
Abstract
Purpose
Elastic stable intramedullary nailing is increasingly used for surgical treatment of tibial shaft fractures, but frequently requires immobilization and delayed full weight-bearing. Therefore, external fixation remains interesting. The aim was to report clinico-radiological outcomes of monolateral external fixation for displaced and unstable tibial shaft fractures in children.
Methods
All tibial fractures consecutively treated by monolateral external fixation between 2008 and 2013 were followed. Inclusion criteria included skeletal immaturity and closed and open Gustilo I fractures caused by a direct impact. Patients were seen until two years postoperatively. Demographics, mechanism of injury, surgical data and complications were recorded. Anteroposterior and lateral side radiographs were performed at each visit. Full-limb 3D reconstructions using biplanar stereroradiography was performed for final limb length and alignment measures.
Results
A total of 45 patients (mean age 9.7 years ± 0.5) were included. In all, 17 were Gustilo I fractures, with no difference between open and closed fractures for any data. Mean time to full weight bearing was 18.2 days ± 0.7. After 15 days, 39 patients returned to school. Hardware removal (mean time to union 15.6 weeks ± 0.8) was performed during consultation under analgesic gas. There were no cases of nonunion. No fracture healed with > 10° of angulation (mean 5.1° ± 0.4°). Leg-length discrepancy > 10 mm was found for six patients.
Conclusions
This procedure can be a safe and simple surgical treatment for children with tibial shaft fractures. Few complications and early return to school were reported, with the limitations of non-comparative study.
Level of Evidence
IV
Introduction
Tibial shaft fractures are common in children, and the majority of them result from falls during recreational activities that can be treated conservatively by cast immobilization with excellent outcomes, including four to six weeks of long leg cast followed by a short leg cast or a removable fracture boot.1–4 However, operative interventions are mandatory when the mechanism of injury is secondary to a direct impact that involves a skin injury with or without exposure of the fracture site, a compartment syndrome and an unstable and displaced fracture.2,5 In such circumstances, treatment must provide correct reduction and stability and the possibility to control wound healing.
Two main surgical techniques have been reported to be effective in treating tibial shaft fractures in skeletally immature children: internal fixation (elastic nails and screws) and external fixation.5,6 Screw internal fixation is a suitable option, but is not stable enough to be used alone and requires supplemental long leg cast application. Elastic stable intramedullary nailing (ESIN) has been commonly used since it provides stability, flexible mobility and is usually performed by closed reduction.7–11 Several major complications such as compartment syndrome, malunion, nonunion, leg length shortening and nail migration have been allocated to the use of ESIN compared with external fixation.12–16 Therefore, the latter procedure has often been recommended for unstable patterns with associated injuries (open fractures, compartment syndrome, head injury, polytraumatisms).5,17–19 However, several complications (nonunion, delayed union, malunion, pin infections and re-fracture) have also been frequently reported, meaning that physicians currently prefer ESIN.5,17,20,21
The aim of this study was to report clinical and radiological outcomes of monolateral external fixation associated with open reduction for displaced and unstable tibial fractures in skeletally immature patients. The hypothesis was that the monolateral fixator should remain a good alternative to ESIN in tibial fractures with early return to weight-bearing and few encountered complications.
Materials and methods
Patients
All consecutive tibial shaft fractures secondary to a direct impact or a high-energy traumatism were treated by monolateral external fixation after open reduction between 2008 and 2013. Inclusion criteria were: skeletally immature children with a displaced and unstable, closed and/ or open Gustilo I fracture. Children with history of lower extremities fractures, skeletal congenital diseases and systemic or metabolic diseases were excluded. Primary outcome was defined by the success of bone healing assessed by the lack of residual pain associated to radiological bone healing. Secondary outcome was defined by the presence of major complications: nonunion, bone infection and malunion > 10°. Informed consent was obtained from all individual participants included in the study. All data was collected after approval by the local ethic committee. Patient charts included demographic data, mechanism of injury and surgical data.
Surgical treatment
After failure of closed reduction, open reduction as minimal as possible and osteosynthesis by external fixation was performed in all patients. External synthesis used the monolateral dynamic axial external fixator (Limb Reconstruction System; Orthofix SA, Verona, Italy) that required correct alignment of the fracture before pin insertion. No angulation was possible by the device. Therefore, reduction was performed through a 4 cm to 5 cm anteromedial minimal approach, to avoid secondary skin necrosis. The reduction was maintained using a temporary four-holes plate (without inserting screws), slid through the incision, in contact with the periosteum, and held by two close bone pliers in order to stabilize the fracture before pin insertion. A minimum of four bicortical pins were placed anteriorly under fluoroscopic control, with two proximal and two distal pins using the provided alignment grid for connection of the fixator body. Patients with an open fracture received intravenous prophylactic antibiotics (Amoxicillin/clavulanic acid 80 mg per kg/days) upon arrival in the emergency department and continued until 48 hours postoperatively. Debridement procedures were performed in all of these patients before reduction and stabilization.
Clinical outcomes
Care consisted of daily pin dressing with sterile saline solution until complete wound healing. After 15 days, the patient was allowed to take a shower with the external fixator. At the first postoperative visit (seven days) swelling was resorbed, the patient was allowed to progressively bear weight by using crutches (according to the pain) and was authorized to go back to school. During the third postoperative visit, all patients were asked to report the number of days until full weight-bearing without crutches. When fracture healing was successfully obtained on radiographs, hardware removal was performed in the outpatient clinic visit under analgesic gas (inhaled nitrous oxide oxygen mixture) by the orthopaedic surgeon. Weight-bearing was immediately authorized after removal and was conditioned by the use of crutches, again according to potential pain and risk of re-fracture related to the pin removal. The patient decided himself when he was ready to walk without them. Clinical outcomes recorded residual pain based on painkiller consumption, return to school (< 15 days) and early and late complications such as revision surgery, pin track and bone infections, and re-fractures.
Radiographic outcomes
Anteroposterior and lateral radiographs were performed pre- and perioperatively. Then, patients were followed on a regular basis at one week, two weeks, six weeks, three months, six months, one year and two years postoperatively. Full-limb biplanar 3D reconstructions stereoradiography (EOS Imaging, Paris, France) looking for leg-length discrepancy (LLD) was performed only for the two-year postoperative visit. 22 Radiographs were analyzed to determine initial fracture location (proximal third, middle third or distal third) and type (transversal, oblique or comminuted), to assess postoperative alignment, to follow fracture healing and to assess final LLD and angulation. The patient was considered to have a successful union and healing if there was minimal to no pain with full weight-bearing and evidence of bridging callus on three of four cortices on radiographs. Delayed union was defined as the lack of radiographic bone union at six months postoperatively. Malunion was defined as significant if the residual deformity exceeds 10° of angulation in the coronal and/or sagittal plane.
Statistical analysis
This was performed using Stata 14.0 (Stata Corp., College Station, Texas). Numerical data was expressed as means ± standard error of the mean (sem). A Shapiro-Wilk test was performed to assess data distribution. Group comparisons used a two-tailed Student's t-test for variables with normal distribution. A 2-sample Wilcoxon test was performed for the non-parametric data. Statistically significant results were accepted as valid with a significance of p < 0.05.
Results
Patients
A total of 45 patients were included (33 men, 12 women), but nine patients were lost to follow-up. Two fractures occurred in the proximal third, 23 in the middle third and 20 in the distal third (Table 1). Forty tibial fractures were associated with a fibula fracture. Mean age at surgery was 9.7 years ± 0.5. The most common mechanism of injury was direct impact (95%) including 36 pedestrians struck by a motor vehicle (Fig. 1). In all, 17 patients had associated Gustilo I open fractures. Three patients were diagnosed with compartment syndrome preoperatively.
Patient demographics
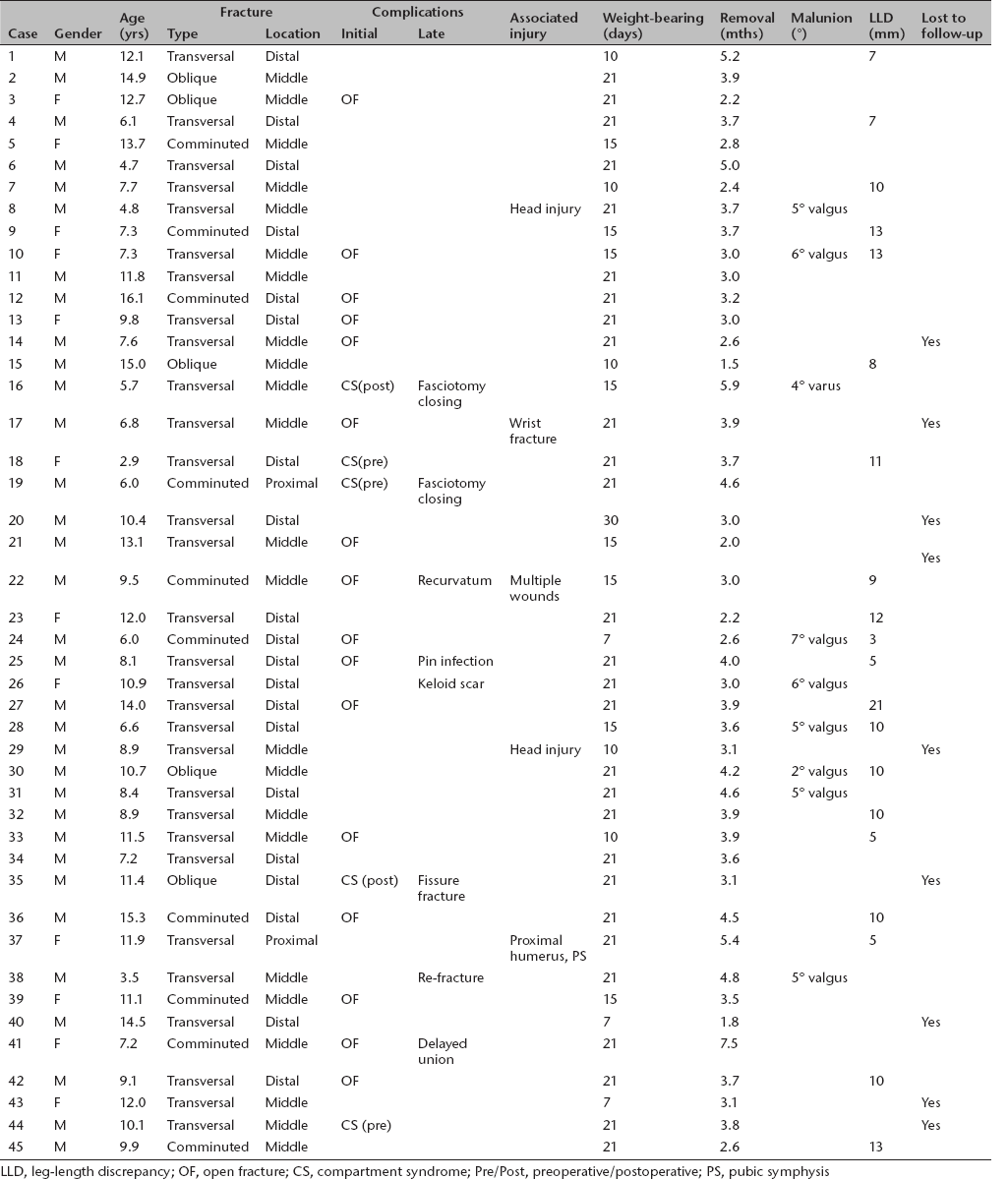
LLD, leg-length discrepancy; OF, open fracture; CS, compartment syndrome; Pre/Post, preoperative/postoperative; PS, pubic symphysis
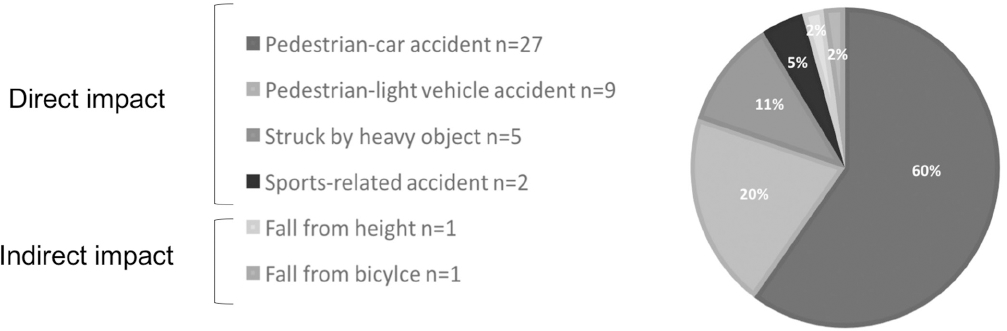
Mechanism of injuries chart.
Clinical outcomes
Mean length of hospital stay was 5.9 days ± 0.4 (3 to 14), with no difference between open and closed fractures (mean time 5.7 days ± 0.7 and 5.9 days ± 0.5 respectively, p = 0.5). Mean time to full weight-bearing from initial injury without crutches was 18.2 days ± 0.7 (p = 0.9 for open versus closed fractures). For 39 patients (87%) return to school was possible before 15 days (Fig. 2). Three children (less than six years) were not enrolled in pre-school before the injury and continued to be kept at home. Ten patients were send to a rehabilitation centre postoperatively for medical supervision, which is a common practice in France. Three patients had associated injuries requiring staying in bed. Seven came from poor social backgrounds and were living in low hygienic conditions, requiring close medical monitoring. However, during the period of rehabilitation, children had access to school. Return to the operating room for implant removal was not required.
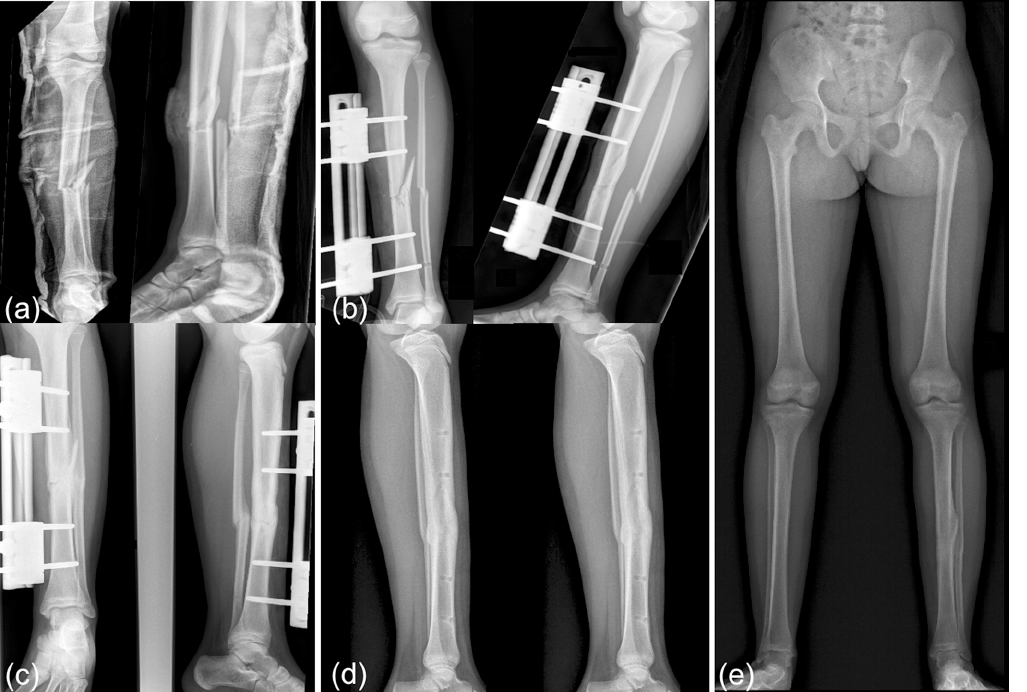
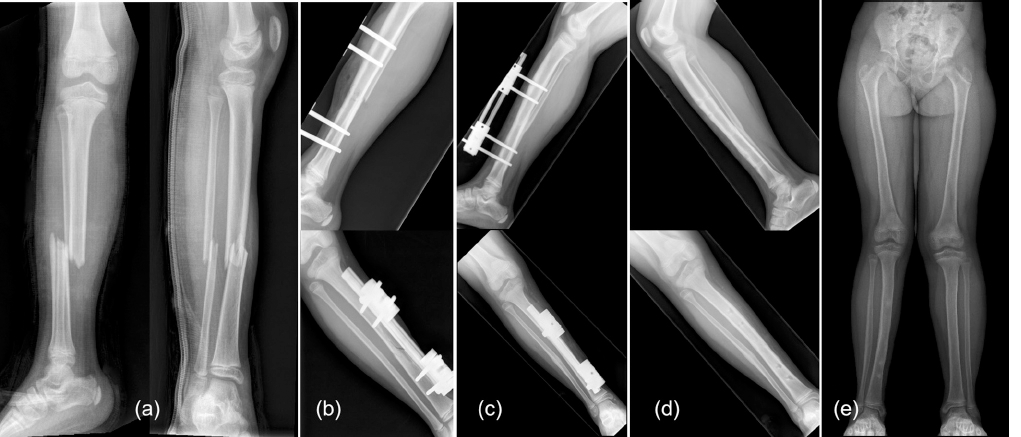
Girl, 11-years-old struck by a car, Gustilo I fracture with good outcome: (
Six patients required secondary surgical interventions: fasciotomy for postoperative compartment syndrome (two patients), repeat dressing for gradual fasciotomy closing (two patients), re-manipulation after unacceptable remaining recurvatum diagnosed two weeks postoperatively (one patient) and plastic surgery for unaesthetic keloid scars in one case. One patient was treated for 48 hours with intravenous antibiotics for pin infection. One patient presented with pain requiring grade I painkillers at three- and six-month follow-up but had no residual pain after one year. There was one case of re-fracture after another injury occurring three months after hardware removal and treated bv cast immobilization. For one patient, a fissure fracture occurred after another direct impact two years later.
Radiographic outcomes analysis
All children achieved radiographic union by final follow-up. The mean time to union was 15.6 weeks ± 0.8, with no increased delay for open fractures (p = 0.1). Only one patient showed a delayed union (32.9 weeks) that resolved spontaneously (Fig. 3). No fracture healed with > 10° of angulation in the coronal plane (ten patients, mean 5.2° ± 0.5°, three with > 5°) and none required corrective osteotomy (Table 2). No patient had sagittal plane misalignment.
Boy, 11.5-years-old struck by a scooter, good outcome despite delayed union and Gustilo I fracture: (
Clinical characteristics of patients with leg-length discrepancy (LLD) > 10 mm and malunion > 5°. Only one case of malunion > 5° occurred with no significant LLD

For 20 patients, LLD was found on stereoradiographic measures (mean 9.6 mm ± 0.9 mm) (Fig. 4). LLD > 10 mm was found in 13% (one patient > 20 mm, five patients > 10 mm, mean age 7.9 years ± 1, 3.5 to 11.8). A contralateral epiphysiodesis was offered to the patient with 21 mm discrepancy. He was asymptomatic and declined treatment.
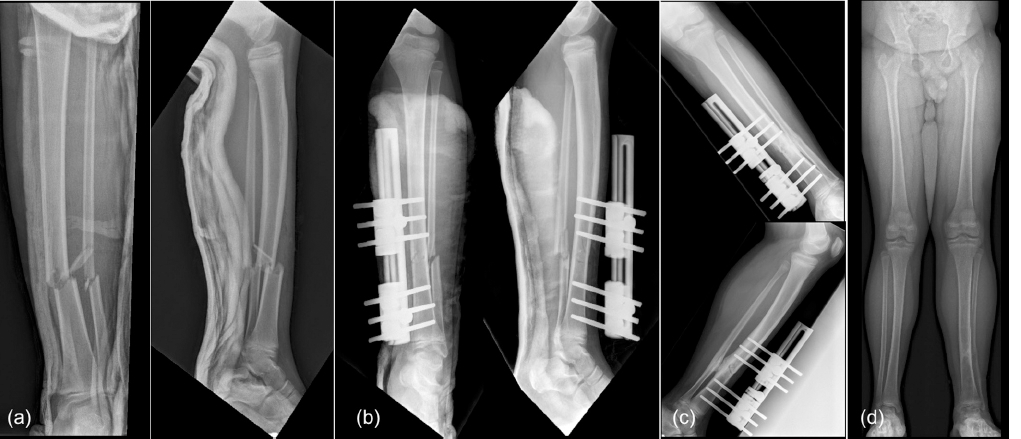
Girl, 7.3-years-old struck by a scooter, poor outcome: (
Discussion
Tibial shaft fractures are common in paediatric traumatology and mostly treated without operative intervention. 2 However, surgical stabilization may be required for unstable and displaced fractures, compartment syndrome and skin injury with or without opening of the fracture site.2,5 Although ESIN rapidly became the most common technique used for surgical treatment of diaphyseal long bones fractures, tibial shaft fractures showed a higher rate of complications than femoral shaft fractures.11,13,15 Monolateral external fixation has been reported to be a simple and effective procedure in the treatment of displaced tibial fractures in children.18,23,24 However, risks of pin infection, nonunion, loss of reduction and re-fracture have tempered their use.
Patients characteristics
Pedestrian struck by a vehicle was the major mechanism of injury (80%). For 87%, fractures were transversal or comminuted and involved both the tibia and the fibula except for in six cases. These factors are at higher risks of compartment syndrome, varying from 12% to 32%.8,14,19 Pandya et al 14 have also suggested that ESIN might potentially contribute to increasing that risk. Their study showed a rate of nearly 20% of postoperative compartment syndrome, particularly for comminuted fractures and high energy traumas.
Surgical procedure
The current procedure was chosen since anatomical reduction is necessary in order to be able to put on the device. Immediate stability and the opportunity of early weight-bearing are therefore possible. Furthermore, fasciotomy can be directly performed if necessary and skin surveillance is practical. However, when closed reduction fails, the monolateral fixator requires an open reduction and periosteum opening. 25 Indeed, no angulation is possible with the device that is designed as a track. The advantage is that it provides stress-shielding forces absorption, preventing secondary displacement and allowing early weight-bearing. 25 Closed reduction might be difficult because of the anatomical shape of the tibia and the presence of the fibula and periosteum or soft-tissue incarceration. Therefore, open reduction is also recommended after three to four attempts at ESIN, rates of open reduction required with the ESIN technique varying from 33% to 60%.8,11,13,14 As a matter of fact, repeated closed passing of nails created soft-tissue damage and swelling, which also increased the risk of compartment syndrome. 11
Clinical outcomes
Mean time of hospital stay was comparable with previous reports, regardless of the type of surgical treatment.15, 26 Weight-bearing was allowed after seven days until the swelling resorbed. In our series, we did not find any loss of reduction as seen in the series reported by Gordon et al. 23 In their study, the fracture's initial displacement was not mentioned and at least nine open reductions were not performed in 30 patients treated with a monolateral external fixator; that might explain the six patients with a secondary loss of reduction after using a monolateral external fixator. Regarding ESIN, data are unclear on whether the patients should or should not be weight-bearing, with time varying from seven days to seven weeks postoperatively.10–12,20 However, Lascombes et al 12 do recommend three weeks of cast immobilization.
Risk of re-fracture is frequently associated with the use of external fixators, but that was not supported by our results.17,18,23,24 The only case was secondary to a new injury occurring three months after hardware removal.
Radiological outcomes and complications
Bone healing was achieved for all patients. Mean time to union was similar to the literature (mean time to union: 18.5 weeks versus 15.6 weeks in our study), which has been reported to vary from 7 weeks to 31.5 weeks for ESIN and from 9.4 weeks to 27.7 weeks for external fixators.5,23,25–27 However, time to union in surgically treated tibial shaft fractures is longer than in fractures treated non-operatively since time to union varied from 13 weeks to 18 weeks for the latter.3,28
Conversely to previous studies which have reported healing complications rates as high as 66%, only one delayed union was found as well as one pin-track infection.5,20,23 We also found no cases of nonunion. However, these complications might be influenced by fracture type and mechanisms of injury rather than the type of osteosynthesis.9,13,20,23
Conversely to Gordon et al 23 and Myers et al, 5 the present study found no case of major malunion, and this emphasizes the stability of the device, even though it is also associated with early weight-bearing. Rates of malunion are variable in literature for ESIN, ranging from 0% to 21%.8–10,13,15 For this reason, many authors have recommended the use of additional protection with cast immobilization.9–12
Our LLD rate (> 10 mm) was higher than other studies using an external fixator for treatment.9,13 Each patient had particular characteristics prone to develop LLD, but these were inherent in childhood fractures and corresponding to biological overgrowth.10,16 Lee et al 16 reported 70% of LLD > 10 mm after ESIN and showed that age and male gender were factors correlated to the risk of developing LLD. Pandya 11 also reported 21% of LLD in open fractures treated by ESIN.
Limitations
The study has several limitations. Nine patients were lost to follow-up, perhaps because of a lack of satisfaction. The use of an external device may not be tolerated well by patients and their parents. Montpetit et al 29 showed a lower quality of life for the physical health and psychological functioning subscales using the Pediatric Quality of Life Inventory 4.0 Generic Core Scales (PedsQL) in children with congenital LLD. Therefore, a score which collected patient and parent satisfaction could have been used, even though there was no patient with residual pain, or limping at the final follow-up. Furthermore, the time to non-limping, which is an external sign of dysfunction along with the evaluation of the scar's appearance (one patient developed keloids requiring plastic surgery) were also not evaluated. Kubiak et al 20 have reported an increased level of satisfaction in the ESIN group compared with the external fixator group. Nonetheless, the current study encountered less bone healing complications than Kubiak's. Finally, the study is not comparative. Therefore, the superiority or the inferiority of our technique cannot be evaluated. However, the study focuses on the advantage of early weight-bearing and the lack of major complications. Furthermore, few studies have compared monolateral external fixation to other osteosynthesis.20,23,27 Indication for allocation to one or another group was not clearly defined, as well as the type of fracture treated by each method. Kubiak et al 20 also assigned more open fractures to the external fixator group, which are prone to poorer outcomes. Further randomized investigation comparing both techniques should be performed, including a PedsQL assessment.
Monolateral external and axial fixation can be a safe and simple procedure for the treatment of displaced tibial shaft fracture at risk of compartment syndrome in skeletally immature children. It provides good stability without secondary displacement and reliable bone healing, with relatively few complications. The main benefits remain early weight-bearing and early return to school, which is of particular interest in a time of need for increased reduction of societal costs.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
K. Mazda declares they are a consultant for Implanet. B. Ilharreborde declares they are a consultant for Implanet, Zimmer Spine, Medtronics and EOS Imaging. All other authors declare no conflict of interest.