
Abstract
Abstract
Purpose
We sought to determine if a varus-producing osteotomy of the proximal femur was related to a better outcome than non-operative treatment for LCP disease.
Methods
This was a retrospective review of 121 patients; clinical outcome was determined with the Iowa Hip Score, and radiographic outcome was determined with the Stulberg classification.
Results
A total of 73 patients undergoing a VO and 48 treated non-operatively were included; 70 had lateral pillar type B and 51 type C hips. Average follow-up was 12.03 years. The mean Iowa Hip Score was 86.8 for the VO group and 85.9 for the non-operative group. According to the Stulberg classification for the group undergoing a VO, there were 8 type II, 33 type III, and 32 type III, and for the group undergoing non-operative treatment there were 11 type II, 24 type III, and 13 type IV.
Conclusions
We found no statistically significant difference in the clinical or radiographic result for patients undergoing a VO compared to non-operative treatment.
Introduction
The optimal treatment of Legg-Calvé-Perthes disease (LCP) remains elusive; many of the concepts regarding the disease have not evolved in almost a century [1–6]; in fact, the original descriptions by Legg, Calvé, and Perthes contain some pertinent points that are still valid today. While many theories on the etiology have been proposed and some causal relationships have been established [7–12], no single cause has been identified. It is clear that the disease affects boys more often than girls [13], and it is well known that the radiographic result of a flat head is associated with the development of early degenerative arthritis [5, 14–22]. The controversy surrounding the treatment of disease becomes understandable when the different strategies for it are numbered [22–27]. However, to be able to consider any treatment as the standard of care, it must be proven to produce clinical results better than those obtained without treatment.
A recent landmark multicenter study determined that the outcome of hips with LCP in the B or B/C borderline group in children over the age of 8 could be improved with surgical treatment [28]. Children under the age of 8 tend to do well in general, and children with hips classified as C by the lateral pillar classification tend to do poorly regardless of treatment. Although these conclusions are somewhat broad, they are generally held true by pediatric orthopedic surgeons all over the world. Many surgical procedures have been used in an attempt to favorably alter the course of the disease [29–33]. One of the most commonly applied procedures is a varus-producing osteotomy of the proximal femur (VO). The option not to operate on these patients and treat them with a regime of physical therapy and functional rehabilitation also has many proponents [34].
The disease courses with four distinct clinical stages: an initial ischemic insult is followed by a stage of fragmentation, then a stage of reossification, and finally a stage of remodeling that ends at skeletal maturity. Most patients present to the orthopedist during the stages of fragmentation, or reossification, when treatment poses a significant challenge [35]. Many studies on the outcome of the disease and treatment of it are flawed because of the variable duration of the stages and the moment at which surgery is performed.
There is a direct relationship between the radiographic appearance at skeletal maturity as determined by the Stulberg classification and the incidence of early degenerative arthritis [14, 16, 35–37]. The clinical result, however, at the time of skeletal maturity is not always related to the radiographic appearance [38].
We sought to determine if the clinical outcome of LCP disease was favorably altered by a varus-producing osteotomy when compared to a matched group of patients treated with physical therapy.
Materials and methods
A retrospective review of all patients undergoing treatment for LCP disease at the Shriners Hospital for Children in both Mexico City and Houston was undertaken. The clinical chart was used to determine the age at the time of presentation, the treatment, the age at time of surgery when performed, and the presence of pain or a limp. The clinical outcome was determined by using the Iowa Hip Score at the time of final follow-up. The radiographic chart was used to determine the lateral pillar classification at the time of presentation as well as at the time of surgery, and the Stulberg classification was used to determine radiographic outcome.
We decided only to include those patients undergoing a proximal femoral varus osteotomy as the study cases and only those treated with inpatient traction and physical therapy as the control cases; only patients classified with the lateral pillar classification as type B or type C were included. We excluded all patients with bilateral disease in order to improve classification and reduce measurement error. We identified 73 patients undergoing a varus osteotomy and 48 patients with non-operative treatment who had reached skeletal maturity at the time of this review. The patients were not specifically allocated to either treatment group; this reflects the differing opinions of the attending orthopedic surgeons at the time of the review.
The varus-producing osteotomies were all performed by senior pediatric orthopedic surgeons, all were performed in the intertrochanteric region, and most were fixed with a dynamic hip screw, although some were fixed with an angled blade plate. All of the osteotomies were done in the fragmentation stage; the mean time between initial diagnosis and surgery was 4.3 months. The average femoral neck-shaft angle was reduced from 138° to 112°. The postoperative protocol was to keep the children on protected weight bearing for a period of 6 weeks, followed by a physical therapy program consisting of range of motion and strengthening exercises, performed at least once a week in the hospital and as a home program on a daily basis. For the group undergoing non-operative treatment, the protocol included in hospital skin-traction for 17 of the patients, with 3–7 lbs of weight with the patient supine and the knee extended. It was utilized on average for 11.4 days, and there was a supervised program of physical therapy consisting of stretching exercises of the hips, hamstrings, and lower back and a strengthening program focusing mainly on the gluteus medius. All patients were evaluated by a senior physical therapist experienced in pediatric patients. We do not have data on compliance with home-therapy programs.
The lateral pillar classification was determined by three different observers in all cases; all were either senior pediatric orthopedic surgeons or pediatric orthopedic fellows. The lateral pillar classification initially included only three types: type A where the lateral pillar maintains 100% of the height when compared to the other hip; type B presenting up to 50% of collapse of the lateral pillar when compared to the other hip; type C where there is over 50% collapse of the lateral pillar when compared to the healthy hip. In 2004 a modification was added to include a fourth group known as the B/C borderline group to include those hips considered difficult to classify. We decided not to use the current modification of the lateral pillar classification, which incorporates the B/C borderline group, as it was not in use at the start of the study, and we considered interobserver variability to increase with the addition of this group. When there was a discrepancy in the classification, the most agreed-upon grade was used (i.e., two out of three). This only happened in 14 cases.
The Stulberg classification describes the radiographic appearance of the hip at the time of skeletal maturity and includes five types: type I is defined as a completely normal hip; type II indicates hips that have a spherical femoral head that is larger than normal, has a short neck, or an abnormally steep acetabulum. Sphericity was determined with the protractor technique as described by Herring et al.; to consider a hip to be a type II, the same concentric circle should match the femoral head on both the anteroposterior and frog-leg lateral X-ray views. Type III hips have a non-spherical femoral head with an ovoid mushroom or umbrella shape, but not flat; type IV hips have a flat femoral head that is articulated with a flat acetabulum, and type V hips have a flat femoral head within a round acetabulum. For final determination we used the same method of having three experienced observers classify each set of radiographs; at least two senior pediatric orthopedic surgeons and one pediatric orthopedic fellow classified each radiograph. There was a discrepancy in the grade given to the hips by the different observers in only seven cases where the majority view was used.
The Iowa Hip Score was used to determine the clinical outcome at the time of final follow-up. This outcome measures various aspects of hip function and is reported as the sum of points with 100 being the maximum available. We considered a result between 90 and 100 to be an excellent clinical result, between 75 and 90 a good result, between 60 and 75 a fair result, and below 60 to be a poor result.
The results were statistically validated by using the paired Student's t test, considering a P value less than 0.05 to be statistically significant.
Results
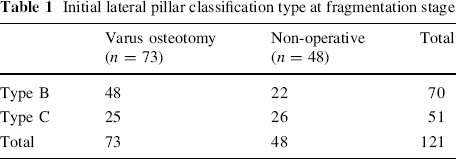
In all, we had 121 patients, 73 who underwent a VO and 48 who were treated non-operatively. The mean age for the entire population was 5.52 years, for the group undergoing a varus producing osteotomy the mean age at the time of initial diagnosis was 5.68 years, and for the group undergoing non-operative treatment the mean age at the time of initial diagnosis was 5.20 years (P = 0.03). The mean age at the time of surgery was 6.02 years. There was a male predominance: 103 of the 121 were boys, and both treatment groups had the same distribution, with 86% of the patients in the VO group being boys and 87% of the patients in the non-operative group being boys. As far as the lateral pillar classification, 70 patients were classified as being type B, and 51 were classified as being type C. In the group undergoing a VO, 48 patients were classified as type B and 25 as type C, whereas in the non-operative group, 22 patients were classified as type B, and 26 were classified as a lateral pillar type C (Table 1).
Initial lateral pillar classification type at fragmentation stage
Average follow-up for the entire population was 12.03 years (range 6.2–19.7 years). For the VO group, average follow-up was 12.71 years, and for the non-operative group average follow-up was 11.66 years. Average age at the time of final follow-up was 18.3 (range 17.3–26.3).
From the clinical charts we recorded the presence of pain at the time of initial evaluation and found that at the time of the initial visit, 111 of the patients had reported pain. Sixty-nine of these patients with pain were in the group undergoing a VO, and 42 patients were in the non-operative group; only 4 of the patients in the group undergoing a VO and 6 patients in the non-operative group were without pain. At the time of the initial visit, 115 patients had a limp, 71 of the patients undergoing a VO and 44 in the non-operative group. Only two patients from the group undergoing a VO and four patients from the non-operative group did not present a limp.
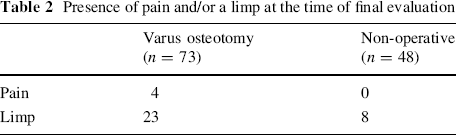
At the time of final evaluation, four of the patients in the group undergoing a VO referred to pain, whereas no patients in the non-operative group referred to pain. Twenty-three of the patients in the group undergoing a VO presented a persistent limp at the time of final follow-up, whereas only eight patients in the non-operative group did (Table 2).
Presence of pain and/or a limp at the time of final evaluation
There was residual shortening (average 23 mm) in 45 patients who had undergone a VO; most were managed with a shoe-lift, and three have undergone a subsequent contralateral epiphysiodesis. All 23 of the patients with a persistent limp had a residual shortening (average 26 mm). There was also residual shortening (average 18 mm) in 21 patients who had undergone non-operative treatment; all of these were managed with a shoe-lift.
The mean Iowa Hip Score at the time of final evaluation was similar for both groups. For the group undergoing a VO, it was 86.8 ± 6.8, and for the non-operative group, it was 85.9 ± 7.1 (P = 0.56).
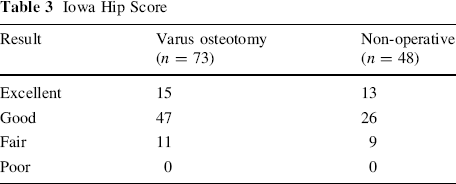
According to the Iowa Hip Score for the group undergoing a VO, we found 14 excellent results (21%), 47 good results (64%), and 11 fair results (15%). In the non-operative group, we found 13 excellent results (28%), 26 good results (54%), and 9 fair results (18%). No poor results were found in either group (Table 3).
Iowa Hip Score
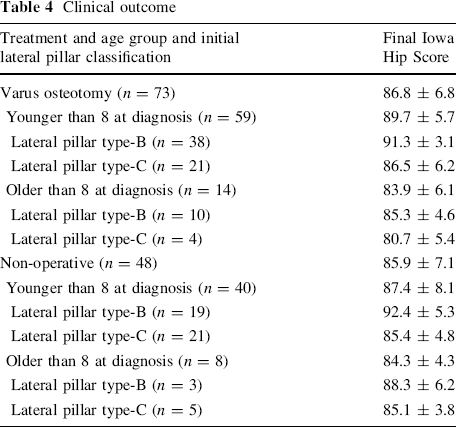
We did note a lower Iowa Hip Score with increasing age at the time of surgery, with a mean of 89.7 ± 5.7 for patients under the age of 8 at the time of surgery compared to 83.9 ± 6.1 for patients over 8 at the time of surgery (P = 0.011). We also noted a better Iowa Hip Score for those patients undergoing non-operative treatment when the age at initial diagnosis was less than 8 years old with a mean of 87.4 ± 5.2 for those under 8 and 84.3 ± 4.3 for those over 8.
Of the 70 patients classified initially as lateral pillar type B, 48 had undergone a VO and 22 were in the non-operative group. The clinical results for these patients showed a mean Iowa Hip Score of 91.9 ± 5.6 for the group undergoing a VO and 88.5 ± 6.4 for the group undergoing non-operative treatment (P = 0.09).
Of the 51 patients classified initially as having lateral pillar type C, 25 had undergone a VO, and 26 were in the non-operative group. The mean Iowa Hip Score for the group undergoing a VO originally classified as lateral pillar type C was 87.7 ± 6.3, and for the group undergoing non-operative treatment, it was 88.5 ± 4.3 (P = 0.07).
When considering age and lateral pillar classification as codependent variables, the final clinical outcome for each group was as follows: for patients under the age of 8 years at the time of initial diagnosis who were classified as having lateral pillar type B and underwent a VO (n = 38), the mean Iowa Hip Score was 91.3 ± 3.1. For those patients under the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type C and underwent a VO (n = 21), the mean Iowa Hip Score was 86.5 ± 6.2. For patients over the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type B and underwent a VO (n = 10), the mean Iowa Hip Score was 85.3 ± 4.6, whereas for patients over the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type C and underwent a VO (n = 10), the mean Iowa Hip Score was 80.7 ± 5.4.
For patients under the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type B and underwent non-operative treatment (n = 19), the mean Iowa Hip Score was 92.4 ± 5.3. For those patients under the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type C and underwent non-operative treatment (n = 21), the mean Iowa Hip Score was 85.4 ± 4.8. For patients over the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type B and underwent non-operative treatment (n = 3), the mean Iowa Hip Score was 88.3 ± 6.2, whereas for patients over the age of 8 at the time of initial diagnosis who were classified as having lateral pillar type C and underwent non-operative treatment (n = 5), the mean Iowa Hip Score was 85.1 ± 3.8. The clinical results are shown in Table 4.
Clinical outcome
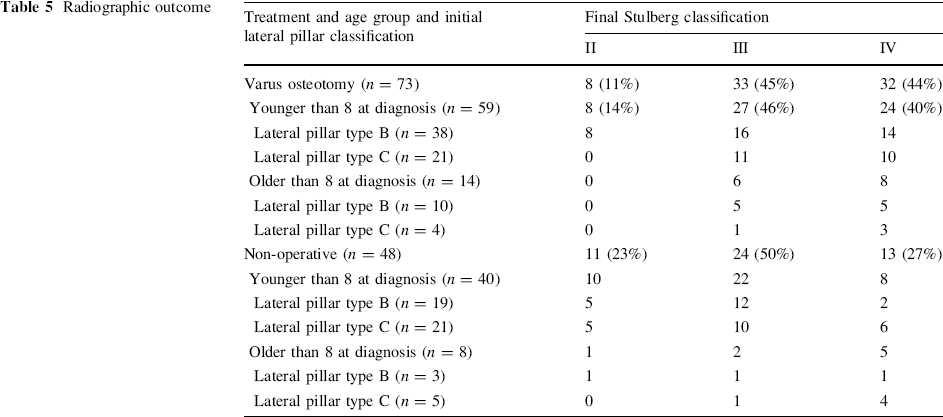
The radiographic outcome was determined according to the Stulberg classification, and we found 19 Stulberg type II hips, 57 Stulberg type III hips, and 45 Stulberg type IV hips. No Stulberg type I or type V hips were found. Of the 73 patients undergoing a VO, 8 resulted as Stulberg type II, 33 as Stulberg type III, and 32 as Stulberg type IV. Of the 48 patients undergoing non-operative treatment, 11 were Stulberg type II, 24 Stulberg type III, and 13 Stulberg type IV.
Of the patients initially classified as having lateral pillar type B (n = 70), 14 were Stulberg type II hips, 24 Stulberg type III hips, and 22 Stulberg type IV hips.
There were 48 patients initially classified as having lateral pillar type B undergoing a VO, resulting in 8 Stulberg type II hips, 21 Stulberg type III hips, and 19 Stulberg type IV hips. Of the 22 patients undergoing non-operative treatment who were initially classified as having lateral pillar type B, the results were 6 Stulberg type II, 13 Stulberg type III, and 3 Stulberg type IV hips.
Of the patients initially classified as having lateral pillar type C (n = 51), 6 ended up with Stulberg type II, 19 with Stulberg type III, and 26 with Stulberg type IV hips.
Of the 25 patients initially classified as having lateral pillar type C who underwent a VO, none ended up with Stulberg type II hips; 12 had Stulberg type III hips, and 13 had Stulberg type IV hips. There were 26 patients undergoing non-operative treatment who were initially classified as having lateral pillar type C; the results of 5 were Stulberg type II hips, 11 were Stulberg type III hips, and 10 were Stulberg type IV hips.
Radiographically for the group of patients who were over age 8 at the time of initial diagnosis, we found the following results: for the patients undergoing a VO (n = 14), there were six patients who ended up with Stulberg type III and eight patients with Stulberg type IV. Of the patients initially classified as having lateral pillar type B who were over 8 at the time of diagnosis and underwent a VO (n = 10), five ended up having Stulberg type III and five Stulberg type IV. Of the patients initially classified as having lateral pillar type C who were over 8 at the time of diagnosis and underwent a VO (n = 4), one ended up with Stulberg type III and three with Stulberg type IV.
For the patients undergoing non-operative treatment who were over the age of 8 at the time of diagnosis (n = 8), we found one patient who ended up with Stulberg type II, two patients who ended up with Stulberg type III, and five patients who ended up with Stulberg type IV. Of the patients initially classified as having lateral pillar type B who were over 8 at the time of diagnosis and underwent non-operative treatment (n = 3), one ended up with Stulberg type II, one with Stulberg type III, and one with Stulberg type IV. Of the patients initially classified as having lateral pillar type C who were over 8 at the time of diagnosis and underwent non-operative treatment (n = 5), one ended up with Stulberg type III and four with Stulberg type IV. The radiographic results are shown in Table 5.
Radiographic outcome
Conclusion
Our patient groups were demographically similar in most ways, consisting of a large series of patients with LCP disease classified as lateral pillar type B and C hips undergoing either a VO or non-operative treatment, and we found no statistically significant difference in the clinical result as determined by the Iowa Hip Score at a long-term follow-up. It should be noted that both groups consisted of patients of a relatively young age.
The overall radiographic results were also similar for both treatment groups with similar Stulberg grading for the hips in each age- and involvement-matched group. The possibility that further follow-up will yield different results for these patients is still latent; however, the Stulberg classification has been shown to have a direct relation to long-term outcome with the presence of early degenerative joint disease being more common with a higher Stulberg type.
Herring et al. [28] stated that patients with lateral pillar group A hips have an excellent prognosis and require no specific treatment. Likewise, children with a lateral pillar group B hip who have the onset of the disease on or before their 8th birthday have a good prognosis and require only symptomatic treatment. They also found that patients who have the onset of the disease on or before the 8th birthday and have a B/C-border group hip have a somewhat poorer prognosis, but do not appear to benefit from surgical treatment. Finally, they found that patients with lateral pillar group B and B/C borderline group hips in children who are older than 8.0 years of age at the onset of the disease have significant improvement in outcome if treated with an innominate osteotomy or a varus osteotomy of the proximal femur; thus, these authors recommend surgical treatment only in this select group of patients.
Our results do not correlate with those of Herring. We found no significant change in the outcome regardless of treatment for patients with type B or type C lateral pillar involvement both under and over the age of 8 at the time of onset of the disease. We do not believe that the varus-producing osteotomy of the proximal femur has a positive influence on the disease when compared to the natural history. There was a higher percentage of a persistent limp in the patients who had undergone a VO compared to those treated non-operatively in spite of the fact that some remodeling and strengthening had taken place by the time of final follow-up. There was some residual shortening, which was slightly greater in the VO group, which may account for some of the limp.
A possible source of bias in this group of patients comes from the fact that a number of surgeons performed the varus-producing osteotomies in two different hospital units, and the possibility for surgeon variability is very high. Not all surgeons performed the osteotomy in the same way or fixed the osteotomy site with the same hardware. We believe, however, that in spite of these variables, the results obtained do show a tendency for these patients to have similar results no matter what treatment is instituted.
The standard of care for patients with LCP disease is to maintain range of motion in a contained hip in order to obtain a spherically congruent hip at skeletal maturity. The pediatric orthopedic surgeon is always challenged by these cases because there is no single consensus regarding treatment; the results that we obtained should help clinicians in making decisions when faced with a patient of these characteristics.