
Abstract
Purpose:
The British Orthopaedic Association Standards for Trauma-4 includes pediatric Gustilo–Anderson type I upper limb open fractures and recommends surgical debridement as the preferred method of treatment. The reported incidence of fracture-related infection is low in patients with this injury pattern and the evidence supporting debridement is therefore weak. The aim of this systematic review is to compare infection rates between non-operative management and operative debridement in children with Gustilo I upper limb fractures who did not require surgical fixation.
Methods:
A systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Eligibility criteria included patients <18 years with Gustilo–Anderson type I upper limb fractures managed with either antibiotics alone or with operative debridement. Patients in whom the fracture was stabilized were excluded, and the Risk Of Bias In Non-randomized Studies—of Interventions tool was used to evaluate bias.
Results:
Eleven, predominantly retrospective studies were identified, involving 537 patients with fractures including 466 forearm, 70 wrist, and one humerus. A non-operative management strategy was used in 293 patients with one superficial infection (0.3%). Operative debridement was used in 244 patients with one superficial infection (0.4%).
Conclusion:
The optimal management of Gustilo–Anderson type I pediatric upper limb fractures is unclear. Based on the current evidence base, surgical debridement does not appear to reduce the rate of infection. The decision to manage these injuries aggressively should therefore be individualized to consider patient age, mechanism, and clinical extent of injury.
Level of evidence:
level II.
Introduction
Open fractures communicate with the external environment 1 and are generally treated emergently to prevent wound contamination and infection. 2 Classification systems from the Orthopaedic Trauma Society (OTS), the Orthopaedic Trauma Association—Open Fracture (OTA-OFC), and the Ganga classification attempt to classify these injuries.3 –6
Gustilo et al. 7 stratified these injuries into three distinct types, based on mechanism, location, soft tissue damage, fracture pattern, and degree of contamination. This classification remains in common use and is of value in predicting infection.7,8
Injuries with a wound <1 cm, with minimal contamination or soft tissue involvement are classified type Ι.9 –11 The rate of infection in pediatric patients with this injury pattern is lower than their adult counterparts12,13 particularity in the upper limb, and a thicker, vascularized periosteum may be a contributory factor.12,13
The British Orthopaedic Association Standards for Trauma (BOAST-4) considers an evidence base that is predominately derived from lower limb injuries and extrapolates this to include the upper limb,14 –16 recommending operative debridement and intravenous (IV) antibiotics in all cases, irrespective of patient age and fracture site.14 –16 There is a paucity of evidence that considers open fracture management and the relevance of the BOAST-4 in the pediatric population. The aim of this study was to examine the available published evidence to compare infection rates of non-operative management with operative debridement within this population and therefore evaluate the relevance of BOAST-4 to children with upper limb open fractures.
Material and methods
A systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the study was prospectively registered on PROSPERO: International prospective register of systematic reviews (Registration Number: CRD42023465576).
The literature search was conducted separately by two authors (OO) and (SH) and included OVID Medline, EMBASE, Cochrane, OrthoSearch, and Web of Science. These databases were systematically searched from inception until 13 December 2023, not limited by language with search terms: (pediatric or child or adolescent or teen or youth or toddler or baby or neonate) AND (Gustilo–Anderson or Open fracture) AND (upper limb or shoulder or clavicle or humerus or elbow or olecranon or radius or ulna or wrist or forearm).
All potentially relevant studies were initially screened based on title and abstract. Randomized controlled trials (RCTs), retrospective and prospective cohort studies, and case–control studies involving patients <18 years with Gustilo–Anderson type Ι upper limb fractures, managed with antibiotics ± emergency room debridement, formal operative debridement, or both were eligible for inclusion. Patients who underwent internal fixation were excluded. Full-text articles were selected for further consideration and data extraction by OO and SH with any disagreements resolved by consensus and with YG.
The Risk Of Bias In Non-randomized Studies—of Interventions (ROBINS-I tool) 17 was used by OO to assess the methodological quality of individual studies in seven domains 17 and arbitrated as required by (YG). The information that was recorded included publication date, author, country of origin, level of evidence, gender, mean age and range, total number of grade Ι upper limb fractures and their location, and length of follow-up.
The primary outcome measure was defined as the rate of infection. This was assessed in patients managed with formal debridement (operative group) or with antibiotics alone ± emergency room debridement (non-operative group). Additional information included plastic surgery input, use of oral/intravenous (IV) antibiotics, time from injury to first dose of antibiotics, and the length of antibiotic course.
Results
The initial search identified 1633 studies, of which 1537 were excluded on the basis of title and abstract. Ninety-six studies were suitable for full-text review and 11 studies were included in the final review based on the eligibility criteria (Figure 1). Ten retrospective and one prospective cohort study provided a total population of 537 fractures located in the forearm (n = 466), wrist (n = 70), and humerus (n = 1) (Table 1).
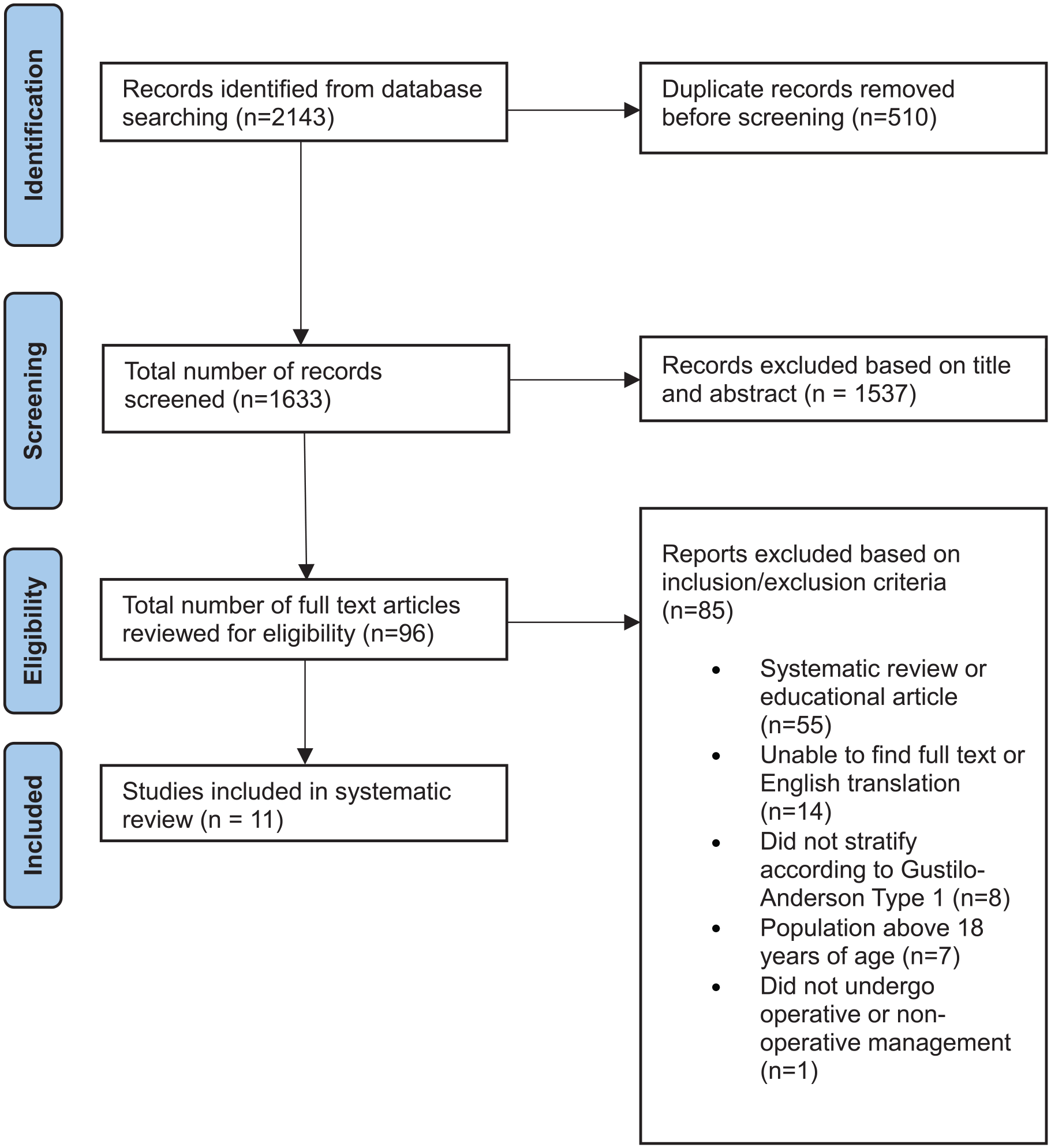
PRISMA flow chart illustrating the search strategy.
Study characteristics.
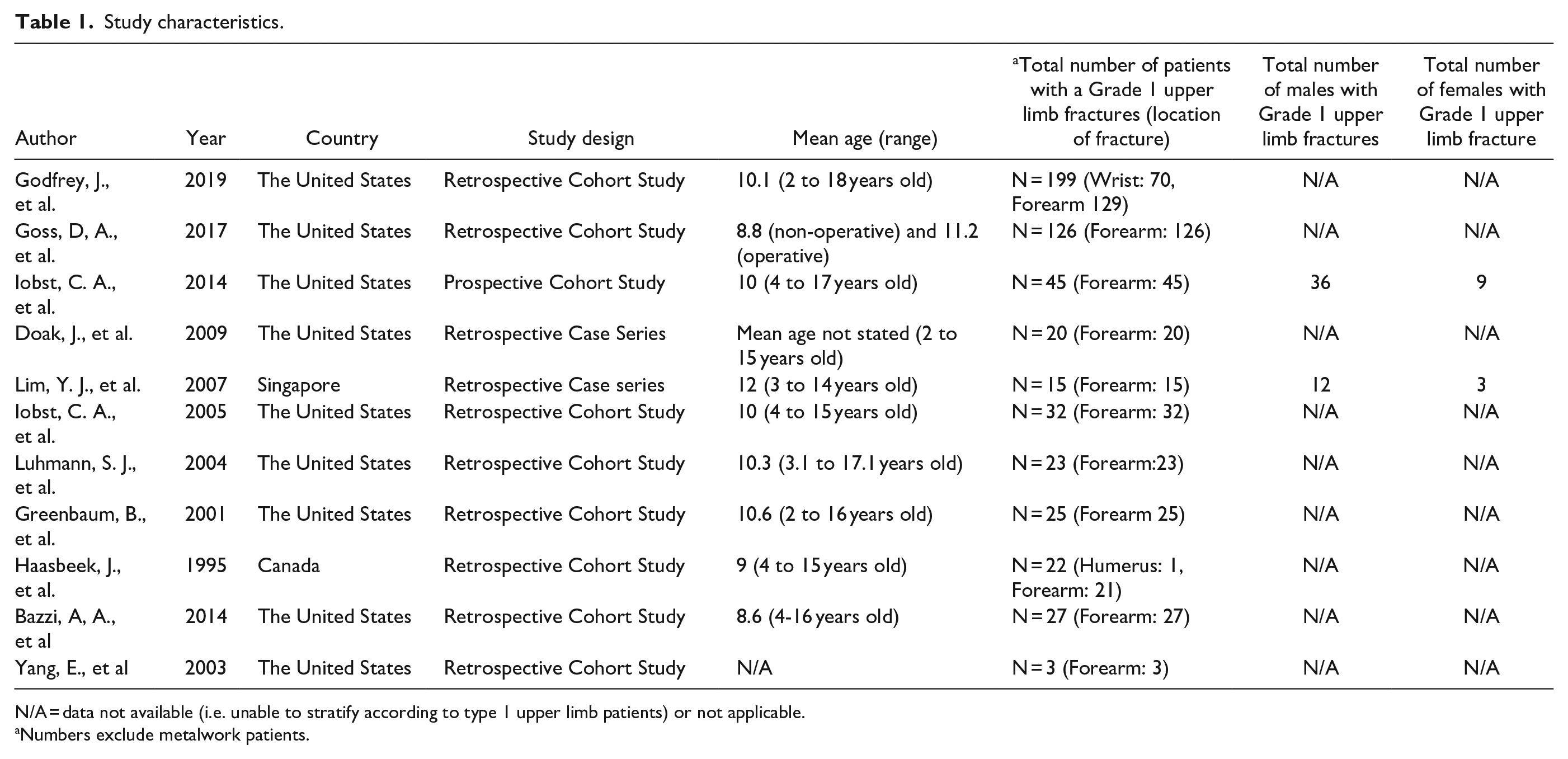
N/A = data not available (i.e. unable to stratify according to type 1 upper limb patients) or not applicable.
Numbers exclude metalwork patients.
The ROBINS-I tool 17 considered that all studies were either moderately or severely impaired with no studies considered to be methodologically sound. This was generally due to retrospective studies, often with missing patient data and outcomes (Figure 2).
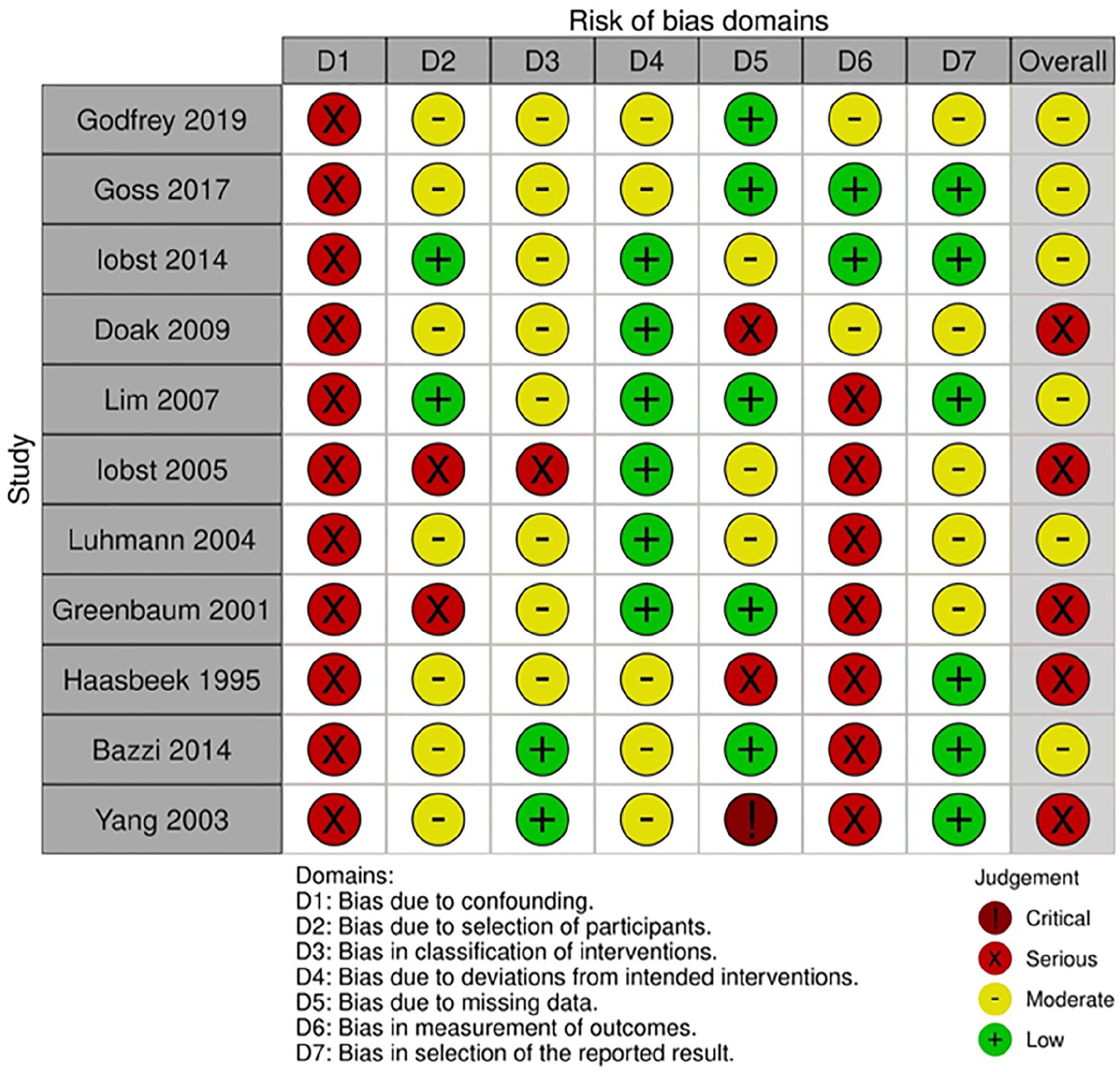
ROBINS-I risk of bias assessment.
The weighted mean age was 10 (range = 2–18) years, with a range of follow-up between 4 weeks and 13 years (Tables 1 and 2). One study did not report participant age 18 and sex distribution was limited to two studies19,20 (Table 1).
Details of intervention.
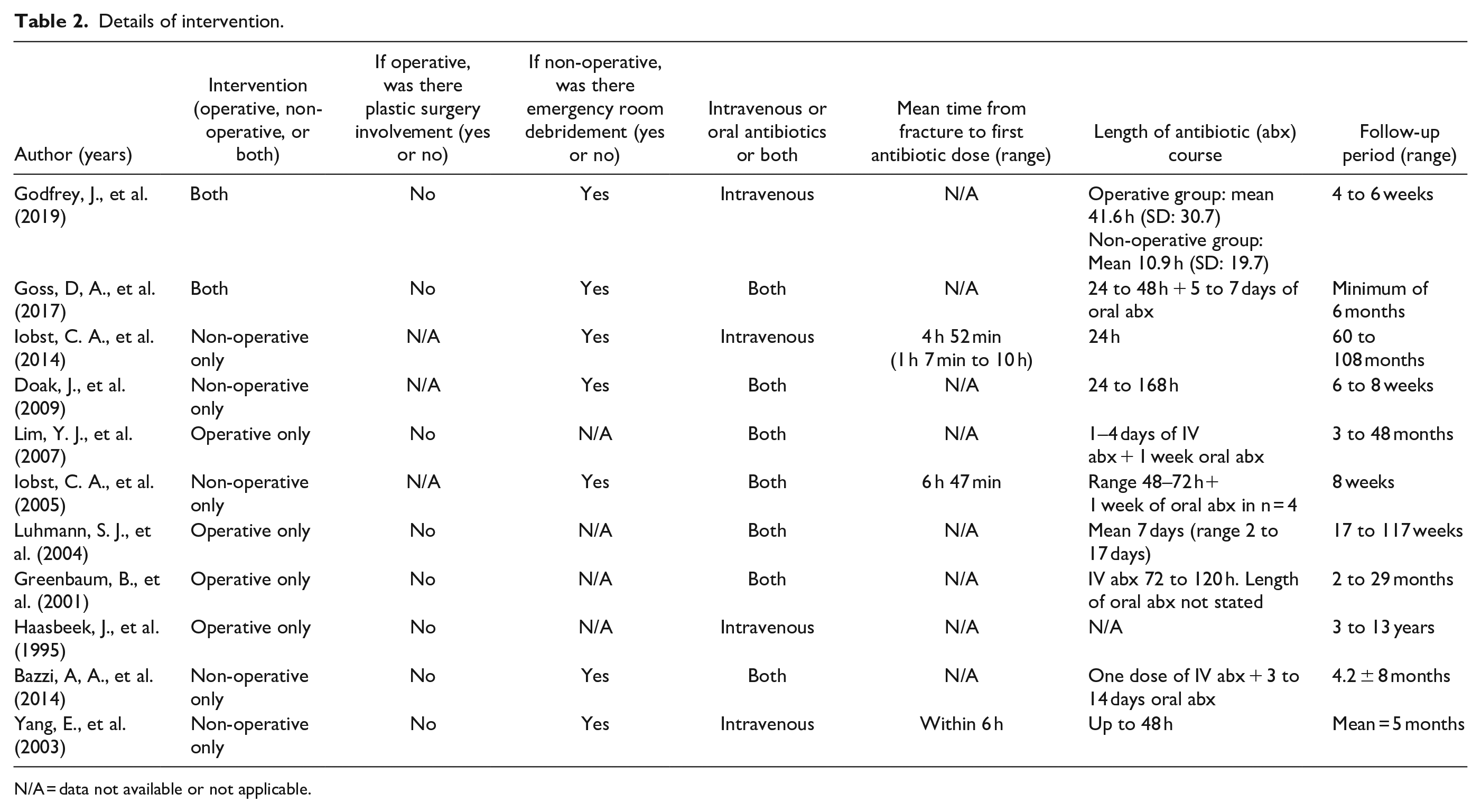
N/A = data not available or not applicable.
Non-operative management in isolation was considered in five studies,18,19,21 –23 operative management in isolation in four studies,10,11,20,24 and two studies considered patients managed either non-operatively or operatively.25,26 All studies reported using a course of IV antibiotics, with a weighted mean duration of 44 h (range = 24–168), and seven studies implemented an additional course of oral antibiotics.10,20 –24,26 Only three studies reported the interval between injury and first antibiotic dose, with a weighted mean of 5 h 41 min (range = 4 h 52 min to 6 h 47 min).18,19,22 Debridement in the emergency room combined with IV antibiotics was utilized in seven studies,18,19,21 –23,25,26 and none reported plastic surgical involvement (Table 2).
Infection was reported in one patient managed with formal operative debridement (n = 1/244, 0.4%) 10 and in one patient managed non-operatively (n = 1/293, 0.3%) 25 (Table 3). The infection in the non-operative group occurred in a 10-year-old patient who presented with a superficial wound infection 4 days after initially being treated and discharged with IV antibiotics and emergency room wound irrigation. 25 He was subsequently managed with operative debridement and went on to achieve satisfactory fracture healing with an otherwise uneventful clinical course. 25
Rates of infection.
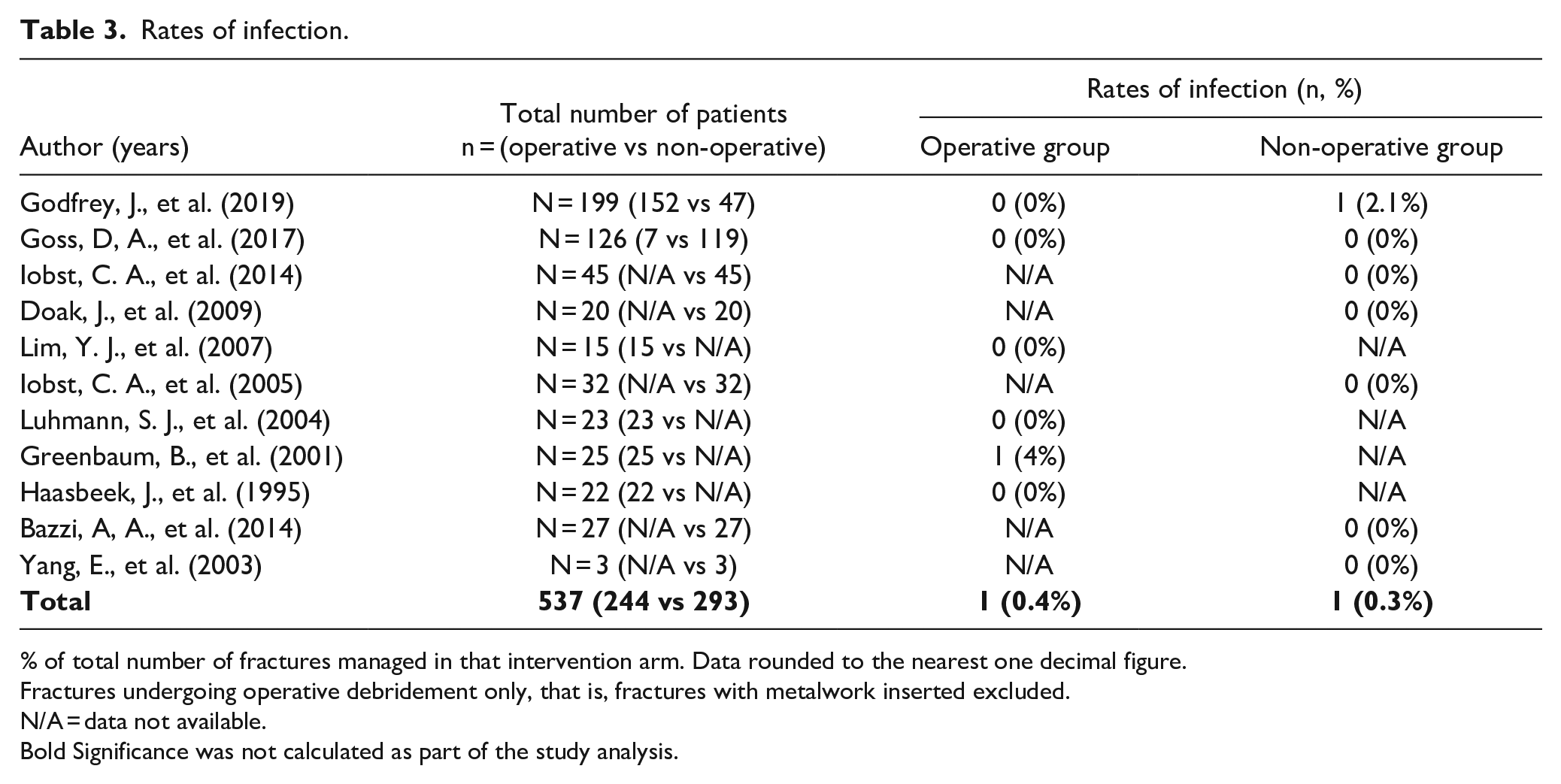
% of total number of fractures managed in that intervention arm. Data rounded to the nearest one decimal figure.
Fractures undergoing operative debridement only, that is, fractures with metalwork inserted excluded.
N/A = data not available.
Bold Significance was not calculated as part of the study analysis.
In the operative debridement group, one superficial wound infection was noticed in a 12-year-old boy 6 weeks after initial operative debridement. 10 Notably, at the time of operative debridement, cultures grew Staphylococcus epidermidis, and this patient was initially treated with a 5-day course of parenteral antibiotics of, compared to the 3 days for other patients included in the study. 10 The superficial infection that developed 6 weeks later was treated with an further course of 4 days of intravenous and 10 days of oral antibiotics. 10
Complications in the operative group (n = 30) included wrist stiffness (1), 25 loss of reduction (13),10,20,24 refracture (3),20,24,26 malunion (4),24,25 delayed union (4),24,25 temporary ulnar neuropathy (3),10,25 anterior interosseous neuropraxia (1), 10 and combined superficial radial and median nerve injury (1). 10 Complications in the non-operative group (n = 33) included loss of reduction (21),19,25,26 refracture (10),19,21,26 delayed union (1), 23 and a retained foreign body (1) 23 which was identified 4 weeks later and was removed in clinic with no evidence of a resultant infection. 23
Discussion
BOAST guidelines recommend operative debridement and IV antibiotics in all open fractures irrespective of patient age and fracture site.15,16 These guidelines are from an evidence base that is predominately derived from adult lower limb injuries, extrapolated to include the upper limb.27,28
To the authors’ knowledge, this is the first systematic review that compared non-operative management with operative debridement in pediatric Gustilo–Anderson type Ι upper limb fractures. The review identified comparable rates of infection between operative debridement and non-operative groups with a very low overall rate. In addition, complication rates were similar in both groups and were rarely associated with the soft tissue component of the injury. Only one complication was a result of the intervention and involved a retained foreign body following non-operative fracture management. 23
BOAST-4 guidelines may therefore be unnecessarily invasive, when blindly applied to a pediatric population with this injury pattern. 29 The poor quality of available evidence limits the ability to reach robust conclusions and challenge conventional wisdom, and it is therefore recommended that each case is considered on an individual basis with management based on age, mechanism of injury, level of contamination, and any other relevant clinical considerations.
Conclusion
Based on the limited current evidence base, surgical debridement of Gustilo I upper limb fractures in a pediatric population has the same infection rates as not performing a surgical debridement and the BOAST-4 guidelines may be excessive for this specific subgroup. Treatment should be considered on an ad hoc basis, and a level 1 study is the recommended next step to identify the optimal treatment.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241262973 – Supplemental material for Initial management of pediatric Gustilo–Anderson type I upper limb open fractures: Are antibiotics enough?
Supplemental material, sj-pdf-1-cho-10.1177_18632521241262973 for Initial management of pediatric Gustilo–Anderson type I upper limb open fractures: Are antibiotics enough? by Olufemi Olatigbe, Sabba Hussain, Anna Bridgens, Caroline Hing, Fergal Monsell and Yael Gelfer in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors thank the NHS librarian team at St George’s Hospital. In particular, Ayo Ogundipe and Karen John-Pierre for their assistance in ensuring that a robust literature search was conducted.
Author contributions
O.O. (primary author) took the lead in the design, methodology (including the literature search), data extraction, and implementation of the research. He also drafted the manuscript and designed the tables and the figures. S.H. (secondary author) assisted O.O. in the drafting of the manuscript and the design of the tables and figures. She also performed the secondary literature search and separately corroborated the data extraction. A.B., C.H., F.M., and Y.G. conceived of the presented idea. A.B. also contributed to the design of the study. F.M. and Y.G. both also contributed in providing critical feedback which helped to shape the research, analysis, and the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors request that the following individuals not be approached to review our manuscript as they are listed as co-authors: Ms Y.G., BSc, MD, PhD, St George’s University Hospitals NHS Foundation Trust, London, UK and Mr F.M., MBBChB, MSc, PhD, University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, UK.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.