
Abstract
Background:
Displaced medial epicondyle fractures are treated with open reduction and internal fixation with K-wires or screws. Rates of implant prominence, failure, or non-union reported are considerable. Magnesium screws have demonstrated biocompatibility, osteoconductivity, and high pull-out strength. The aim of this study was to compare surgical fixation of medial epicondyle fracture using resorbable magnesium Herbert screws to K-wires, in skeletally immature patients.
Methods:
A retrospective analysis was performed from January 2015 to April 2020. Inclusion criteria were as follows displaced medial epicondyle fracture, <15 years, and absence of concomitant ipsilateral upper limb fractures. Two consecutive cohorts based on fixation device were made: Group A (wires) and Group B (magnesium screws). Alignment, pain, range of motion, Mayo Elbow Performance Score, and radiological healing were assessed.
Results:
A total of 27 patients were included: 15 in Group A and 12 in Group B. Groups were comparable for age and sex. Mean follow-up was higher in Group A (38.73 ± 3.15 vs 26.18 ± 4.85 months; p < 0.001). No significant differences were observed regarding range of motion, alignment, pain, and Mayo Elbow Performance Score, with excellent results in both groups. Two patients in Group A developed a deep wound pin site infection requiring antibiotics. X-rays revealed three cases of non-union in Group A and one in Group B, all of them asymptomatic. No patient required a second surgical procedure.
Conclusion:
Open reduction and internal fixation of medial epicondyle fractures with magnesium screws showed comparable results to a widely accepted procedure such as the use of K-wires, potentially with a lower incidence of non-union and infection. No adverse reactions were recorded.
Level of evidence:
level III.
Introduction
Elbow fractures are frequent in pediatric population. The medial epicondyle (ME) is involved in approximately 7% and is among the most frequent fractures of the elbow requiring surgical treatment. 1
Controversies regarding displacement measurement accuracy, imaging modality, and surgical indications have recently been raised. 2 The widely accepted treatment is open reduction and internal fixation (ORIF) with either K-wires or screws, even though there is still controversy on which one is to be considered superior. In fact, both techniques have demonstrated rates of complication up to nearly 50%, including implant prominence, implant failure, non-union/delayed union. 3 Thus, even if some author still debate on the usefulness of resorbable implants, this setting appear to be one of the clearest to demonstrate that research on biodegradable fixation can improve patients’ outcomes.4,5
Su and Nan 6 have recently published on the use of biodegradable polymer–based pins for ME fractures in children, reporting comparable outcomes as compared to K-wires. Despite being resorbable, although, biodegradable polymers are not osteoconductive and their resorption is associated with persistent osteolysis. 7
Previous studies have demonstrated that Magnesium (Mg)-based alloys appear to be biocompatible and osteoconductive. In addition, Mg-based screws showed higher pull-out strength as compared with titanium (Ti) and polylactide screws.8–10 Moreover, Young’s modulus and density of Mg is different from Ti and stainless steel, and more similar to that of cortical bone. This would reduce bone resorption around the implant due to the so-called stress-shielding phenomenon. 11
MgYREZ is the first Mg-based alloy approved for clinical use in 2013, and it is composed by Magnesium, Yttrium, Rare Earth elements, and Zirconium. It is available in various configurations: pins, standard cortical screws and Herbert-type cortical screws, and interference screws.
Despite a lack of evidence, during the latest years, an increasing number of authors published on the use of Mg screws or pins for fixation of malleolar fractures, 12 chevron hallux valgus osteotomies,13,14 intraarticular fractures 15 and other procedures, reporting results not inferior compared to standard fixation devices.
Aim of this study was to evaluate safety and efficacy of the surgical fixation of displaced medial epicondylar fracture of the humerus using resorbable Mg-based headless cortical screws as compared to K-wire fixation, in a population of skeletally immature patients.
Patients and methods
After approval of the study by the local ethics committee, the database of our department was mined for the records of all patients, younger than 15 years, who underwent ORIF of displaced ME fractures, from January 2015 to April 2020. The patients’ parents/guardians provided their informed consent to the use of the children’s medical charts.
Diagnosis, degree of displacement, age at surgery, sex, surgical procedure, clinical evaluation and radiological exams, months of follow-up (FU), and eventual complications were recorded. As routinary at our center with the use of Mg implants, peri-implant osteolysis is controlled with X-rays during standard follow-up, to assess complete resorption. Osteolysis enlargement between month 1 and month 3, cortical thinning and implant mobilization were arbitrarily considered red flags for intensifying radiological controls, even if these have not been described.
Signs of inflammation persisting for more than 3 days after surgery or appearing later were considered local reactions. All the patients implanted with MAGNEZIX (Syntellix AG, Hannover, Germany) screws and their respective parents/guardians were counseled to refer every abnormal or suspect systemic reaction occurring during the follow-up. If nothing was reported by the end of follow-up, the patient was considered to have “no systemic reactions.”
Detailed report of surgical act was obtained from hospital registry. The inclusion criteria were as follows: fracture of the ME with >5 mm displacement, patients <15 years old, and 2 years of minimum clinical follow-up. The exclusion criteria were as follows: patients lost at follow-up, concomitant fracture in the ipsilateral upper limb, and open fractures. In addition, all patients presenting with chronic intraarticular incarceration of the ME were excluded from the retrospective analysis, considering that they reach significantly lower outcomes regardless of fixation techniques.
The measured outcomes were as follows: pain measured with Numeric Rating Scale (NRSp), range of motion (ROM) of the elbow, clinical elbow alignment measured with a goniometer, Mayo Elbow Performance Score (MEPS), and time to return to sport (RS). Outcomes were evaluated at last follow-up for all patients. Time to RS was retrospectively assessed at last follow-up.
Elbow alignment was assessed prospectively at 6 months for all patients during standard follow-up. Differences <5° with contralateral elbow was considered normal. Radiological healing of the fracture was assessed with standard anteroposterior and lateral X-rays. Non-union was defined as radiolucent space interposed between humeral shaft and ME apophysis persisting 6 months after surgery. Comparative analysis between the two groups was made using unpaired T-test. A p-value < 0.05 was considered statistically significant.
Surgical technique
All surgical procedures were performed by two senior authors (M.M. and V.C.), with expertise in the treatment of pediatric trauma. The use of Mg screws for the treatment of epicondylar fractures was introduced in our institution in 2018. Since then, this became the routinary surgical treatment for these fractures, and all consecutive patients presenting with ME fractures were treated with Mg screws. This provides a sort of randomization, while implying a consistent difference in mean follow-up between groups. Thus, to minimize bias, we only considered patients with a minimum of 2 years of follow-up.
All patients were positioned supine with the affected arm abducted and externally rotated on a radiolucent table with a pneumatic tourniquet at the base of the ipsilateral limb. Surgical approach was made with a curved medial elbow incision centered over the native position of the ME. Ulnar nerve was visualized and protected in all cases, but not transposed. After identification, the footprint of the ME was debrided with a sharp curette to expose underlying cancellous bone.
In Group A, the fragment was fixed with two divergent, bicortical, K-wires of appropriate dimension. K-wires were left unburied in all cases to permit easy “in office” removal (Figure 1).
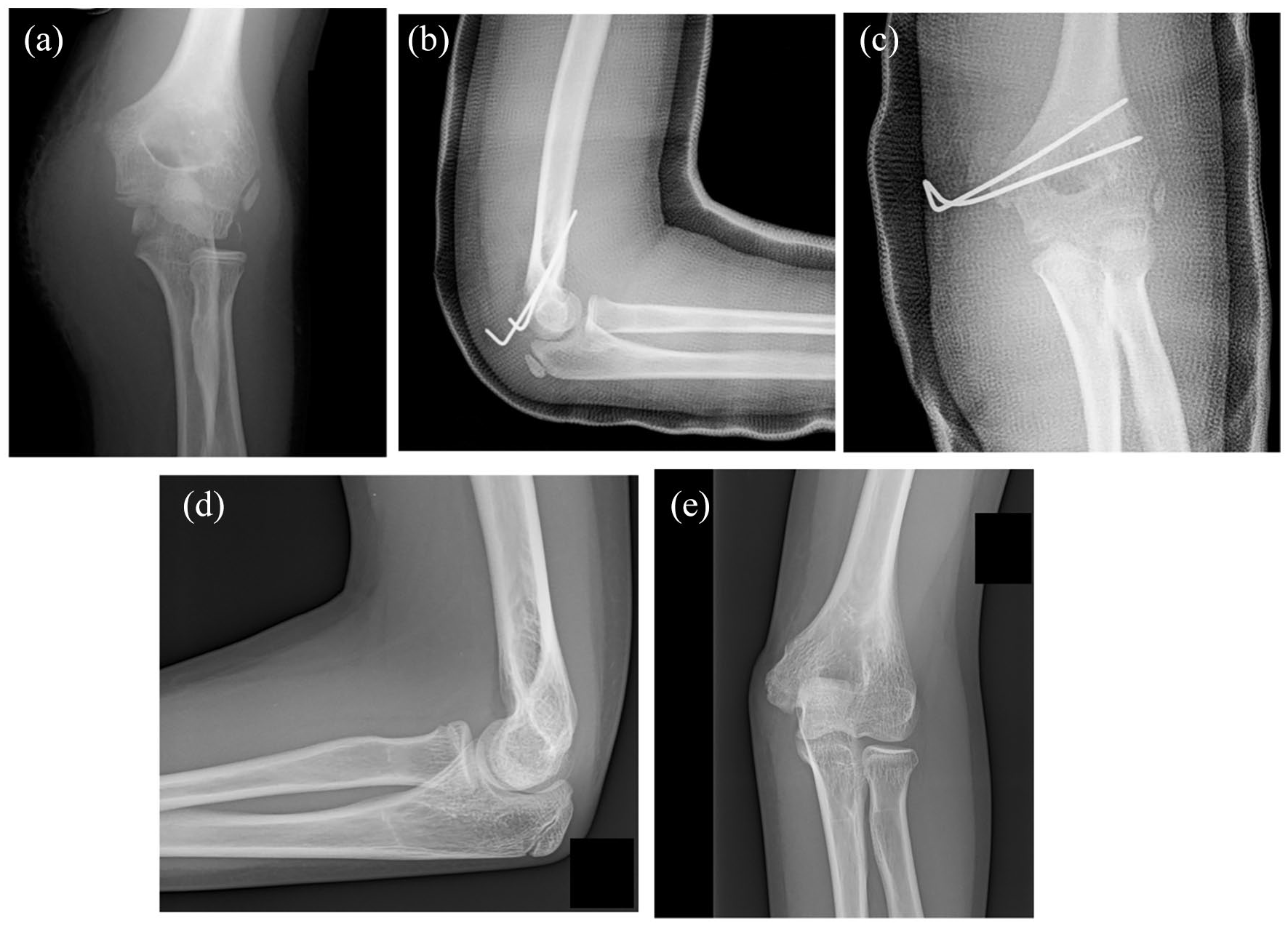
(a) Elbow dislocation with fracture of the medial epicondyle, that is incarcerated in the joint. (b and c) X-ray at 4 weeks after ORIF with K-wires. Two divergent wires are placed with bicortical fixation. (d and e) Healing of the fracture at 6 months of follow-up.
In Group B, the fragment was fixed with one or two 3.2 mm Herbert-type Mg screws (MAGNEZIX®, Syntellix AG) depending on the dimension of the avulsed fragment.
In all cases, reduction and fixation of the fragment were performed with the elbow in 90° of flexion, forearm fully pronated, and wrist and fingers fully flexed, in order to minimize tension on the flexor conjoint tendon. After surgery, patients were immobilized in cast with elbow in 90° of flexion and forearm in neutral position for 4 weeks. K-wires were removed in office between the fourth and the fifth week post-surgery. Postoperative X-ray and clinical evaluation were performed at 1 week, 4 week, 3 months, and 12 months. Free movement of the elbow was permitted after cast removing at 4 weeks, with restriction on sport for additional 4 weeks in both groups.
Results
A total of 27 patients were included in the retrospective analysis, 15 in Group A, treated with K-wire pinning, and 12 in Group B, treated with resorbable Mg screws.
Groups were comparable for age and sex. Patients in Group B had shorter mean follow-up (p < 0.001), with a minimum of 24 months. There were seven males in Group A (47%) and five males in Group B (42%). Age at surgery was 10.2 ± 1.20 in Group A and 11 ± 1.18 in Group B (p > 0.05). Patients’ demographics are presented in Table 1.
Demographics and follow-up.
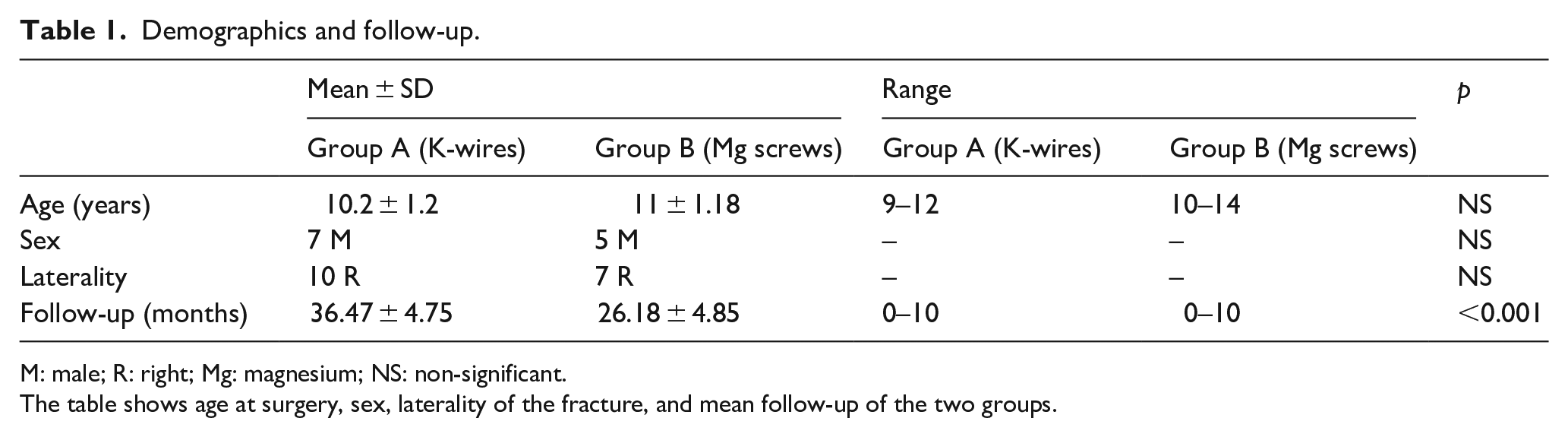
M: male; R: right; Mg: magnesium; NS: non-significant.
The table shows age at surgery, sex, laterality of the fracture, and mean follow-up of the two groups.
Clinical elbow alignment measured with a goniometer was comparable to contralateral unaffected side in all patients. Clinical outcomes evaluated with MEPS reached comparable excellent values in all patients, both in Group A (97.2 ± 5.1) and Group B (97.3 ± 4.7), with values that did not differ significantly between groups (p > 0.05). No significant differences were observed between groups regarding flexion, extension, and pronation/supination (Table 2).
Postoperative values of pain, functional outcomes, and complications.
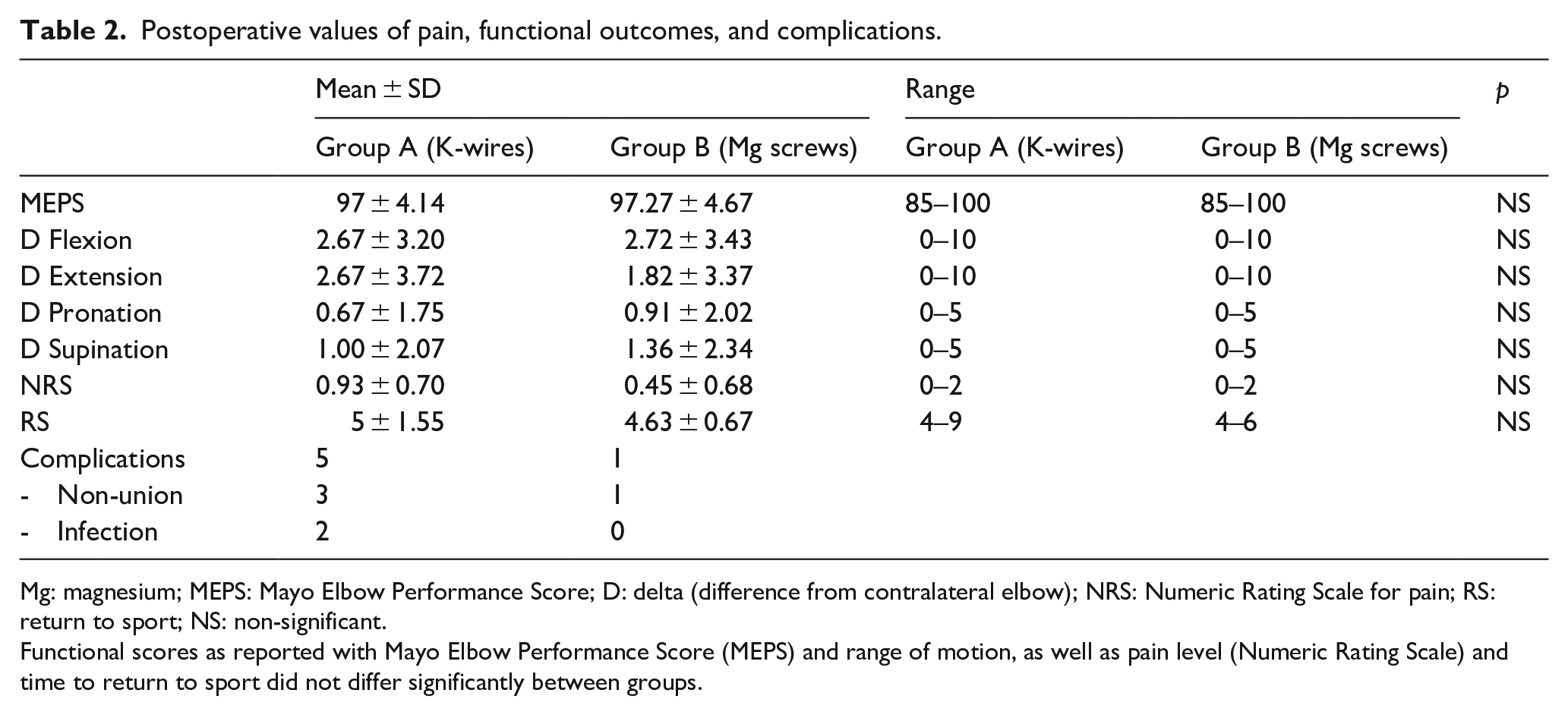
Mg: magnesium; MEPS: Mayo Elbow Performance Score; D: delta (difference from contralateral elbow); NRS: Numeric Rating Scale for pain; RS: return to sport; NS: non-significant.
Functional scores as reported with Mayo Elbow Performance Score (MEPS) and range of motion, as well as pain level (Numeric Rating Scale) and time to return to sport did not differ significantly between groups.
Mean time to RS was slightly shorter in the Mg group (5 ± 1.55 months in Group A and 4.63 ± 0.67 months in Group B), even if this difference was not statistically significant (p > 0.05). Postoperative pain was absent in nearly all patients, with persisting very low levels only reported in the two patients experiencing postoperative pin site infection.
Evaluation of postoperative routine X-ray revealed three cases of non-union in Group A (20%) and one case in Group B (8%). All cases of non-union were incidentally diagnosed in otherwise asymptomatic patients (Figure 2). Peri-implant osteolysis around Mg screws was evident at 1 month, less evident but still visible at 3 months and resolved without complications in all cases (Figure 3).
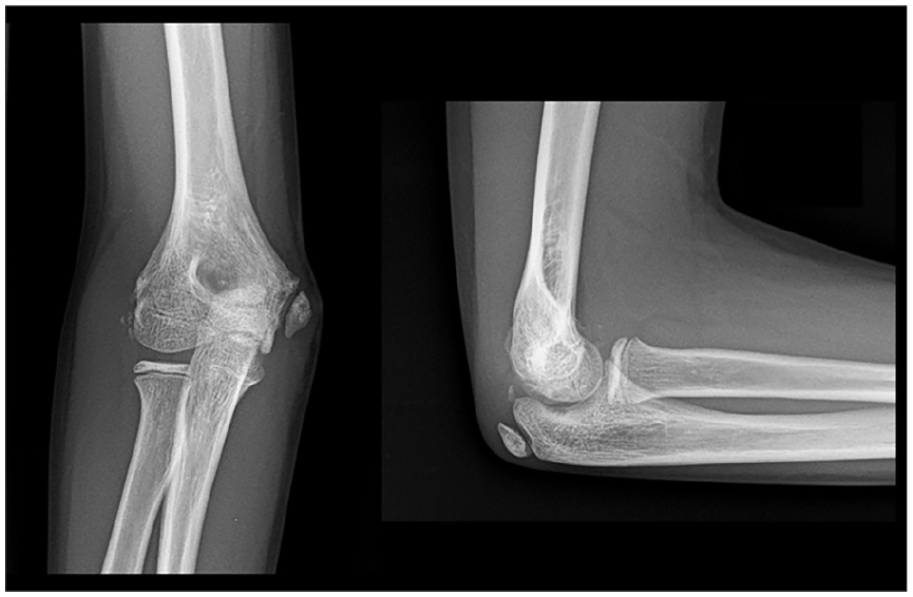
Fibrous union of the medial epicondyle 12 months after surgical treatment with K-wires. Despite the patient is completely asymptomatic and satisfied with the treatment, the uneven surfaces of the fracture site are still clearly visible.
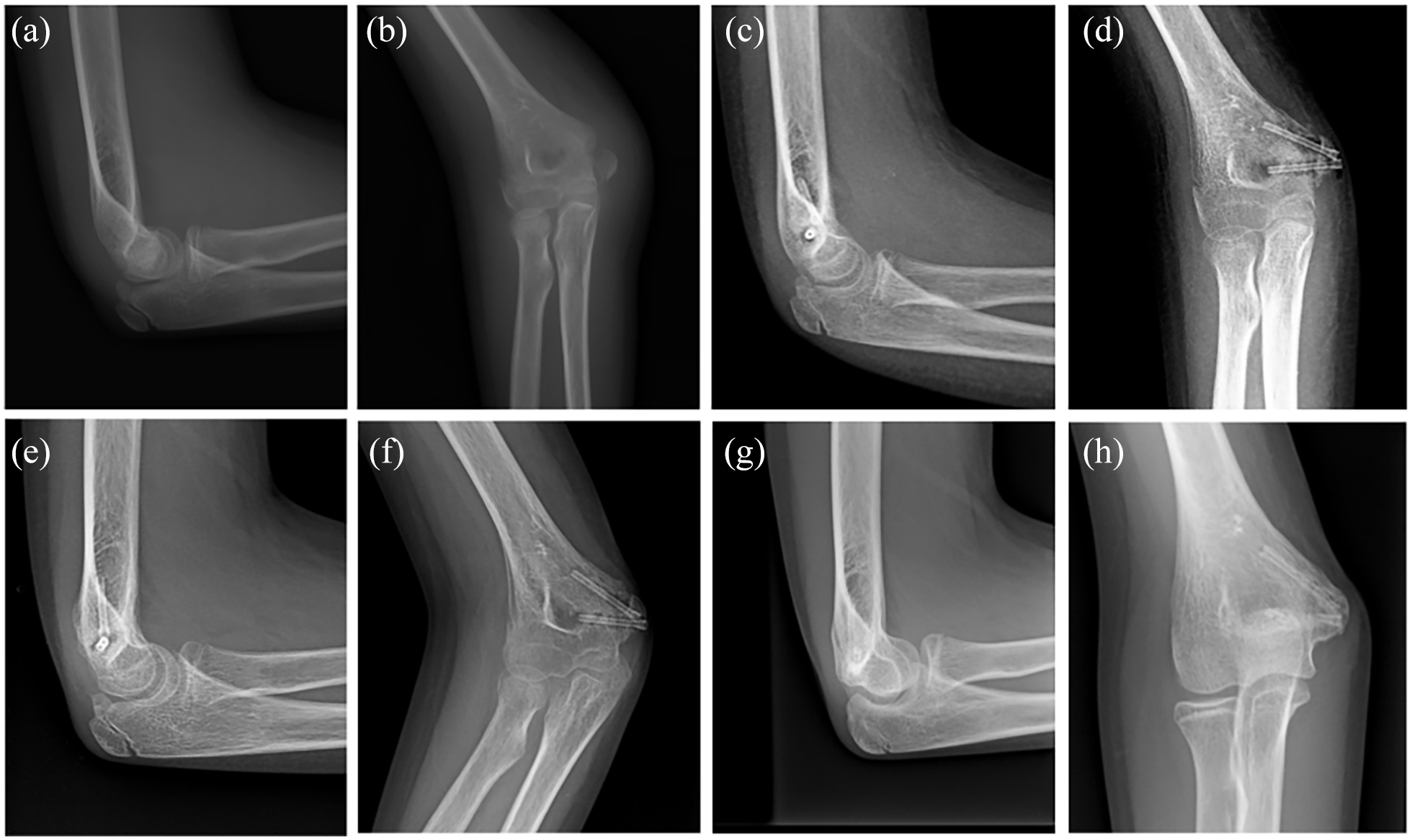
(a and b) Displaced fracture of the medial epicondyle of a right humerus. (c and d) One month after ORIF with two divergent Mg Herbert screws. Peri-implant osteolysis is limited but clearly visible. (e and f) Control X-ray at 3 months shows advanced healing of the fracture and consistent reduction of the osteolytic area. (g and h) 12 months after surgery, the fracture is no longer visible, and the screws show the advanced level of resorption.
Two patients in Group A (13%) were diagnosed with deep wound pin site infection 1 month after surgery. K-wires were removed; patients were admitted again for a short course of intravenous (IV) antibiotic, and then discharged to complete a 15-day therapy with oral antibiotics. The infections resolved without clear bone involvement or other clinically relevant sequelae, but these patients required a longer time to RS (8 and 9 months). No patients in Group B complained about local or systemic adverse reaction potentially related to Mg implant, after a minimum of 2 years of follow-up (Figure 4).
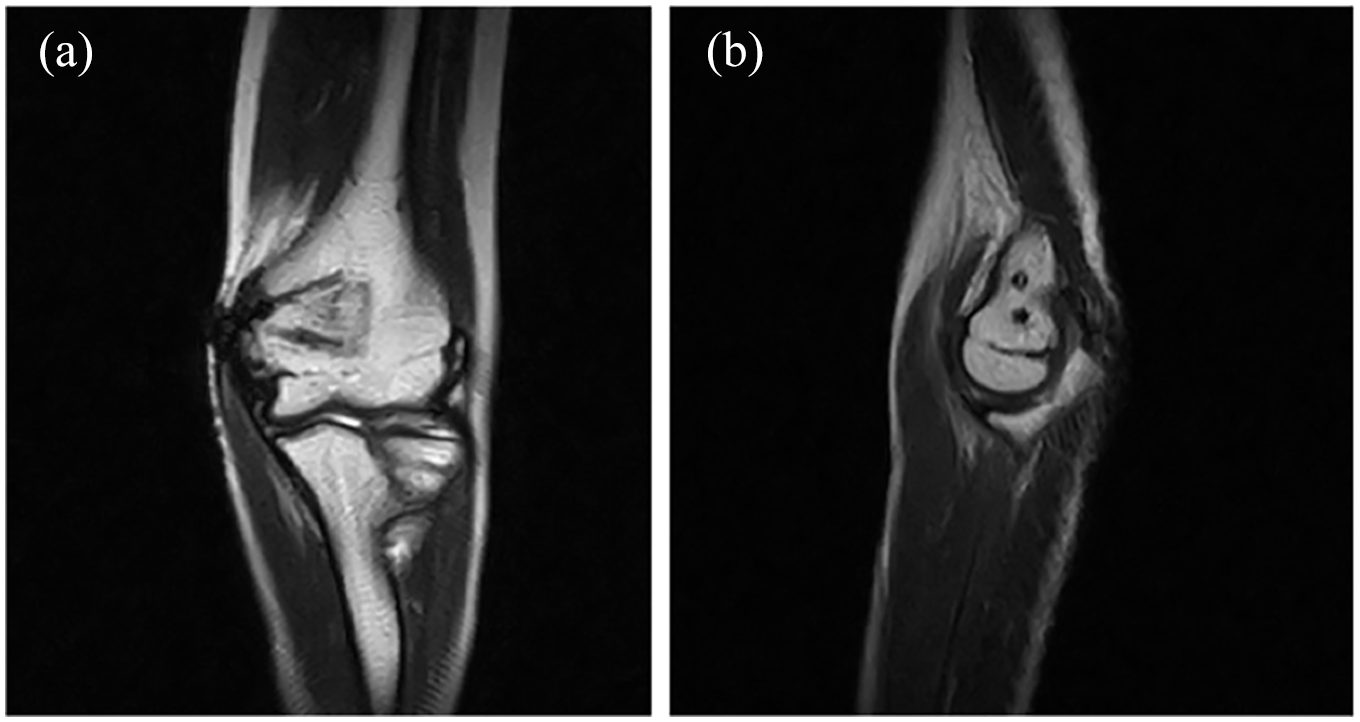
(a)-(b) Coronal and sagittal section of MRI performed 24 months after surgery show minimal distortion related to the screws, with evidence of partial substitution of the implant with marrow-like signal substance.
Discussion
To the best of our knowledge, this is the first study to compare the use of resorbable Mg screws with a standard of care like the use of K-wires, for fixation of medial epicondylar fractures. Moreover, this study is performed in a population of skeletally immature patients, where evidence on the use of these implant is even more scant. 16
This is a retrospective study comparing outcomes of procedures performed by two different senior surgeons, during a 5-year period, in children with different age and different levels of skeletal maturity. In addition, there is an intrinsic unavoidable biomechanical difference between K-wires and screws, that is, the compression torque of the latter on the bony fragments. All those features, including the obvious absence of a blind evaluation of the outcome and the relatively small number of patients, represent weaknesses. Nevertheless, the author believes that in this setting, the retrospective nature of data collection may neutralize bias arising from surgeon’s personal opinion on this implant either during the surgical procedures and the follow-up. Moreover, the presence of a control group and the relatively long term of follow-up could be considered additional strengths.
This fixation device is relatively new, and there is still not much evidence, as Baldini et al. 16 previously reported. Nevertheless, Mg alloys have demonstrated to be biocompatible both in vitro and in vivo and previously reported issues arising from high rates of degradation in vivo seem to have been overcome by MgYREZ alloying.17–19
In fact, clinical interest toward Mg-based fixation devices has recently grown, along with published literature, and since 2018, an increasing number of authors published on the use of Mg screws or pins for fixation of malleolar fractures, 12 chevron hallux valgus osteotomies,13,14 intraarticular fractures, 15 and other procedures, reporting at least not inferior outcomes compared to standard fixation devices without implant specific known adverse effects.
Thus, even if the size of groups is limited, this result is a first step in the way to the potential implementation of resorbable Mg-based implants as a standard of care for the treatment of ME fractures and, in general, other type of epiphyseal and apophyseal fractures, particularly in the skeletally immature population. In this study, we demonstrated that in the setting of ME fractures, ORIF with resorbable Mg screws is comparable with a widely accepted procedure such as the use of K-wires in terms of clinical efficacy and radiographic healing.
The use of resorbable screws may combine the advantages of the standard screws (high pull-out strength, active compression at the fracture site and absence of external implants) 9 with those of the K-wires, namely, the absence of implant intolerance and the need for a second surgical procedure to remove the implant.
Percutaneous K-wire fixation is a solid and widespread technique for stabilization and fixation of bony fragments in different situations. According to a recent systematic review from Pezzutti et al., 20 Kirschner wires are the most frequently adopted implant fixation in ORIF of ME fractures.
Wires are inexpensive and practical and can be removed with a simple ambulatory-based procedure. Nevertheless, they do not provide compression at the fracture site, with potential diastasis of the fracture, while screws in general guarantee a stable fixation, with compression at the fracture site.
From a radiological point of view, we found a higher proportion of non-union in patients treated with wires, even if this difference was not statistically significant, probably due to the reduced numerosity of the samples. None of the patients, experiencing a radiographic non-union in either group was symptomatic, and all of them reached excellent functional scores. Nevertheless, it is worth of note that some authors have reported pain, functional impairment, and valgus instability associated with fibrous union and non-union, particularly during sport.21–23
The compressive torque guaranteed by the screws could, at least in part, explain the lower rate of fibrous union reported in Group B. In addition, the osteoconductive properties demonstrated by the Mg alloy may play a role.24,25 Indeed, Mg is a resorbable implant, and it is by far not clear how the compression forces on bone fragments dissipate with time. Avoiding the use of external K-wire may significantly lower the risk of pin site infection 26 and secondary associated complications, such as osteomyelitis. 27
In our casuistry, two patients in the K-wire group developed a deep wound pin site infection which required a course of combined IV and oral antibiotics. The infections resolved without clinically relevant complications, but postoperative rehabilitation was longer and osteomyelitis could have been developed. In Group B, no patients developed surgical site infection and none required a second surgical procedure or hospital admission.
Even though fixation with K-wires and Ti screws have demonstrated comparable results, the latter demonstrated high rates of implant intolerance leading to frequent revision surgery for removal of the screws, either with or without the use of washers. 28 However, no patient in the Mg group developed implant-related complications or complained about implant intolerance. Thus, even if Mg screws are a bit more expensive at the beginning, it has been demonstrated that when taking into account second surgical procedures for implant removal, Mg devices were cheaper than standard Ti screws. 29
In conclusion, according to our results, ME fractures in skeletally immature patients can be effectively treated with resorbable Mg screws with clinical and functional outcomes comparable to a standard procedure such as the use of K-wires. Moreover, stable fixation can potentially be achieved with less morbidity and no need for second surgical intervention for implant removal. It needs to be considered that the small number of patients available for the retrospective analysis does not permit to draw firm conclusions. More studies with a higher number of patients are required to confirm the present evidence. Nevertheless, these results, are in line with growing evidence supporting that Mg screws are not inferior to standard of care for fixation of bony fragments in different orthopedics and traumatological procedures.
Footnotes
Author contributions
M.B., M.M., V.C., D.F. have contributed with the surgical procedures and the redaction of the manuscript. M.B., G.C., and D.M. have contributed to data collection and revision of the databases. A.P.G. has contributed to redaction and revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.