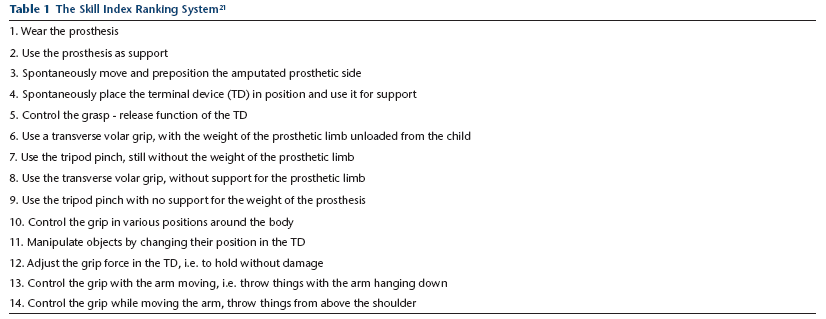
The UBET and the UNB tests consist of similar activities but the score is different. The former focuses on the spontaneity of prosthetic use, whereas the latter presents a difficulty level in performance. 20 The SIRS, in contrast, describes the child's accomplishments when using the prosthesis on a scale of 1 to 14 (levels 1 to 4 for wearing the prosthesis; levels 5 to 14 for using myo hand). 21 This scale is particularly useful for documenting progress during prosthetic training and occupational therapy (Table 1).
The Skill Index Ranking System 21
Laboratory tests may seldom be indicated in patients with dysmorphic features in order to identify genetic or other abnormalities secondary to organ involvement.
A radiograph of the affected limb is a basic exam, which should be carried out to better identify the level of amputation and particularly the length of the stump, especially in below-elbow deficiencies. However, the cartilaginous part of the bone is not yet visible on the radiograph in infants, and therefore further images may be acquired later during the child's growth. Supplemental imaging, such as magnetic resonance imaging may only be indicated in more complex cases.
Treatment
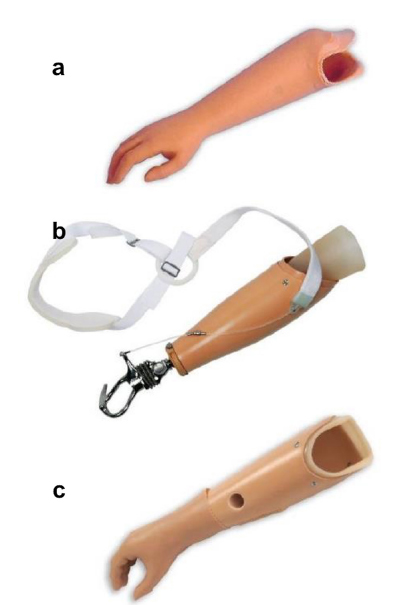
Children with transradial or transhumeral peromelia can nowadays be fitted using three different prosthetic devices: cosmetic (passive), body-powered (active) or myoelectric (active) prostheses (Fig. 2). The main goal of a cosmetic prosthesis is to imitate a missing upper extremity using a relatively light device which, however, can only assist with passively holding objects; no active grasp is possible with this type. Nevertheless, this type is often the first device provided to infants to stimulate their body image and retain body balance and symmetry. In contrast, body-powered prostheses are self-operated by the patients’ stump, shoulder and shoulder girdle with a bandage. Although this device can actively aid in daily life, its use is rather unpopular due to unavoidably unnatural forms of upper limb and shoulder movements during usage (Fig. 2c). Relevant advances have recently been achieved in the field of myoelectric prostheses. This type of prosthesis uses muscle energy, detected by electrodes at the skin surface of the deficient limb part, and transforms these potentials into signals to the control device of the prosthesis. The movements of the prosthetic hand can be either simple (e.g. open/close, pinch grip; Myobock, Ottobock SE & Co. KGaA, Duderstadt, Germany; Fig. 3a) or more complex (open/close in two modes, flexible multiaxial wrist joint, flexible thumb, four flexible fingers; Michelangelo, Ottobock SE & Co. KGaA; Fig. 3b). These independent movements of thumb, index and wrist are particularly desired by prosthetic users. 22 Such myoelectric prostheses are available for infant, adolescent, to adult hand sizes (e.g. Vincentyoung, Vincent Systems GmbH, Karlsruhe, Germany; Touch Bionics, Össur Deutschland GmbH, Frechen, Germany; Bebionic, Ottobock SE & Co. KGaA; Fig. 3c). These devices have been shown to be beneficial in clinical practice because they can contribute in a significant manner to the patient's rehabilitation and mental health.23,24 Functional tasks can more easily be accomplished with myoelectric than with conventional prostheses (Fig. 4).23–25 A reduced prosthesis weight seems important to achieve a high acceptance rate among patients. 26 It may sometimes be necessary to remove nubbins and/or skin dimples to improve fitting and cosmesis. However, despite prosthetic fitting, withdrawn or anxious behaviour can still be present in children with peromelia. 24 The treatment of children with peromelia should, however, be individualized, as not every child may benefit from wearing a prosthesis in the long-term. Therefore, a multidisciplinary team approach is necessary to analyze which child qualifies for this option, and to determine how functional outcomes can be optimized.
Commonly available (

Current myoelectric devices offer different options for terminal grasp, ranging from (
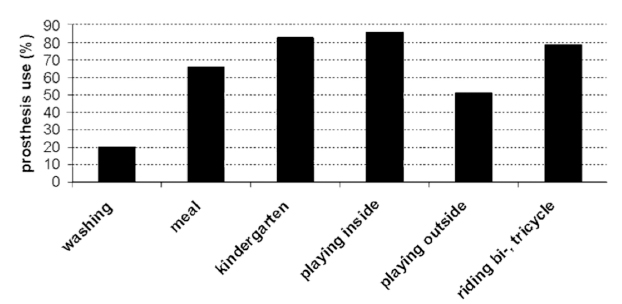
The myoelectric prosthesis was used for certain activities of daily living among a cohort of 41 children as shown in the graph (reproduced with permission from Egermann et al 23 ).
Clinical outcomes of prosthetic fitting in children
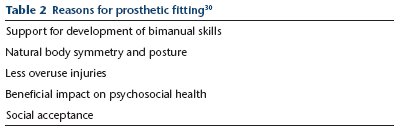
First-time prosthetic fitting with a cosmetic device is usually initiated between six months (“sit to fit”) and 24 months of age. However, the optimal age for prosthetic fitting is still controversial. Many authors believe that early fitting can enhance and increase physical skills and decrease prosthesis rejection time. A systematic review indeed revealed a trend towards lower rejection rates in children who were fitted with their first prosthesis before the age of two years. 27 However, no relationship was found between the age of first fitting and clinical outcomes, and the authors thus concluded that prescription should rather be guided by clinical experience. 27 A recent study from Sweden compared children who were younger and older than 2.5 years at the time of first fitting with a myoelectric device. 28 The skills according to the SIRS improved constantly without any statistical difference between groups, but interestingly, the patients (< 2.5 years of age) showed a less frequent use compared with the controls (>2.5 years of age) at nine years of age, and had a 2.83 times higher risk of rejection. The authors concluded that children showed a similar developmental pattern for prosthetic use, and fitting after 2.5 years was sufficient to achieve good outcomes. This study confirmed other reports suggesting the age of 2.5 to four years as the age for first time myoelectric fitting.23,29 Cognitive readiness and the ability to absolve a guided training programme are thought to be important prerequisites for myoelectric fitting. Moreover, a multidisciplinary team approach is essential to follow and guide patients and parents successfully throughout these critical early years of life (Tables 2 30 and 3). It is also known that there may be gaps between a child's capacity and eventual performance when using a prosthesis and therefore, this should ideally be evaluated beforehand. 31 Children do not necessarily need to wear a prosthesis for several hours a day, but they should rather use it constantly to perform specific tasks and ADLs successfully. An intensive in-patient occupational training is therefore important to optimize daily prosthetic use in children (Tables 4 and 5).21,23,30,32 Some authors still mentioned that prosthetic use did not lead to a better function or quality of life compared with that of non-wearers for the below-the-elbow type. 33 James et al 33 have shown in a large multicentre trial among 489 children that dedicated outcome measures were significantly higher for prosthesis wearers for the psychosocial domain of the The Pediatric Quality of Life Inventory (PedsQL) only but not for its physical health domain; The Pediatric Outcomes Data Collection Instrument (PODCI) results showed no significant differences between the two groups, and UBET scores showed even better outcomes for the non-wearers. The authors thus questioned the routine prescription of prostheses and emphasized that there is room for technologic improvements. Another study has confirmed that psychosocial health can be improved using a prosthesis, and it was moreover found that delinquent behavior can be reduced. 24 Children fitted with a myoelectric prosthesis exhibited social competence and behaviour/emotional problems similar to those of a normal population, and the authors emphasized the need for social support to eventually achieve satisfying results. 24 Alternatively, some treatment providers favour prosthetic terminals such as hooks to do a desired activity (e.g. grasping the circle wheel, rowing).
Reasons for prosthetic fitting 30
Reasons against prosthetic fitting
Reasons for prosthetic acceptance 30
Reasons for prosthetic rejection 30
Lengthening of stumps with external fixator
Prosthetic management and proper fitting of a prosthesis requires an adequate length of the stump (minimum of 6 cm to 7 cm from the elbow crease), sufficient power of the muscles, enough surface of the stump and an adequate range of movement of the joint. The length of the stump is more important than other factors in order to provide a stable suspension and an effective lever arm. Children with very short congenital transverse deficiency stumps may show fitting problems for the prosthetist. Because the function of the prosthesis is related to the level of the amputation stump that can be fitted, a lower-level prosthetic fitting results in a potentially higher level of upper extremity function. When the stump is too short, the patients act as if they had disarticulation of the elbow/shoulder.
There are few options for the treatment for short upper extremity amputation stumps: stump modification (lengthening of the stump) and prosthetic modification. Lengthening of the arm/forearm is needed to provide a longer above/below-elbow situation with improved function. The application of methods based on distraction osteogenesis in the treatment of acquired/congenital malformation of the upper limb has significantly widened the therapeutic use of these methods.34–36 The Ilizarov device (external fixation frame) has gradually become more useful in the correction and lengthening of arms and forearms in various cases of congenital limb shortening.
One common surgical technique includes a limited incision for the insertion of fixator pins under direct visualization. Threaded fixator pins (2.0 mm to 3.0 mm in diameter) are inserted. The bone is then divided by circumferential corticotomy without violation of the medullary canal. The frame device is assembled with the bone ends in direct apposition under fluoroscopy. The periosteum and soft tissues are closed. After a latency period of five to seven days, the elongation process begins. Lengthening of 0.25 mm is performed four times a day, achieving up to 1 mm length per day. The patient and parents are instructed with regard to the precise lengthening technique and pin site care. Physiotherapy is necessary to promote joint mobility during the lengthening period. The devices are left in place until consolidation of new bone in the fracture gap demonstrates radiographic and clinical stability and a useful length of the stump is achieved.
Most authors have used the Ilizarov method-based lengthening to gain acute length. 37 Seitz et al 38 described indications, technique and pitfalls of 12 bone lengthenings of the upper extremity. Two of them presented congenital transverse deficiency of the forearm with extremely short ulnar segment and functionally non-usable elbow joint. Alekberov et al 39 reported a largest series with six patients with congenital below-elbow stumps, which were lengthened (both radius and ulna) using Ilizarov rings. The mean period of distraction was 62.6 days (40 to 85) with a mean increase in the length of the forearm of 5.6 cm (3.4 to 8.4) without major complications. Orhun et al 36 reported on a ten-year-old patient with congenital transverse deficiency in his forearm. Both the ulna and tibia were lengthened simultaneously with the Ilizarov method without soft tissue complications. Jasiewicz et al 40 described two cases of severe congenital forearm defects with inadequate length of the stumps that also involved treatment using Ilizarov. The total stump elongation was 4 cm and 5 cm and was enough for effective and functional limb prosthesis. Bernstein et al 41 reported on two patients (one bilateral amputation) with congenital above-elbow amputation with stump lengthening to improve non-prosthetic function. Both of them improved their ability to grasp objects and play.
The lengthening of very short above-elbow and below-elbow congenital amputations stumps in children by the Ilizarov or monolateral techniques is a reliable method to obtain adequate stumps and also allows some correction of elbow contractures. This technique increases the possibilities of prosthesis application and provides better cosmetic and functional results.
Future perspectives
Remarkable research efforts on several fronts are ongoing to improve the quality of life of children with peromelia. Efforts have been continuously made to improve mechanics and functionality of myoelectric prostheses (e.g. individually powered digits, wrist extension, forearm rotation) and control improvements (e.g. direct control from the central nervous system or from the peripheral nervous system via targeted re-innervation or neurointegration). 42 However, further research efforts should be directed to underline definitive long-term benefits of prosthetic treatment compared with non-usage with regards to especially compensatory sequelae of the skeletal system. Moreover, prosthetic bone anchoring (so-called osseointegration) is a fast-evolving scientific target.43–45 Despite all disadvantages such as infection and osteomyelitis, new techniques allow for a reliable, stable fixation of external devices to humeral, femoral or tibial bone amputees. However, these techniques have mainly been used for post-traumatic purposes in adults. Nevertheless, osseointegration may well be an alternative option for younger patients in future, since they may especially benefit from the stable fixation to overcome possible rejection of the terminal prosthetic device. Pro- and supination may also be preserved when using an osseointegrated, radius- and ulna-anchored device. However, risks and disadvantages have to be further diminished before these techniques are applied to children, owing to their growing bones.
Moreover, further studies are still required to improve sensory feedback. 46 As the lack of sensibility while wearing a device is one of the key factors for paediatric prosthesis rejections, improved feedback mechanisms will increase the interaction between patient and device, and wearing a prosthesis will result in an experience that is more real. Maximal research efforts should be directed towards conferring sensibility to the prosthetic user. Upper limb allotransplantation might also be a future treatment option for these children as long as toxicity of immunosuppression is reduced. 47