
Abstract
Purpose:
Conventional radiography is frequently performed in pediatric patients in whom finger fractures are suspected. However, until now, the rate of positive findings of finger radiographic examinations in pediatric patients is unknown. This study aimed to evaluate the number of positive findings in the standard radiographic examinations of finger injuries in pediatric patients in a Level 1 trauma center systematically.
Methods:
We conducted a retrospective study on all children 0–16 years old admitted for acute finger injury in the Emergency Department of a University Hospital during the first semester of 2019 and received a radiographic examination. Their demographic characteristics, fracture pattern, and treatment were then analyzed and interpreted.
Results:
Out of 478 finger injuries reviewed in this cohort, 160 X-rays revealed positive for a fracture giving a fracture rate of 33.5%. More than half of them (51.9%) occurred in the age group of adolescents (11–16 years). Among all finger fractures, only 3.8% of them treated surgically.
Conclusion:
In this study, a relevant amount of standard finger radiographs revealed a low fracture rate and a rare operative indication of 3.8%. Therefore, indications for X-rays should be reviewed properly and alternative procedures should be discussed. Clinical decision rules should be developed and the necessary pathways must be implemented to minimize radiation exposure, waiting time, and costs.
Level of evidence: level IV
Keywords
Introduction
The hand is the most frequently injured part of the body in the pediatric and adolescent age group,1,2 with finger fractures being the most common type of hand fracture that occurs in the pediatric population.3,4 Although few data exist on the number of minor finger injuries that require only symptomatic treatment and heal without sequelae they likely account for the majority of all pediatric hand injuries. Significant finger injuries, although rare, must be recognized by the emergency physician since they may cause massive disability in children. 5 Conventional X-rays are in the first-line imaging of choice in pediatric finger trauma and are frequently asked from emergency physicians out of fear of failing to diagnose a fracture or dislocation in the pediatric patient rather than on patients’ trauma circumstances and accurate clinical examination. Consequently, unnecessary radiation exposure, prolonged waiting times in emergency departments, and accumulated costs from the frequent application of conventional X-rays for unnecessary investigations may be avoidable.
Since no validated clinical guidelines exist to the indication of an X-ray for the instance, as for ankle and cervical spine (i.e. Ottawa Ankle Rules or Canadian C-Spine Rule), the knowledge of fracture rates in standard radiographs in pediatric finger trauma is a useful instrument to evaluate the indication for a radiographic examination in combination to patients’ history and accurate clinical examination.
There are only a few studies published on the finger fracture rates on standard radiographs after trauma in the pediatric population.5–7 Therefore, this study aimed to retrospectively evaluate the number of positive fracture findings in finger standard radiographic examinations in pediatric patients in a Level I pediatric trauma center.
Materials and methods
After obtaining approval from the local Ethics Committee, we performed a single-center retrospective study from January 2019 to June 2019 including 475 consecutive patients who had sustained a finger trauma and received a radiographic examination. All patients presented to the pediatric emergency department of our University Hospital spontaneously after the accident or were referred to the emergency department by a pediatrician within 48 h of the accident. Children included in the study were aged 0–16 years with a mean age of 10.1 years. We excluded from the cohort children if suffered from the Ehlers–Danlos disease, if surgery on the injured finger had been performed within the previous 6 months, and if they presented repetitive trauma on the same finger, dislocation, or polytrauma.
The indication for the radiographic examination was a suspected fracture after trauma. All standard finger X-rays from patients under 16 years old admitted to the pediatric emergency department after finger trauma from January 2019 to June 2019 were analyzed. During this period, no specific clinical guidelines were used by our physicians to evaluate a patient.
Positive X-rays findings were defined as a disruption of at least one cortex of the bone. Avulsions, fissures, buckle, or bowing fractures were also included. X-ray with localized soft tissue swelling without any bone lesion was considered negative.
The images were evaluated by an experienced pediatric radiologist using a digital radiologist workstation and by an experienced pediatric orthopedic surgeon. In case of doubtful findings, the images were re-evaluated by a senior consultant in pediatric orthopedic surgery.
Microsoft Excel was used for data collection including demographic characteristics (age, sex, laterality) of the population studied. Our population was divided into three groups according to their age at the time of injury: (1) 1–5 years: toddlers and pre-school children, (2) 6–10 years school-age children, and (3) 11–16 years adolescents. There were no patients younger than 1 year in this cohort. In case of positive X-rays, we recorded the location of the lesion (finger and phalanx number) as well as the type of injury as follows: (1) intra-articular fractures including Salter–Harris III, IV, and V and epiphyseal bone avulsions more than >30%, (2) extra-articular fractures including metaphyseal, diaphyseal, and Salter–Harris I and II fractures, and (3) crushing fractures of distal phalanges. Subsequently, for the population with positive radiologic findings, we reviewed the methods of treatment distinguishing in conservative (splinting and/or syndactyly) and surgical.
The data were evaluated using descriptive statistics to determine the frequency of different factors surveyed. Statistical analysis was performed using the Mann–Whitney U test for continuous variables, chi-square, Fisher’s exact tests for categorical variables, and Spearman’s rho tests. Statistical significance was taken to be at P < 0.05.
Results
Four hundred seventy-five consecutive patients with a mean age of 10.1 years with a total of 478 injured fingers were included in this study. The overall fracture rate was 33.5% (160/478). Just more than half of all fractures occurred in the age group of adolescents (11–16 years) (51.9%, n = 83). Six- to ten-year olds accounted for 31.8% of all fractures (n = 51) and only 16.3% (n = 26) of fractures occurred in toddlers and pre-school children. The incidence of finger fractures rose greatly from 9 years old (p < 0.001) peaking at 12 years. The proportion of fractures in the groups of 0–5 years (16.2%), 6–10 years (31.9%), and 11–16 years (82.2%) increased with increasing age.
Overall, boys accounted for 63% (n = 101) and girls 37% (n = 59) of all fractures in this cohort giving a male-to-female ratio of 1.7:1. Compared to girls, the number of fractures in boys was significantly increasing with increasing ages (Spearman’s rho test, p = 0.69, P = 0.03). In the youngest age group, 0–5 years, when the overall fracture ratios were compared, girls (n = 13, 22.1%) were more prone to have finger fractures compared to boys (n = 13, 12.9%). After the age of 5 years, the number of fractures in boys was higher than in girls with increasing age (Spearman’s rho test, p = 0.42, P = 0.17).
Figure 1 illustrates the distribution of finger fractures by age and sex.
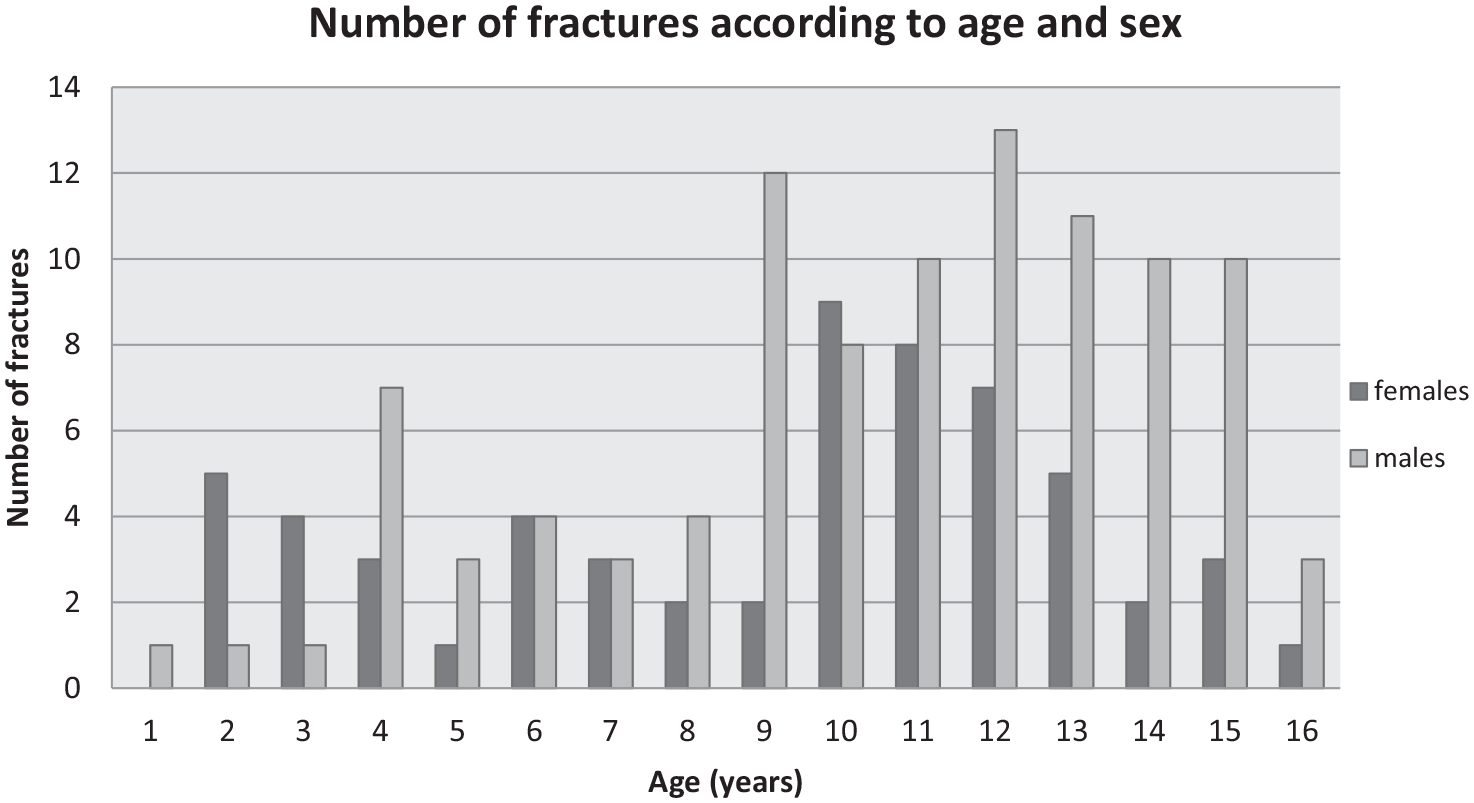
Distribution of finger fractures by age and sex.
One hundred fifty-five patients (98.9%) had one fracture on each involved digit, whereas two children sustained two fractures on a single digit, and three patients sustained a single fracture on multiple fingers on the same hand.
The distribution of fractures by phalange of each digit in the different age groups is shown in Figure 2.
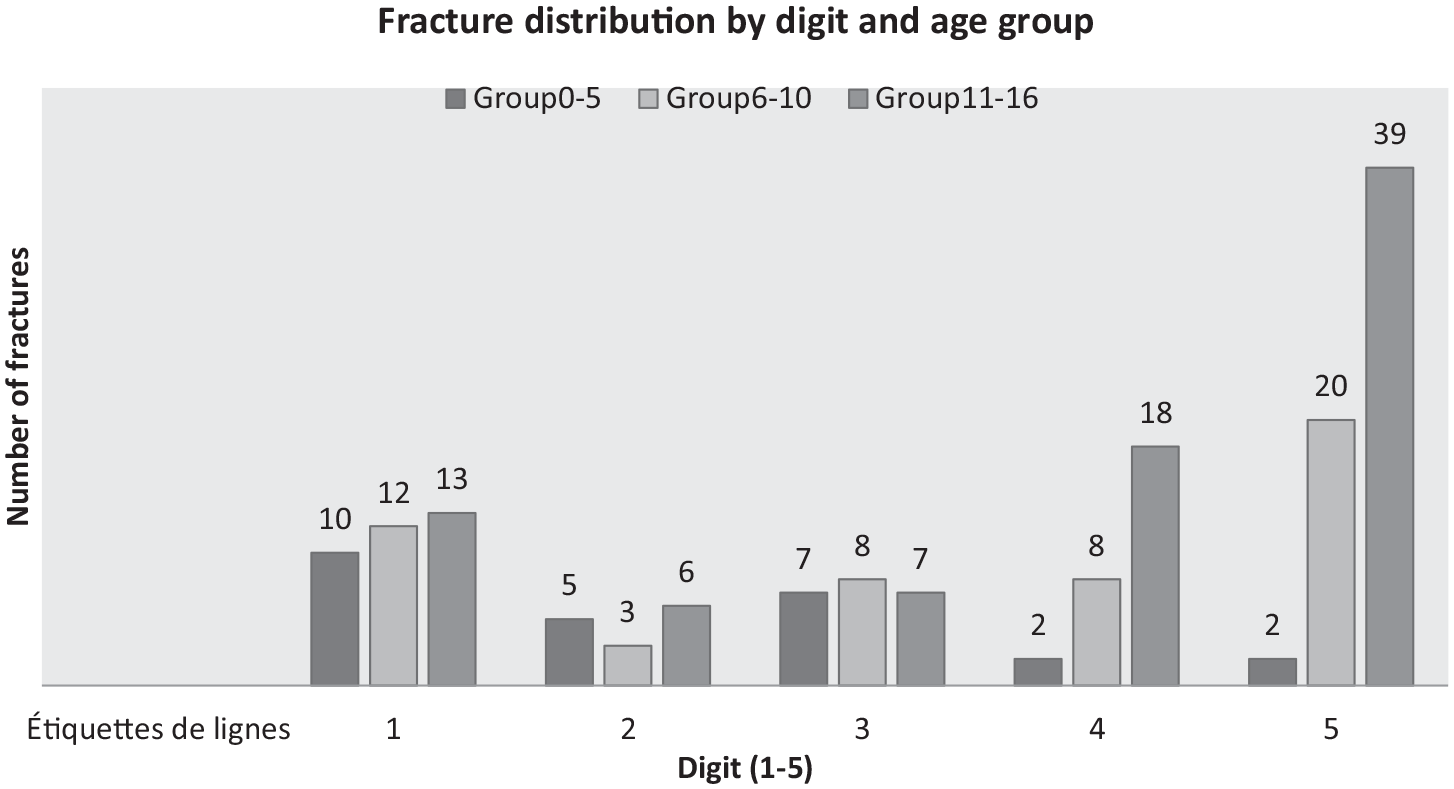
Distribution of fractures by digit and age group.
A higher incidence of thumb fractures was observed in the toddlers and pre-school group, and the fifth digit was the most frequently fractured in children 6 years and elder (p = 0.01).
In contrast to older patients, most of the toddlers and pre-school children were affected by distal phalange fractures (69.2%). As demonstrated in Figure 3, the older the patient, the most proximal the phalange fractured due to finger trauma.
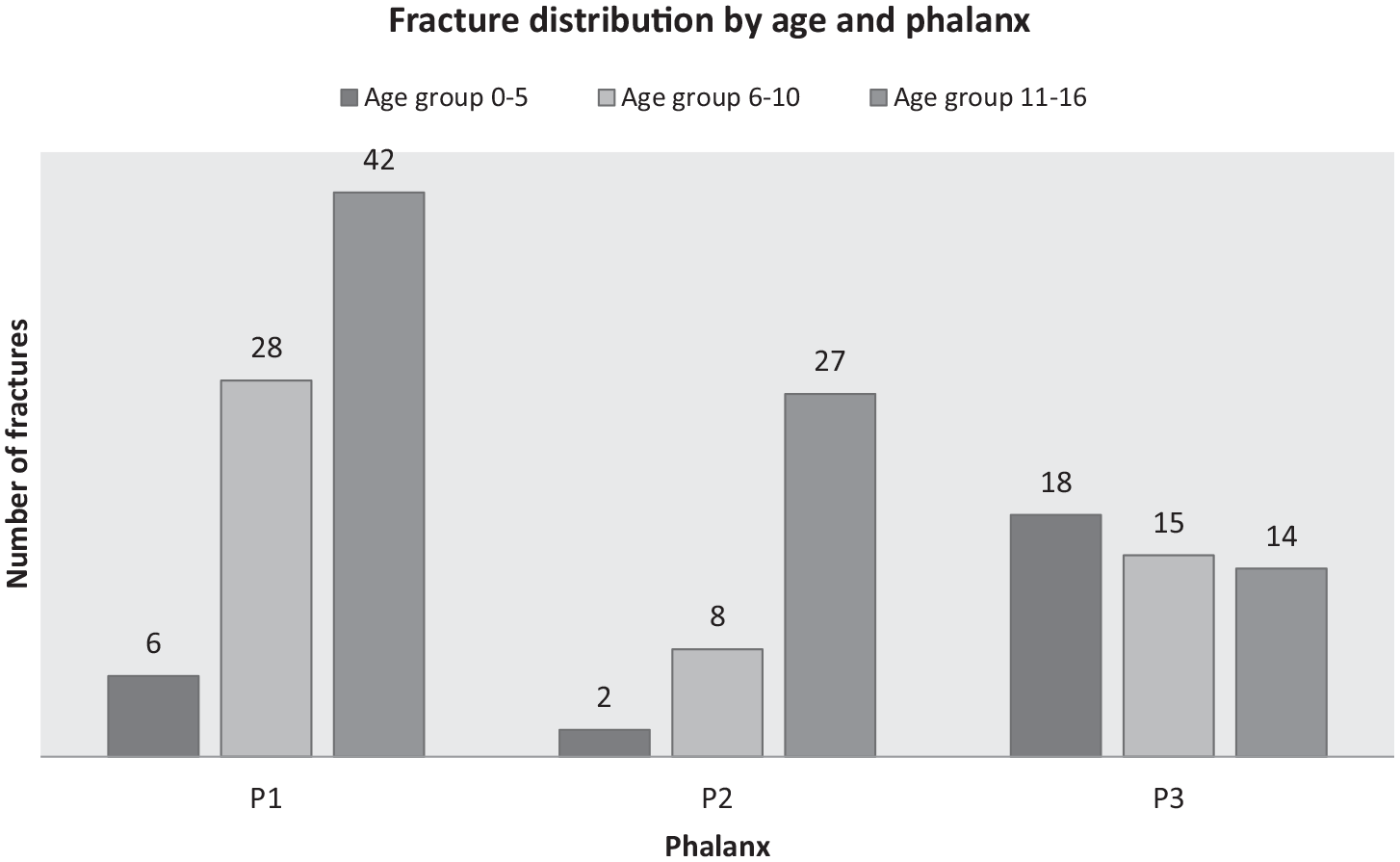
Fracture distribution by age and phalanx.
According to the fracture pattern in the positive for fracture X-rays, the majority of them (70%, n = 112) were extra-articular including metaphyseal, diaphyseal, and Salter–Harris I and II fractures, 16% were crushing fractures of distal phalanges, and 14% were intra-articular fractures including Salter–Harris III, IV, and V and epiphyseal bone avulsions more than >30% (Figure 4). The incidence of Salter–Harris II fractures peaked in the adolescent group with 60.2% (n = 50) of patients in this group to have sustained them in a proximal phalanx.
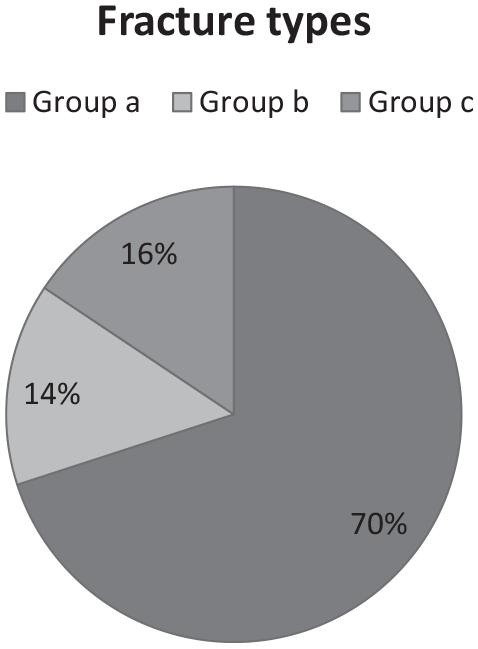
Distribution of fractures according to the fracture pattern.
Compared to the female patient population, Salter–Harris II fracture was significantly more common in males (65/160) (p < 0.0001) versus females (28/160), whereas crushing fracture of the distal phalanx was more common in females (16/160) versus males (9/160).
The details regarding the children’s initial treatment and follow-up were available for all patients in our cohort. Most finger injuries (98.7%, N = 469/475) were treated with immobilizing the finger (e.g. syndactyly, splinting, or casting). Among the 160 X-rays positives for fracture, closed reduction in the emergency department was provided in 17 patients before immobilizing (10.6%). Irrigation and wound closure as the initial management were performed for five crush injuries of distal phalanges (3.1%). No patient was presented with complicated soft tissue injuries at the time of their fractures in this cohort. Only six patients (3.8%) were treated surgically; all of them included in the group a. Two of them (1.25%) were treated with open reduction and internal fixation and four of them with closed reduction and percutaneous fixation with the Kirschner wires.
Discussion
In this cohort, we demonstrated a finger fracture rate of 33.5%. There are only a few studies published on this topic in children. In most of the publications, hand injuries are investigated and are not split up into anatomic regions (i.e. fingers). Nevertheless, in studies where finger injuries in children are clearly defined, the reported fracture rates are lower, ranging from 18.5% to 25.7%.5,8,9 A possible explanation for the higher rate in this study could be the application of the ALARA principle in several Pediatric Trauma Centers according to clinical examination 5 where not every finger trauma in children is investigated by an X-ray, as in our cohort. The results of this study demonstrate that more than half of all fractures occurred in the age group of adolescents (11–16 years) (51.9%, n = 83). The prominent peak in the early teenage years is also observed by other authors.2,6,7,9–12 This trend is likely related to increased participation in sports with increasing age. Overall, there was a preponderance of boys in our fracture series with a male-to-female ratio of 1.7:1. Similar results are also reported by other authors.6,7,9,13,14 However, in children aged 5 or younger, 50% were females. A similar distribution has been reported by other authors.9,10,13,15 In our series, most finger fractures (69.2%) in toddlers and pre-school children were observed in the distal phalanxes and the thumb was the most frequently injured digit. Whereas in children 6 years and elder, the fifth digit was the most frequently fractured with the observation that the older the patient, the more proximal the phalanx fractured. This trend is likely related to the mechanism of injury, with young children being vulnerable to crush injuries and older children being injured during sports. This is also in keeping with observations by other authors.9,10,12,14–16 Knowledge of digit fracture common site in each age group, in combination with the mechanism of trauma and clinical signs of fracture, may aid physicians to estimate the necessity of radiologic examination to establish the diagnosis. Authors suggest an optimal pre-set scheduled examination of closed finger injuries in children to distinguish acute minor from major injuries according to the mechanism of injury. We chose four clinical signs to be evaluated systematically in every closed finger trauma: (1) axial or rotational deformity, (2) hematoma, (3) swelling, and (4) active mobility of the finger compared with the uninjured site. The presence of deformity or hematoma is considered absolute indications for radiologic evaluation independent of the mechanism. For sport injuries, in the absence of deformity and hematoma, X-rays are also suggested if the presence of localized swelling and reduced active joint amplitude more than 50% comparing to the contralateral site after Stage I analgesia. For open injuries with the absence of all the previous signs, we do not recommend radiological examination unless the presence of a foreign body is suspected. Wound exploration by a hand specialist is highly recommended. In case of need of radiologic evaluation, we recommend posteroanterior and lateral X-rays of the isolated digit rather than hand views which may lead to misdiagnosis.2,9 The misdiagnosis rate due to inadequate X-rays or misinterpretation of them arrives to 8% according to the current literature.2,9 When a fracture is suspected, it is important to correlate the area of clinical abnormality, with the radiological abnormality of properly obtained radiological incidences.
Moreover, similar to other previous studies, we could demonstrate that Salter–Harris Type 2 fracture of the proximal phalanx was the most common finger fracture type in older children.3,6,7,9 The demonstrated domination of distal phalanx fractures in toddlers and pre-school children, as well as in the female gender, is in agreement with the previous studies.6,8,9,13
Surgical treatment of hand fractures is quite rare. The rate of surgical treatment of finger fracture ranges from 0.8% to 6% of all fractures, according to different studies.6,7,10,17 Throughout the study period, we found that only 2 out of 160 (1.25%) finger fractures required surgical treatment.
Due to the very low need for surgical treatment for finger fracture, the need to investigate by X-ray every finger trauma becomes questionable. As most of the injuries usually require conservative treatments such as splinting, it would be interesting to compare the rate of clinical suspicion of finger fracture in the Emergency Department versus the fracture rate based on the radiographs, to understand whether a clinical examination is sensitive enough to distinguish sever finger trauma from minor. According to the ALARA principle, we should expose the patient to radiation as little as necessary; thus, a validated clinical scoring system to distinguish minor from major finger trauma could be developed. Prospective multicentric studies are encouraged to establish reliable criteria for accurate clinical diagnosis. Fewer radiographic investigations will not only minimize radiation exposure and its stochastic effects in the pediatric population, 18 but also will diminish waiting times in Pediatric Emergency Departments. Furthermore, it could be beneficial in terms of cost. Especially as we reported that a finger radiograph costs around 100 CHF and that around 500 patients were radiographed over 6 months, which is quite significant.
Limitations of the study are related to its retrospective and monocentric design. The database lacks information related to the mechanism of injury and to clinical signs at the time of presentation. Insufficient medical reports of these two factors obliged us to discard this information for fear of bias. The strength of this study is that it is focused on finger fractures specifically and provides clearer epidemiology comparing to the literature where hand injuries are not split up to anatomic regions. The knowledge of the incidence of finger fractures and their common sites in each age group can help physicians not only diagnose and treat accurately but also Health Systems find measures to prevent these lesions in the pediatric population.
Conclusion
This study showed a relatively low fracture rate of 33.5% in pediatric finger injuries from which only 1.25% needed surgical treatment. When the cost and X-ray exposure are considered, the added value of radiographic examinations to decide the need for surgery for pediatric patients should be reconsidered. A careful physical examination and a well-established clinical scoring system taking into consideration clinical signs such as deformity, swelling, hematoma and limitation of joint mobility can be a useful alternative to unnecessary radiographic examinations.
Footnotes
Author contributions
S.S. contributed to conception and design of the study, collected data, carried out statistical analyses, drafted the initial manuscript, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. N.L. collected data, reviewed and critically revised the manuscript, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. E.V. collected data, carried out statistical analyses, reviewed and critically revised the manuscript, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. S.M. contributed to the design of the study, reviewed and critically revised the manuscript, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. P.-Y.Z. substantially contributed to the design of the study, reviewed, and revised the manuscript, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. E.S. conceived and designed the study, collected data, carried out statistical analyses, drafted the initial manuscript, approved the final manuscript as submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The informed consent from all participants/their parents/carers was waived due to the retrospective nature of this study.