
Abstract
Osteomyelitis of the pubic symphysis is a rare infectious disease commonly caused by the opportunistic bacteria Staphylococcus aureus and Pseudomonas aeruginosa. The clinical context includes fever, and pubic, or abdominal pain, thus should prompt a biological, microbiological, and radiological assessment. We report the case of a 16-year-old patient who developed inflammatory pygalgia in a febrile context laboratory examination showed an elevation of C-reactive protein and sedimentation rate. Pelvic X-rays and magnetic resonance showed bilateral bone lysis and destruction of the edges of the pubic symphysis, in addition to a pubic pelvic collection. Bacteriological examination revealed by methicillin-sensible S. aureus. The patient was put on antibiotic therapy for 2 months with good clinical and radiological evolution without surgical debridement. In conclusion, osteomyelitis of pubic symphysis can be misdiagnosed because of its atypical manifestations. Recovery is often achieved if adequate treatment is started early.
Introduction
Osteomyelitis of the pubic symphysis is a rare infectious disease commonly caused by the opportunistic bacteria Staphylococcus aureus and Pseudomonas aeruginosa.1–4
It occurs in the majority of cases among athletes, drug addicts, or after surgery on the small pelvis as female incontinence surgery.1,5
Its diagnosis is often difficult given the variety and non-specificity of the symptoms, delaying its therapeutic management.5–7
Case
A 16-year-old boy was hospitalized in rheumatology for bilateral inflammatory lumbopygalgia in a febrile context. In fact, initially, he had abdominal pain for which the diagnosis of appendicitis was suspected however the abdominal echography does not show specific signs. His symptoms began 2 weeks before his hospitalization following a trauma during a sporting activity, resulting in a wound of 1 cm depth in his left thigh. The wound was treated with antiseptic application. On examination, the patient was 37.7° and the lumbar spine was stiff. Sacroiliac shear maneuvres were negative and hip examination was normal. In addition, the patient reported pain on mobilization of the right shoulder radiating to the ipsilateral chest wall. Blood screenings showed a biological inflammatory syndrome with a C-reactive protein (CRP) at 142 mg/L and a sedimentation rate (SR) at 115 mm/h. Infectious investigations (cytobacteriological examination of urine, three series of blood cultures, syphilitic, brucellian, and chlamydia trachomatis serologies as well as the search for Koch’s bacilli in sputum and urine) were initiated and proved negative. On the radiological assessment, the chest radiograph was normal. The pelvis radiography (Figure 1) showed osteolysis of the left side of the pubic symphysis. A pelvic magnetic resonance imagery (MRI) was done showing significant bilateral bone lysis and destruction of the edges of the pubic symphysis in high signal T2 (Figure 2(a)) with enhancement after gadolinium (Figure 2(b)), in addition to a bilobed thick-walled retro pubic pelvic collection in hypo T1, hyper T2 with enhancement after gadolinium injection (Figure 3(a)). The MRI also showed evidence of an ascending blind fistulous path originating opposite the pubic symphysis and extending over 23 mm (Figure 3(b)) with a secondary orifice located subcutaneously opposite the rectus abdominis muscles. A bone scintigraphy (Figure 4) was performed in search of other septic locations, which resulted in the discovery of a double infectious location: the pubic symphysis and the first right rib. A scan-guided biopsy (with a 64-bar, 128-slice scanner) of the pubic symphysis was performed, its histological examination showed moderate chronic and acute osteitis and the bacteriological examination revealed methicillin-sensible S. aureus (MSSA). The patient was put on ciprofloxacin 1 g × 3 per day and fusidic acid 500 mg × 3 per day for a total of 2 months which resulted in an effective clinical and biological evolution (disappearance of pain and significant improvement in mobility and a drop in CRP and SR). A computed tomography (CT) scan of the pelvis performed to monitor the recovery 1 month after treatment showed irregularity and widening of the chondral surface of the right first rib and of the articular edges of the pubic symphysis without significant infiltration or adjacent collection. The patient consulted us, 3 and 6 months after the end of antibiotic therapy, he was apyretic with perfectly normal walking, he no longer had pain and the biological tests did not show inflammatory syndrome.

Pelvis radiography showing osteolysis of the left side of the pubic symphysis (black arrow).
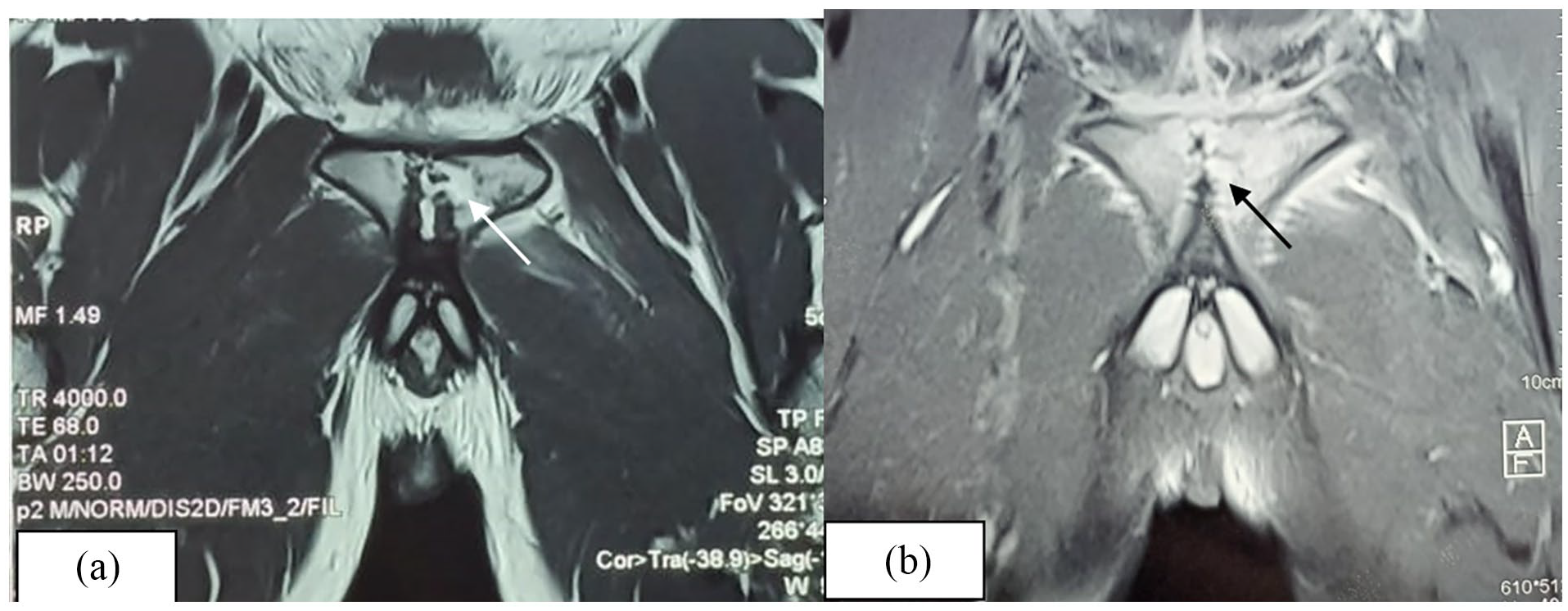
Coronal section of pelvis MRI showing significant bilateral bone lysis and destruction of the edges of the pubic symphysis in high signal T2 (a, white arrow) with important enhancement in T1 fat-saturated post-contrast sequence (b, black arrow).

Coronal section of pelvis MRI T1 fat-saturated post-contrast showing a bilobed, thick-walled retro pelvic collection (a) and an ascending blind fistulous path originating opposite the pubic symphysis and extending over 23 mm (b) with a secondary orifice located subcutaneously opposite the rectus abdominis muscles.
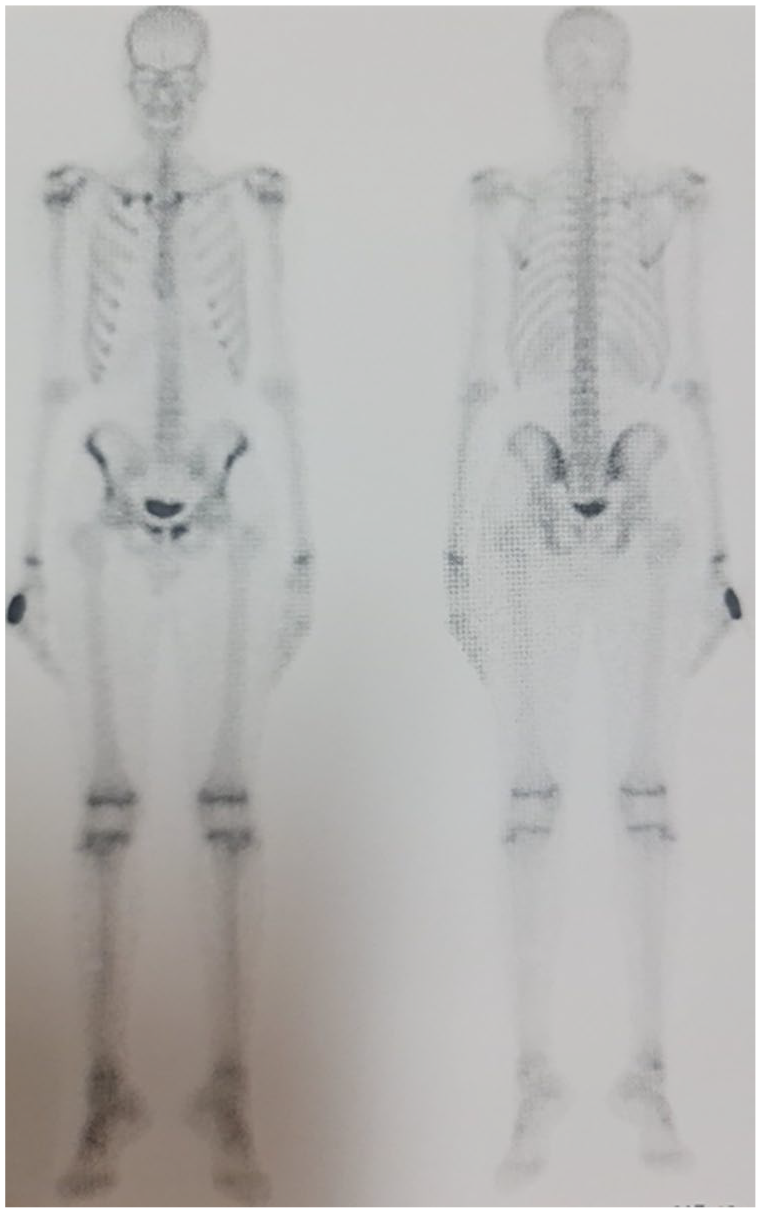
Bone scintigraphy revealing double infectious location: the pubic symphysis and the first right rib.
Discussion
The pubic symphysis is an original joint made of a vertical fibro-cartilaginous disk sandwiched between two layers of hyaline cartilage. 2 As with the intervertebral discs, it must withstand compressive stress, as well as shear and torsion.2,8
Pathologies of the pubic symphysis are grouped under the term “pubalgia,” 2 whose etiologies are varied: mechanical, iatrogenic, rheumatic, infectious, and tumoral.
Osteomyelitis pubis is a rare disease and represents less than 1% of all cases of osteomyelitis. 7 To date, only about 200 cases have been described. 9
There are often conditions that promote the development of an infectious pubic symphysis such as a uro-gynecological intervention (radical prostatectomy, incontinence treatment, inguinal hernia repair, etc.), all obstetrical procedures, intravenous drugs use, and less frequently mechanical causes such as pregnancy and in athletes. 3
The symptomatology of this pathology includes fever, pubic tenderness, and painful hip mobility, but the clinician must also consider inguinal or abdominal pain which worsens standing or walking. 5 This varied and nonspecific clinical presentation may delay investigations and treatment.5–7 In our case, fever, pubic pain, and the presence of a cutaneous entry point led us to consider pubic osteomyelitis.
Biology does not always show anomalies. The biological inflammatory syndrome that was been present in our patient is neither specific nor constant. 3 Only 35% of patients in Ross and Hu’s study had an increase in white blood cells greater than 11,000.
For imagery, the standard X-ray of the pelvis is usually performed in the first instance. 3 It may show after a period of 2–4 weeks a widening of the joint space with blurry edges and erosions.2,3 Later on, osteo-condensation and periosteal appositions appear, sometimes leading to a synostosis. 3 Standard X-ray is also useful to exclude differential diagnoses.2,5
The CT scan, which is more sensitive and precise, allows for a better visualization of the invasion of the soft tissues, a bone sequestrum, an abscess or potential complication and to guide a biopsy. 3
MRI is the gold standard in terms of sensitivity.2,5 It allows early detection of edema and inflammation of bone and muscle, intra-articular effusion or abscess. 3
The scintigraphy can show hyper fixation which is not specific but it may be useful in ruling out differential diagnoses2,3 or revealing a bone lesions cartography as in our patient.
The rarity and nonspecific clinical presentation of this condition can make diagnosis challenging, particularly in young patients without a surgical history. Common conditions such as osteitis pubis must be considered in the differential diagnosis. Osteitis pubis, often seen in athletes and characterized by chronic pelvic pain exacerbated by activity, is typically non-infectious and mechanical in origin. In contrast, pubic symphysis osteomyelitis may present with systemic symptoms like fever, elevated inflammatory markers, and worsening pain with movement. 3
Clinicians should consider pubic symphysis osteomyelitis, especially in cases where there is unexplained pelvic pain, fever, or elevated inflammatory markers that persist despite initial treatment for more common conditions. Early advanced imaging, such as MRI, should be considered when symptoms are persistent or severe, or when initial investigations are inconclusive. 3
It is always necessary to seek the responsible germ. It can be isolated in blood cultures, or lochia within the post-partum, otherwise we can suggest a local biopsy whether surgical or using trocar. 3 The germ most commonly responsible is S. aureus, especially in athletes with a cutaneous entry point as in our case. In the study by Ross and Hu, the germ was found in 100% of patients and S. aureus was the responsible germ in 34% of total cases and in 17 out of 19 or 89% of athletes. 4
But several other germs can be isolated such as P. aeruginosa (particularly in drug addicts, and after urological surgery), Escherichia coli, Proteus mirabilis after urological surgery, Streptococcus B and anaerobic germs in postpartum. 3
It has been published in literature that long-course intravenous and/or oral antibiotic therapy can effectively treat patients with osteomyelitis of pubis symphysis, particularly in localized forms as in our patient.1,3,10
Therefore, regarding antibiotic therapy, initial empirical treatment often includes broad-spectrum antibiotics, as was the case in our patient who received ciprofloxacin and fusidic acid. The choice of ciprofloxacin was driven by the need to cover a broad range of potential pathogens, including Pseudomonas, given the severe presentation and the initial absence of culture results. Fusidic acid was selected for its effective bone penetration and activity against MSSA, aligning with local antimicrobial susceptibility patterns. Once MSSA was identified, the treatment was adjusted to target this organism specifically. While beta-lactam antibiotics like penicillins or cephalosporins are typically first-line treatments for MSSA, fusidic acid was chosen due to local resistance patterns and considerations of drug penetration into bone. The decision to continue ciprofloxacin initially, despite cultures showing MSSA, was based on the need to ensure broad coverage until the infection was clearly delineated and susceptibilities were confirmed.
The overall duration of treatment is not clearly established, but a minimum of 4 weeks is commonly accepted.5,11 A need for a several-week extension may be necessary depending on clinical and biological evolution. 3 However, when an abscess develops, surgical intervention is usually needed. 6 In Ross and Hu’s study, >50% of patients require surgical intervention. 4 In cases where surgical intervention is necessary, debridement and drainage of abscesses are essential to remove necrotic tissue, reduce bacterial load and restore vascularity maximizing the effectiveness of systemic antibiotic therapy. Additionally, the potential for the formation of sequestra or biofilm in chronic osteomyelitis may necessitate surgical removal to prevent recurrent infections and ensure complete release. When appropriate treatment is initiated early on, healing is often achieved.3,4 In our case, surgery was not deemed necessary, as the CT scan performed 1 month after treatment showed radiological improvement.
Long-term monitoring should include periodic clinical evaluations and imaging to detect any signs of recurrence early and to assess for any long-term complications, such as chronic pain or functional limitations.
Conclusion
Osteomyelitis pubis represents less than 1% of all cases of osteomyelitis. Because of the variability of symptoms it presents, this affection can be misdiagnosed and atypical manifestations may lead to unnecessary investigations and delayed treatment. MRI is the gold standard for early diagnosis of arthritis of the pubic symphysis. The treatment is based on long-course antibiotherapy but in case of non-response surgical debridement may be considered.
Footnotes
Acknowledgements
None.
Author contributions
R.B. draft writing. A.F. draft writing. I.S. conception. C.Z. draft writing. Z.G. data collection. S.B.D. data collection. M.E. conception. M.H.K. supervision. H.F. supervision. S.B. supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the legally authorized representative of the patient for their anonymized information to be published in this article.