
Abstract
Abstract
Purpose
Paediatric hand injuries are a frequent reason for acute medical evaluation. Previous studies have reported only fracture rates, surgical injuries or are limited to database diagnosis coding. The average fracture rates and injury distributions across the hand for all mechanical injuries have not been well-described.
Methods
We performed a retrospective review of all emergent/urgent care visits over 18 months at a US paediatric tertiary hospital with hand injuries recorded anywhere in the encounter. Patient, injury and encounter details were recorded with additional imaging review, categorized and described.
Results
A total of 523 patient visits (0.64% of all encounters) were for mechanical hand trauma. The injury mechanism was 42% crush, 19% jammed, 12% impact, 12% fall on outstretched hand, 7% hyperextension and 8% other/unclear. Crush was responsible for 80% of injuries in patients aged 0 to six years old but only 17% in patients aged 13 to 18 years. Crush resulted in fractures only 26% of the time, while other mechanisms were more likely to fracture (33% to 87%). Border digits were injured more often than others (21% to 23% versus 13% to 17%), and were most commonly fractured in the proximal phalanx (57% to 67% versus 22% to 34% for non-border digits). Providers correctly coded for basic fracture presence in 89.1% of injuries, but 53% of codes were not finger or laterality-specific, and only 15% specified a bony segment demonstrating that International Classification of Diseases-9 coding was nonspecific for injury patterns.
Conclusion
Patients with paediatric hand injuries frequently utilize emergency care and understanding the basic patterns of injury can guide resource utilization and future studies on optimal treatment algorithms in this setting.
Level of Evidence
IV, Prognostic, Case Series
Keywords
Introduction
Paediatric finger and hand trauma are common causes for evaluation in an urgent or emergency care setting. Hand fractures represent some of the most common fractures of childhood.1,2 While most hand injuries do not represent fractures, and even fewer require surgical intervention, these visits consume significant healthcare resources. Most acute hand trauma undergoes radiographic evaluation, while only a portion lead to subspecialty referral. The estimated fracture rate ranges widely from 16% to 65%.3–6
Most previous studies are restricted to patient subgroups such as only those with fractures,1,2,7–12 those referred for subspecialty evaluation6,11–13 or those undergoing surgery.6,14 The few studies looking at all-comers to acute care environments are dependent on large International Classification of Disease (ICD) 15 -coded databases that lack finger-specific details or have focused on injury environment and less on the types of injury.4,5,8 This strategy can have serious inherent flaws as relying on ICD codes will limit accuracy and fail to provide many injury-specific mechanism and anatomical details16–18
The purpose of this study was to examine the characteristics of all presenting mechanical finger injuries to a tertiary referral hospital's emergency department and urgent care clinics. By evaluating each of these patients with detailed chart review instead of simply ICD code review, the goal is to better understand demographics, relative injury and fracture rates, delays in presentation and coding accuracy. We also hope to identify injury patterns more or less likely to result in fracture across different ages, genders and mechanisms as a baseline for future work to help in resource utilization for primary care providers who may not all have specialized imaging or subspecialty care available at their centres.
Materials and methods
This is a retrospective chart review of all visits to a major US paediatric tertiary referral hospital's emergency room and urgent care clinics (Seattle Children's Hospital group, Seattle, Washington) over a period of 18 months (29 June 2012 to 31 December 2013). This hospital serves a local paediatric population of nearly one million, with a larger network of about 2.4 million, resulting in approximately 430 000 annual visits. After Institutional Review Board approval, all visits during that period with a chief complaint, reason for visit or ICD code of finger or hand injury were selected. We identified 568 unique visits; 45 were excluded for age over 18 years, simple lacerations, non-traumatic infections, return visits and congenital abnormalities. The remaining 523 visits underwent review to identify age, gender, injury laterality, finger segment(s), mechanism, delay from injury to presentation, whether subspecialty consultation was obtained and the prescribed follow-up as well as ICD codes assigned to the visit. All imaging underwent review by a senior orthopaedic resident (first author RFG) to identify possible discrepancies from radiology reports, which were subsequently resolved by an attending paediatric hand surgeon (senior author SES). For each visit, injuries to multiple fingers were counted as individual injuries, resulting in a total of 570 injuries for analysis.
Mechanism was divided into the following categories: crush, fall on outstretched hand (FOOSH), hyperextension, jamming (axial loading to the tip of the finger), direct impact and other/unclear. Children were grouped by age: 0 to six, seven to 12 and 13 to 18 years old. Metacarpal fractures were attributed to ‘hand’ injuries instead of the individual finger. Provider-assigned ICD diagnosis codes were compared with official radiograph reports and our individual chart and imaging review.
Data points were collected in a de-identified database for analysis. Chi-squared analysis was performed on categorical data. Significance was assigned at p ≤ 0.05.
Results
Over 18 months, 0.64% (523) of 81 575 paediatric urgent/emergent care visits were for hand complaints. After excluding nontraumatic complaints and evaluating injured digits individually, we identified 570 injuries for analysis. The mean age of presenting patients was 9.34 years old (5 months to 18 years), 43.6% of patients were female, and the fracture rate was 40.7%. Subdividing injuries by age and gender revealed a bimodal distribution (Fig. 1). Gender spread was similar across ages 0 to six years (47.1% female) and seven to 12 years (49.8% female), but after age 12 years, boys presented more often (30.6% female). Fracture rates varied, with girls having double the boys’ rate in the youngest bracket (Table 1).
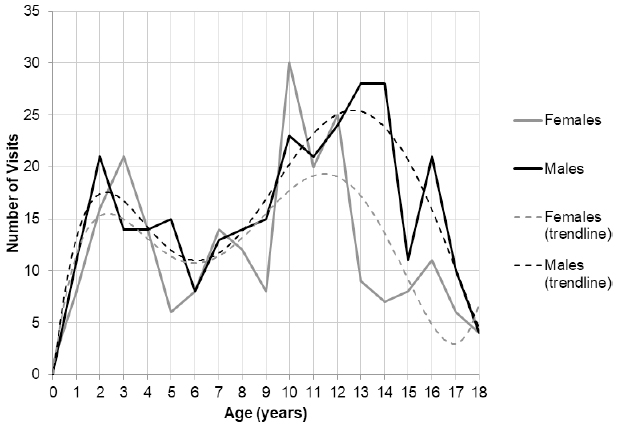
Injury age distribution by gender with trendlines.
Injury and fracture rate by gender and age bracket
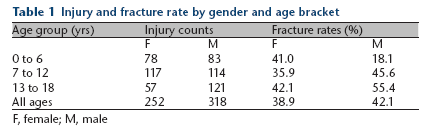
F, female; M, male
Injury rates from different mechanisms also varied by age and gender. Crushing mechanisms accounted for 80.1% of injuries ages 0 to six years, but only 17.4% of injuries at ages 13 to 18 years. Direct impact and jamming injuries were rare in younger children, but common in older children (Table 2).
Injury mechanism as percentage of total injuries per age group

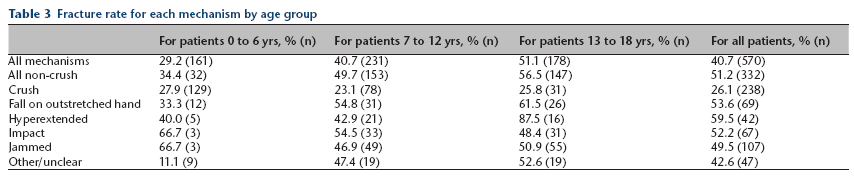
The fracture rate relationship with age was investigated across mechanisms (Table 3). Overall, younger patients had lower fracture rates, predominated by crushing injuries. Across all ages and within each age bracket, crush injuries had a significantly lower fracture rate than all other mechanisms (26.1% versus 51.2%, p = 0.0001). Hyperextension injuries in teenagers had the highest fracture rate of 87.5% of any group.
Fracture rate for each mechanism by age group
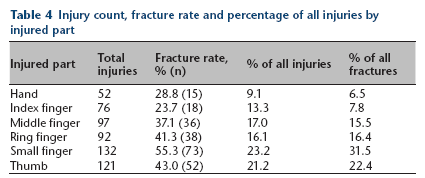
Evaluating injury and fracture distribution across the hand demonstrated that the small finger and thumb were the most commonly injured at 21.2% and 23.2% of all injuries, and most likely to be fractured with 43% and 55.3% fracture rates. The index finger had the lowest injury and fracture rates, with just 13.3% of injuries, and a 23.7% fracture rate (Table 4). Considering bony segments, the thumb and small finger were more likely to fracture at the proximal phalanx, whereas the middle and ring finger were more likely to fracture the distal phalanx (Fig. 2). Half of the injuries to the index, middle and ring finger were crush, whereas the thumb and small finger experienced other mechanisms more often (Table 5). A complete breakdown of the fracture types and locations is included in Table 6 and Figure 3. The majority of fractures identified were metaphyseal base, Salter-Harris 2, volar plate/rim and tuft fractures.
Injury count, fracture rate and percentage of all injuries by injured part
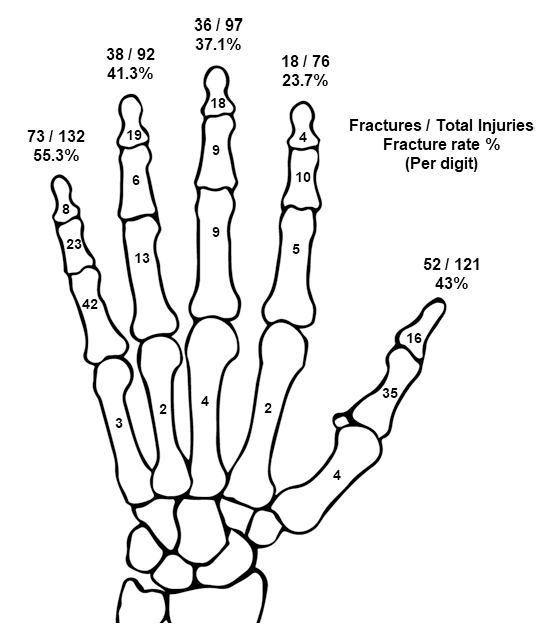
Injury and fracture counts, with fracture rates for each finger and fracture counts for each bony segment.
Injury mechanism distribution by injured part
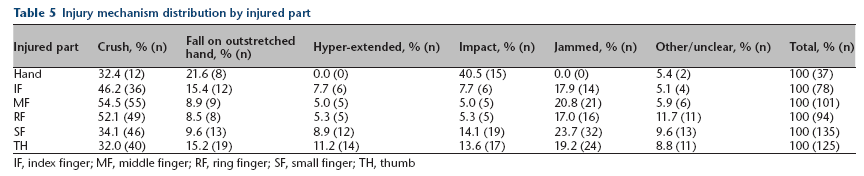
IF, index finger; MF, middle finger; RF, ring finger; SF, small finger; TH, thumb
Fracture counts by fracture type, finger and segment. Letters in parentheses refers to fracture location in Figure 3
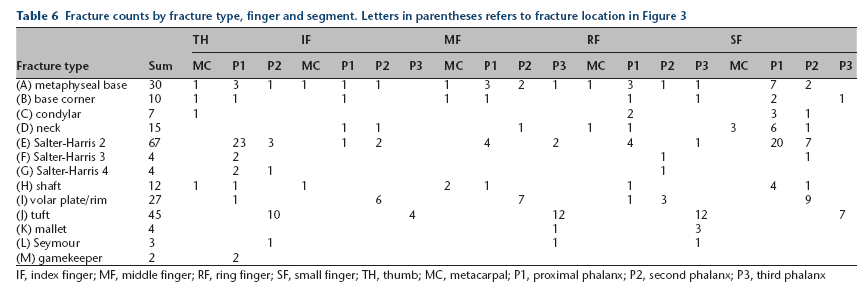
IF, index finger; MF, middle finger; RF, ring finger; SF, small finger; TH, thumb; MC, metacarpal; P1, proximal phalanx; P2, second phalanx; P3, third phalanx
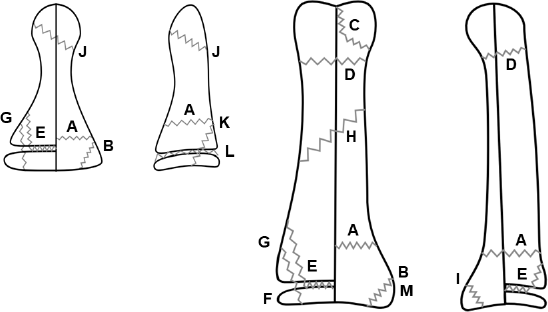
Fracture types referenced in Table 6. From left to right: coronal and lateral views of a distal phalanx, coronal and lateral views of a middle or proximal phalanx.
Mean delay between injury and presentation was 1.82 days (0 to 32 days). Overall, 66% of patients were seen within one day of injury. We did not find patterns relating to season, day of the week or between presenting delay and age or mechanism. In all, 9.8% of patients initially presented at another facility, a group biased towards more significant injury, with a fracture rate of 82.3%.
We found that ICD coding was rarely injury-specific. While 89.1% were correctly coded for fracture, 53% did not specify finger or laterality, 12% specified only laterality, 9% specified only the finger and just 26% specified both. This pattern did not vary significantly between fractures and non-fractures. Only 15% of fracture codes specified the bony segment. Review of imaging by the authors compared with the radiology reports found 92% of injuries received radiographs and that 7% of reports incorrectly identified fracture presence. During evaluation, 14.9% of patients (n = 78) received a paediatric orthopaedic consultation at initial presentation. Of those 78, there were 18 bedside debridements performed, 29 additional closed reductions and 74 were immobilized by buddy tape, splint or cast. Thus, 9% of all patients underwent an initial orthopaedic procedure. At discharge, 32% were referred for hand specialty clinic follow-up. This was generally successful with only 9% of those patients forgoing follow-up in our clinics. Of the 523 patients, 11 were subsequently taken for operative treatment (2.1%). The injuries indicated for operative fixation were certain displaced fractures (three phalangeal shaft, two phalangeal neck, one intracondylar, one metacarpal head and one Rolando thumb base), an infected Seymour fracture and two flexor tendon injuries.
Discussion
Using a large sample group, our goal was to characterize the basic characteristics of all paediatric mechanical hand injuries presenting for urgent/emergent care within a US metropolitan area. With over 500 patients, this report represents one of the largest published collections not based on diagnosis coding.4,5 8 These injuries were responsible for 0.64% of all emergency and urgent care visits, while in other studies, this rate has been as high as 2.1%.3,5,19 This rate should vary depending on the availability of other local hospitals and population age distribution. Epidemiological studies have described an annual paediatric hand injury incidence ranging from 9 to 10, 4 to 18 to 26 per 1000 children per year. 20 Studies focused on fracture rates found incidences from 0.24 11 to 6.24 7 per 1000 children per year. Paediatric hand fracture rates have probably been best characterized by Vadivelu et al, 6 at about 4.18 per 1000 children per year, with soft-tissue injuries increasing that number at least 50%. Direct comparisons are limited by differences in age distribution, population served and ability to capture all patients. A major common limitation are studies investigating subsets of all patients: those with subspecialty referral,6,11–13 only fractures8–13,21 or surgical patients. 14 In our study, we found that only 32% of evaluated patients were recommended for subspecialty referral (based on individual acute care providers’ judgement), suggesting that nearly two-thirds of injuries described in this work would not have been captured by studies limited to subspecialty clinic populations.
Similar to prior reports, we found a bimodal age distribution of injuries in both genders, with peaks in the toddler and teenage groups.3,5,11,12,14,21 In teenagers, male patients predominated by a large margin of 69.4% to 30.6%, with a peak prevalence about 1.5 to two years older than in female patients. Interestingly, under age 12 years, the gender distribution was nearly even, with boys accounting for only 51% of injuries. When including teenagers, the male rate rose to 56%, closer to other reports’ larger male marjorities.4,5,9,11,13,14 This may be due to our patient population, or a consequence of capturing all injuries, and not just fractures. The drop in injury rates seen in older teenagers likely represents a shift to adult facilities and not an actual decrease in injury rate. 13 Like prior reports, there was an interesting gender/age contrast in fracture rates, with higher rates in younger girls despite similar injury rates, and then shifting to older boys.6,10
We investigated injury mechanisms by focusing on the specific injury event, while some studies have categorized by the patient's activity or environment (such as ball sports or home versus school) during the injury4,14 and others reporting a mixture of mechanism and activity/environment.3,8,9,11–13 These categorizations provide overall risk information for those activities and environments, but applicability for care providers evaluating specific patient injuries may be limited. We found that in younger children, crush injuries predominated and resulted in a low fracture rate of 28%. FOOSH, impact and jamming injuries were much more common in older children, likely representing higher levels of activity and sports involvement. Those mechanisms also came with a much higher fracture rate of over 50%. Hyperextension injuries were found to be particularly prone to fracture with a rate of over 80% in teenagers.
When evaluating distribution across the hand, we found that border digits (thumb and small finger) were injured more often than central digits, consistent with prior reports.6,11,13 This likely correlates with their peripheral position putting them at higher risk for getting caught on passing objects. When injured, those fingers also fractured at higher rates. The index finger was injured least frequently and fractured least often when injured, perhaps relating to its strength, relative central position and shorter length than middle or ring fingers. Border digits were more likely to fracture the proximal phalanx, while the middle and ring finger most commonly fractured at the distal phalanx, usually due to crushing injuries, and potentially secondary to their longer length.
Two-thirds of patients were seen within one day of injury, with an overall mean delay of 1.82 days, suggesting good urgent care accessibility in our system. Approximately one in ten injuries seen in our emergency department or urgent care had been evaluated previously by another facility. Those patients had a fracture rate of 82.7%, almost twice the fracture rate of children presenting for the first evaluation. This trend demonstrates that our data set may overrepresent more complex injuries.
We found that providers correctly coded for fracture a majority of the time. Unfortunately, approximately one in ten patients were discharged with a diagnosis code that incorrectly documented fracture presence, and only one-quarter of all codes specified laterality and finger, with even fewer, at about 15%, identifying specific bony segments injured. This supports the characterization that studies based on coding are limited in their ability to characterize specific injury patterns16–18 and reliably document fractures. 9 Ultimately, one-third of our study patients were referred to hand specialty clinic follow-up, which in our system is a group of paediatric orthopaedists, hand surgeons, paediatricians and physician assistants, all with extra experience in paediatric hand fractures. Of those referred, 92% were successfully seen, suggesting good availability of follow-up within our system. While only 2.1% of all patients subsequently went for operative fixation, an additional 9% underwent an orthopaedic procedure such as debridement, nailbed repair or closed reductions. Our data's limitations are not unlike other studies, namely an inability to capture patients who present to other providers and facilities in the area due to age, geography or preference. Because patients with less severe injuries are more likely to present to primary care providers in a non-urgent manner, we expect our data under-represent those injuries.
In conclusion, we performed an 18-month retrospective review of all hand injuries presenting to a paediatric tertiary hospital and its satellite clinics to identify injury patterns, fracture rates and diagnosis and referral behaviours. This study contains one of the largest data sets of paediatric hand trauma to date not based solely on diagnosis coding, significantly improving its accuracy and detail. By including all injuries, not just fractures or those requiring subspecialty referral, our results provide a broader understanding of the scope of mechanical paediatric hand trauma. We found that certain injury mechanisms and age groups had lower rates of fracture and injuries not requiring subspecialty follow-up. With further study, it may be determined that certain patterns do not need radiographs at initial evaluation or subspecialty follow-up, expediting workup and decreasing costs.