
Abstract
Abstract
Purpose
The purpose of this study is to report the number of children from a total population of children with cerebral palsy (CP) in Scotland who had a displaced or dislocated hip at first registration in a national surveillance programme.
Methods
Migration percentage (MP), laterality, Gross Motor Function Classification System (GMFCS) level, CP subtype, distribution of CP and age were analyzed in 1171 children. Relative risk was calculated with 95% confidence intervals. Hip displacement and dislocation were defined as a MP of 40 to 99 and > 100 respectively.
Results
Radiographs were available from the first assessment of 1171 children out of 1933 children registered on the system. In all, 2.5% of children had either one or both hips dislocated (29/1171) and dislocation only occurred in children of GMFCS levels IV and V. A total of 10% of children had a MP 40 to 99 in one or both hips (117/1171). An increasing GMFCS level was strongly associated with an abnormal MP. Hip dislocation was unusual in patients under the age of seven years. A MP of 40 to 99 was not seen in children with isolated dystonia. Displacement was more frequent in children with bilateral involvement and dislocation was only seen in spastic and mixed tone groups.
Conclusion
This data gives an overview of the number of CP children who have hip displacement/dislocation in Scotland and who will possibly require surgery.
Level of Evidence
I
Introduction
There is a well-recognized linear relationship between the risk of hip displacement with increasing Gross Motor Function Classification System (GMFCS) level in children with cerebral palsy (CP). The incidence of hip displacement is about 0% for children at GMFCS level I and about 90% for those at GMFCS level V.1–4 Dislocation is often painful and also causes difficulties with seating and access for perineal hygiene.
The Quality Registry for Children with Cerebral Palsy (Uppföljningsprogram för Cerebral Pares, CPUP) has been running for over 20 years in Sweden 5 and has attracted international recognition for its work. Similar surveillance programmes have been introduced in Australia, 6 Norway, 7 Denmark and Iceland. In Sweden the incidence of hip dislocation in children with CP was reduced from about 8% to less than 1% after the introduction of the surveillance programme. 8
Historically in Scotland there was no nationally agreed approach to evaluating the hip in CP, particularly in children known to be at high risk of hip displacement. Referral patterns to children's orthopaedic surgeons varied 9 and generally management of the children was reactive rather than proactive. Thus in 2013 a surveillance programme, the Cerebral Palsy Integrated Pathway Scotland (CPIPS), which is closely based on the CPUP, was introduced in all Scottish Health Boards. This provides equity of access for children with CP aged two to 16 years to an agreed system of physical examination of the lower limbs and spine by paediatric physiotherapists and pelvic radiography overseen by children's orthopaedic surgeons. 10
The purpose of this paper is to report on hip displacement in the total population of children with CP aged two to 16 years in Scotland at their first registration by the CPIPS to give an indication of the likely future surgical workload for these children.
Methods
Children registered on the CPIPS have to be aged between two to 16 years and have a diagnosis of CP made by a consultant paediatrician, neuro-paediatrician or community paediatrician to be included. Their age at first registration varied according to when a definitive diagnosis of CP was made. CP subtypes were classified according to the Surveillance of Cerebral Palsy in Europe recommendations. 11
The technique for positioning children for pelvic radiography has been standardized in Scotland 12 and displacement is measured using the migration percentage (MP). 13 Hip radiographs of children with CP are arranged according to a nationally agreed protocol for the frequency of radiological examination of the hip and this is shown in Table 1. The normal MP is widely accepted to be < 33 and the MP for a dislocated hip is 100. Radiographic data is uploaded into a secure, central database and clinical decision-making is based on a traffic light system for the MP values (green < 30, within a normal range, amber 30 to 40, red > 40).
Pelvic radiography protocol by age and Gross Motor Function Classification System (GMFCS) level. Dark grey represents all GMFCS levels, mid-grey GMFCS levels III to V, light grey as indicated clinically

The MP from the child's first hip radiograph as part of the CPIPS programme was analyzed along with the following: age, laterality, GMFCS level, CP subtype and neurological distribution of CP. For the purposes of this report, we considered a hip dislocation as a MP > 100 and hip displacement as a MP > 40 and < 100. The analysis took place at one time point and analysis is reported for all children two to 16 years old at first registration.
Data analysis was undertaken using GraphPad Prism version 7.00 for Windows (GraphPad Software, www.graphpad.com, La Jolla, California). Student's t-test was used to compare continuous parametric data between groups. Correlation was calculated using Pearson's correlation coefficient. A p-value < 0.05 was defined as statistically significant. Relative risk was calculated with 95% confidence intervals. For categories with 0 patients, 0.5 was added to each cell in the contingency table to facilitate the calculation.
Results
A total of 1933 children were registered in the system at the time of analysis in January 2018, giving a prevalence of 2.25 cases per 1000 children aged two to 16 years in Scotland and representing around 95% of the CP paediatric population of Scotland. Not all 1933 children had a pelvic radiograph at first registration because this was not indicated according to the radiological protocol.
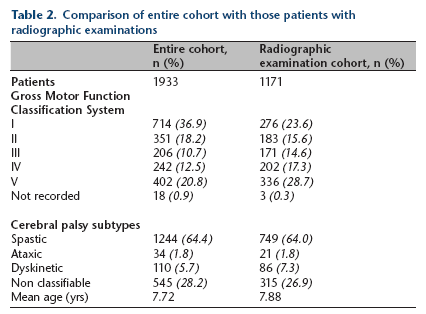
The MP data (from radiographs taken at their first measurement in CPIPS) from 1171 children aged between two to 16 years were examined for this study. The characteristics of these children and those of the entire cohort of 1933 children are shown in Table 2. There was no significant difference in hip displacement/dislocation between the left and right hips and a strong correlation between the right and left hips in individual patients (Pearson's r = 0.63, p < 0.01).
Comparison of entire cohort with those patients with radiographic examinations
Hip dislocation, MP > 100
The percentage of children from the total population with either one or both hips dislocated was 2.48% (29/1171) and only occurred in children at GMFCS levels IV and V. The percentage of hips dislocated out of the total hips was 1.92% (45/2342, bilateral in 16 children, six left and seven right hips). In the GMFCS IV to V population 5.39% of children had either one or both hips dislocated (29/538). The percentage of hips dislocated in these two levels was 4.18% (45/1076). When GMFCS levels III to V were considered, the percentage of children with either one or both hips dislocated was 4.09% (29/709) and the percentage of hips dislocated in these three groups was 3.17% (45/1418).
Hip displacement, MP 40 to 99
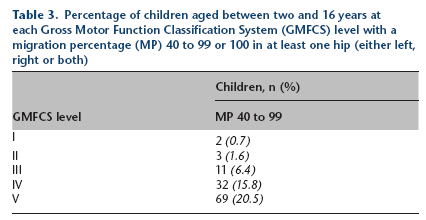
In all, 9.99% of children (117/1171) had a MP between 40 and 99 in one or both hips, 5.81% of hips (136/2342). A total of 19 children had a MP between 40 and 99 in both hips, 46 had a MP between 40 and 99 in only the left hip and 52 a MP between 40 and 99 in only the right hip. It was found that an increasing GMFCS level was strongly associated with a MP > 40 (Fig. 1 and Table 3).
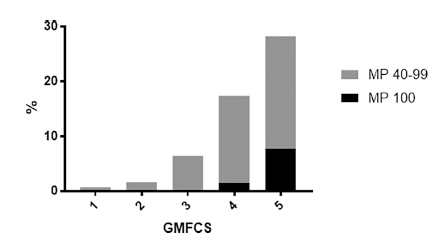
The percentage of children, aged two to 16 years at each GMFCS level with at least one displaced or dislocated hip (1 = GMFCS I, 2 = II, 3 = III, 4 = IV, 5 = V).
Percentage of children aged between two and 16 years at each Gross Motor Function Classification System (GMFCS) level with a migration percentage (MP) 40 to 99 or 100 in at least one hip (either left, right or both)
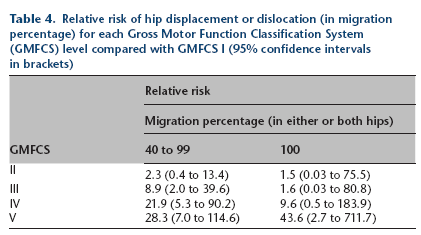
Radiographic hip dislocation (MP >100) was unusual in patients under the age of seven years. Hip displacement and dislocation according to age is shown in Figure 2. The relative risk of hip displacement for GMFCS levels II to V compared with GMFCS level I (as a baseline) is shown in Table 4. Figure 3 shows hip displacement and dislocation according to CP subtype and Table 5 shows the same according to the neurological distribution of CP.
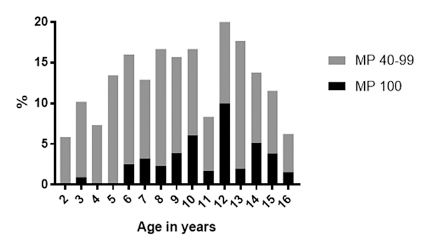
The prevalence of hip displacement or dislocation, of at least one hip, in children of each age between two and 16 years.
Relative risk of hip displacement or dislocation (in migration percentage) for each Gross Motor Function Classification System (GMFCS) level compared with GMFCS I (95% confidence intervals in brackets)
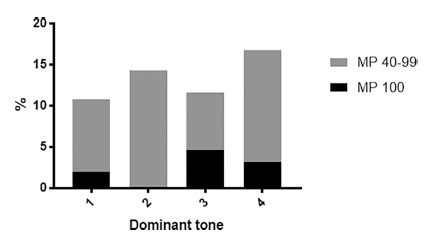
Hip displacement and dislocation, of at least one hip, according to the Surveillance of Cerebral Palsy in Europe (SCPE) classification (1 = spastic, 2 = ataxic, 3 = dyskinetic, 4 = mixed, unclassifiable).
Hip displacement and dislocation of at least one hip according to neurological distribution. Data represented as n (%)
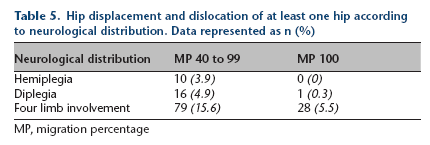
MP, migration percentage
Discussion
This study provides data on hip dislocation and displacement in a cross-sectional analysis of a total population of children with CP in Scotland where this information has not previously available in the United Kingdom. Before the introduction of the programme only children who were referred were monitored in clinics and radiographs were taken according to their clinical needs and managed accordingly. However, there was no consensus as to the frequency of clinical and radiological examinations according to GMFCS levels. The introduction of the programme in 2013 enabled a consistent, nationally agreed approach to the musculoskeletal management of children with CP, according to defined protocols. Thus, our findings are not all from an untreated population of children, and the radiographic data presented in this study, representing their first measurement within the CPIPS registry, may be considered a ‘control’ sample of patients not previously subject to surveillance. Children aged between two and 16 years were registered by the CPIPS, unlike selected age groups at first registration in the Scandinavian systems.
From the prevalence of CP in the United Kingdom and the number of live births in Scotland we are confident that 95% of the population with CP aged between two and 16 years have been registered with the CPIPS. The figure of 95% takes into account children who have been diagnosed with CP but who are not yet registered in the CPIPS or whose families have declined registration, which has been rare.
Hip dislocation MP > 100
A smaller sample study showed that about 8% of children in Southern Sweden had a dislocated hip before the introduction of the CPUP. 7 The percentage of patients with dislocated hips from the total CP population in Scotland at 2.48% was lower than the pre-surveillance figures from Sweden and Norway. However, these figures may not be directly comparable as the Scottish data are cross-sectional and younger children, particularly those at GMFCS level V, who were registered at the initial stages of CPUP in Sweden would have been at increased risk of lateralization of the hip over time.
Elkamil et al 7 reported hip dislocation in a sample of the Norwegian population before the introduction of the Norwegian equivalent of CPUP (CPOP). In all, 15.1% of children at GMFCS levels III to V had a dislocated hip which in the total sample (GMFCS I to V) of 357 is equivalent to 5% of this population. Dislocation was not seen in GMFCS level III children in the present study but 5.26% of Scottish children of GMFCS levels IV to V had either one or both hips dislocated at first registration.
The present study also shows the relative risk of hip displacement for GMFCS levels II to V compared with level I (Table 4) and this confirms the validity of this relationship from previous reports.1,2 Furthermore, dislocation was unusual before age seven years, which was also reported by Rang et al 14 (Fig. 1).
Hip displacement MP 40 to 99
The threshold of a MP > 40 is considered clinically significant as Hägglund et al 8 reported that several hips with a MP between 33 and 40 returned to normal levels without surgery. However, in that study, no hip with a MP exceeding 42 returned to normal without surgery. At the introduction of CPIPS 9.99% of children (145/1203) had a MP > 40 at first registration. Some children may have had previous hip surgery before registration in CPIPS but have been included in the overall analysis because a MP > 40% is clinically significant and may trigger further surgical management of the hip.
There is an increasing awareness of hip displacement in hemiplegic CP, 15 particularly in children with Type 4 hemiplegia. 16 In all, 4% of children with Type 4 hemiplegia had a displaced hip at first registration into the CPIPS even though they were at GMFCS levels I or II (Table 5). The protocol for frequency of pelvic radiography for Type 4 hemiplegics in the CPIPS radiological protocol has since been amended to include an additional pelvic radiograph at age ten years as a direct consequence of the CPIPS.
Neurological classification and distribution of CP
Tone influences hip displacement and data from the dominant tone patterns showed that a MP > 40 was not seen in children with isolated dystonia (Fig. 3). However, hip displacement was seen in spastic, ataxic, dyskinetic and mixed tone groups. Dislocation was only seen in spastic and mixed tone groups underlining the rationale for spasticity reduction as part of the management of hip displacement. Unsurprisingly, displacement was more frequent in children with bilateral involvement.
The first limitation of this study is that radiographs were only taken at enrolment into the programme if the protocol, according to age and GMFCS level, required a radiograph at that time. Whilst it may have been desirable for research purposes for all children to have a hip radiograph at enrolment, this was not done because of the nationally agreed protocol for pelvic radiography for children with CP and to minimize radiation exposure; thus the data should be interpreted with caution. Second, the data analyzed does not yet demonstrate the effect of hip surveillance on children with CP in this population although it does inform clinicians of the number of children with a displaced or dislocated hip at first registration. Third, the programme does not currently inform clinicians of the most effective management of the displacing hip. Currently children's orthopaedic surgeons involved in the programme have autonomy over clinical and surgical management of their patients but any lower limb surgical procedure performed is registered and therefore recorded prospectively in the CPIPS. We anticipate that over time it will be possible to determine the timing and optimal treatment for a displacing or dislocated hip as more surgical data accumulates.
This type of data on hip displacement in children with CP in Scotland has not been previously reported. It has the potential to inform future orthopaedic provision for the most common childhood long-term disability, as well as guide healthcare funders on the needs of this population. Only by collecting long-term prospective data may it be possible to determine optimal timing of surgery, within the overall management of the child, to prevent hip dislocation and to minimize the risk of re-displacement during their growth.
Footnotes
Acknowledgements
We gratefully acknowledge the contributions of all clinicians who have or continue to provide data on their patients for CPIPS. We are grateful to the Scottish Government, The Robert Barr Trust and Brooke's Dream for the funding to set up CPIPS and to Edinburgh Children's Hospital Charity, for continuing funding.