
Abstract
Abstract
Background
The purpose of this prospective study was to assess the impact of cast immobilization on the activities of daily living in children with fractured upper limbs.
Methods
Using the Activities Scale for Kids (ASK), 52 consecutive children (17 girls, 35 boys), aged 5–15 years (mean, 9 years), with upper limb fractures treated by means of above- or below-elbow casts were assessed. The files were reviewed for background and fracture-related data.
Results
Mean score of the above-elbow group was 65.4 ± 15.5 points on the ASK capability domain (ASK-c) (with cast) and 98.7 ± 3 points on the ASK-performance domain (without cast). Corresponding scores for the below-cast group were 89.8 ± 13 and 99.5 ± 2. Factors that positively affected overall function were older age, male sex, shorter duration of pain, and less displacement. On multivariate analysis, only age proved to be a potential predictive factor. Cast position and hand dominance had no effect. The specific activities affected were personal hygiene, dressing, making a snack, and reaching high objects.
Conclusions
To ease their children's adjustment to forearm cast immobilization after fractures, parents should be educated in the areas of daily living that may be affected. This is particularly true for younger children with more displaced fractures that cause more pain.
Keywords
Introduction
Fractures of the upper extremities are very common in children [1–3]. Immobilization in a cast for several weeks may restrain the child from performing many activities of daily living. However, in the medical literature, there has been little attention to the type of activities affected. More knowledge about functional ability during cast immobilization in children with fractures will help both parent and child to cope.
The aim of this prospective study was to assess the impact of cast immobilization for forearm fractures on children's daily activities. The study was conducted after the Institutional Review Board approval was obtained.
Patients and methods
The study sample consisted of 52 consecutive children, aged 5–15 years (mean, 9 years), with closed upper extremity fractures who were treated nonoperatively in our center between March 2005 and May 2006. All children were otherwise healthy, with no cognitive impairment or neurological disorder. Patients with a below-elbow (n = 21) or above-elbow (n = 31) cast were analyzed separately (Table 1).
Fracture types and reductions in children with above-elbow and below-elbow casts
Of the currently available tools for measuring physical function in pediatric orthopedic patients [4–6], we selected the 30-item, self-report Activities Scale for Kids (ASK) [7]. This scale has been tested for validity and was found reliable for evaluating children with various disabilities. Items cover activities done at home, at school, and in the playground [8, 9]. The capability domain of the ASK (ASK-c) measures functioning during immobilization, and the performance domain (ASK-p) measures functioning prior to the fracture. All interviews were conducted by the same physician (B.H.) at 2 weeks after injury to minimize the effect of pain. Data on potential patient- and fracture-related variables affecting functioning—age and sex, side affected, dominant hand, site of fracture displacement, need for reduction and cast position—were obtained from the medical files.
Statistical analysis
Continuous parameters were recorded as means ± standard deviations. The correlation coefficient (r) and the significance for it (P) were calculated in each group for the different variables. To analyze statistically significant differences in mean continuous parameters, the student's t-test was used. A series of multi-variance linear regression models were fitted to the data to identify predictive variables of a higher/lower score. A P value of 0.05 or less was considered statistically significant.
Results
Above-elbow group
The group with above elbow casts consisted of 20 boys and 11 girls aged 6–12 years old (mean age 9.8 years). The left limb was affected in 18 children (58%) and one-third of the children were affected on the dominant side. In 60%, the fractures were displaced. Mean total scores for the patients in an above-elbow cast were 65.4 ± 15.5 on the ASK-c (with cast) and 98.7 ± 3 on the ASK-p (without cast).
Figure 1 shows the significant correlations between the study parameters. In the older children, the fractures were more prevalent in boys (P = 0.04), were more displaced (P = 0.003), and occurred more often in the distal forearm (P = 0.004). It also took more time for the pain to subside (P = 0.01). Fractures in the distal radius were more displaced than shaft fractures (P = 0.004) and were put in neutral position (P = 0.04).
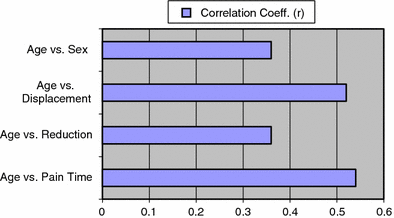
Correlation analysis of parameters for the group with above elbow casts
Below-cast group
The below-cast group consisted of 15 boys and 6 girls aged 6–12 years old (mean age 9.7 years). The left limb was affected in 13 children (62%), and almost half the fractures occurred on the dominant side. In 40%, the fractures were displaced.
Findings for the different variables were similar to those in the above-elbow group (Fig. 2). In older children, fractures were more prevalent in boys (r = 0.42, P = 0.05) and they were more displaced (r = 0.64, P = 0.004). The mean total scores for the patients in a below-elbow cast were 89.8 ± 13 on the ASK-c (with cast) and 99.5 ± 2 on the ASK-p (without cast).
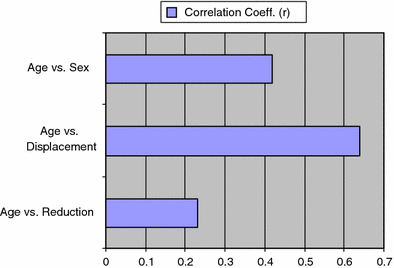
Correlation analysis of parameters for below-elbow-cast group
Whole sample
Overall, higher scores were noted more in boys (P = 0.01), in older children (P = 0.0002), and in those who had pain for a longer period (P = 0.07) (Fig. 3). There was a higher score for distal, displaced, and angulated fractures that needed reduction (P < 0.04). The activities that accounted for most of the differences in scores were personal hygiene, dressing oneself, making a snack, and reaching a high shelf.
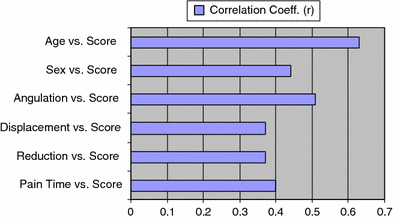
Correlation analysis of parameters and score for both groups
In both groups, writing was difficult for children with fractures on the dominant side (P < 0.005).
Multivariate analysis
Prediction factors entered on the multivariate linear regression model for prediction of the ASK-c score were age, sex, duration of pain (days), fracture site (proximal vs distal), displacement (yes/no), angulation, need for reduction (yes/no), and cast position (neutral, prone, supine). However, the only factor that proved to have a significant contribution was age.
The influence of hand dominance on the ASK-c score between children with casts on the dominant hand and those with casts on the non-dominant hand was tested. Using the student's t-test, no significant influence was found.
Discussion
Our study shows that several activities of daily living are impaired in children with upper limb fractures, particularly in those with above-elbow casts. Therefore, physicians should strive to immobilize distal end forearm fractures in a below-elbow cast when possible [10].
Pain is known to affect daily living activities [11]; thus, to minimize its effect on the ASK score, we conducted the study 2 weeks after immobilization, when the self-reported pain had subsided in most cases.
In older children, fractures were more prevalent in boys and occurred mainly in the distal forearm. Although it took more time for the pain to subside in the older children, they had higher scores than younger children. However, on multivariate analysis to identify predictive factors for the ASK-c, only age remained significant. Neither cast position nor hand dominance was contributory.
The main functions affected were personal hygiene, self-dressing, making a snack, and reaching a high shelf. Some of the problems encountered have simple solutions, such as covering the cast with a plastic bag during bathing to improve hygiene [12]. Therefore, greater awareness of these limitations and improved parental education by the attending physician for when the child is immobilized with a cast are important.
Previous studies have shown that children with upper limb fractures are absent from school for a few days [13, 14]. A letter by the attending physician to the child's teacher explaining the situation could make the child's adjustment at school much easier [14].
Conclusion
In conclusion, immobilization with a cast interferes with daily living activities. Discussing the limitations with the parents and children will improve management.