
Abstract
Purpose
To evaluate sensitivity, specificity and accuracy of a radiographic slipped capital femoral epiphysis (SCFE)-diagnosis among medical specialists.
Methods
Three paediatricians, three paediatric radiologists and three paediatric orthopaedic surgeons completed two rounds of a survey of anteroposterior and frog-leg lateral radiographs of patients with a diagnosis of SCFE (25), femoroacetabular impingement (four), Legg-Calvé-Perthes (11) or no hip pathology (ten). Intra- and interobserver agreement among specialties regarding the diagnosis of a SCFE were assessed using Cohen's kappa coefficient (κ). Diagnostic accuracy of SCFE relative to the benchmark, a combination of the radiographic diagnosis based on Klein's line, clinical symptoms and surgical treatment, was assessed computing sensitivity, specificity and accuracy.
Results
Intraobserver agreement between the surveys was moderate among paediatricians (κ-range, 0.44 to 0.52), moderate to almost perfect among orthopaedic surgeons (κ-range, 0.79 to 0.88) and almost perfect among paediatric radiologists (κ-range, 0.83 to 1.00). Interobserver agreement for survey 1 and 2 was slight among paediatricians (mean κ, 0.19), substantial among orthopaedic surgeons (mean κ, 0.77) and almost perfect among paediatric radiologists (mean κ, 0.86). Sensitivity of SCFE-diagnosis was high among radiologists and orthopaedic surgeons (88% to 100% for both specialties), but lower for paediatricians (24% to 76%). Specificity was high among radiologists and orthopaedic surgeons (72% to 84%), however, variable among paediatricians (56% to 80%). Accuracy of a SCFE-diagnosis was highest in radiologists (84% to 92%), followed by orthopaedic surgeons (80% to 88%) and paediatricians (48% to 78%).
Conclusion
SCFE can be detected on radiographs by different medical specialties. Intra- and interobserver agreement, specificity, sensitivity and accuracy for radiographic SCFE-diagnosis amongst paediatric radiologists and orthopaedic surgeons are better than that of general paediatricians.
Level of Evidence
II
Introduction
Slipped capital femoral epiphysis (SCFE) is one of the most common hip disorders amongst adolescents ranging from nine to 16 years of age. 1 It is characterized by the displacement of the femoral neck in relation to the femoral head through the epiphyseal plate during rapid growth. 2 The incidence of SCFE in the United States is 10.8 cases per 100 000 children, with a significant higher incidence in boys than girls. 3 The majority of patients diagnosed with SCFE are obese. Less common associated disorders include endocrinopathies such as hypothyroidism, hypogonadal states and renal osteodystrophy. 4 An impact of environmental and genetic factors on the development of SCFE has also been suggested. 3
Despite its high incidence, delay in diagnosis of SCFE frequently occurs due to vague and misleading symptomology. Patients can present with hip, groin, thigh or knee pain that can be mistaken for other conditions such as growing pains, muscle strain and tendonitis.5,6 Other risk factors for delayed diagnosis include insurance type, stable slips (compared with unstable slips), increased slip angle and higher body mass index.5–12 Various studies have reported an incidence between 19.6% and 52% of SCFE cases with missed diagnosis at initial exam.5,7,13,14 A significant relationship between delay in diagnosis of a SCFE and increased slip severity exists. 14 Furthermore, the short- and long-term outcomes are worse with complications such as accelerated degenerative changes, decreased range of movement, osteoarthritis, chondrolysis, avascular necrosis and leg-length discrepancy as the slip progresses.6–9,12–23 Although the adverse effects of a delay in diagnosis have been documented for over ten years,7,8,12 recent reports have not shown a reduction in the time interval from onset of symptoms to diagnosis of a SCFE, with average delays ranging from eight to 33 weeks.6–10,13,24,25
In order to avoid the aforementioned complications, it becomes imperative that all SCFE patients are diagnosed as early as possible and treated accordingly. Clinical exam findings of patients with a SCFE include limited internal rotation of the hip, decreased flexion and abduction, pain with extremes of movement and externally rotated foot progression angle. The diagnosis of a SCFE can be made on anteroposterior (AP) and frog-leg lateral hip radiographs. Klein's Line 26 or its modification 27 are commonly used to identify a slip of the epiphysis on AP radiographs, whereas the head/shaft angle and percent epiphyseal displacement describe the extent of the slip on the lateral radiograph. A delay in diagnosis of a SCFE can be due to one of three reasons: 1) the primary examining physician does not screen the hips using radiographs for adolescents presenting with vague symptoms of SCFE not localized to the hips; 2) only the AP view of the hip is obtained without the frog-leg lateral; and 3) mild SCFE can be missed because of the subtle nature of the radiographic findings.5,6,16,18,28,29 Some studies have pointed out the need for ordering hip radiographs when vague SCFE symptoms are present.28,29 To our knowledge no studies have looked into the capability of providers to accurately assess hip radiographs to diagnose a slipped capital femoral epiphysis.
The purpose of this study was to evaluate sensitivity, specificity and accuracy of a radiographic SCFE-diagnosis among medical specialists.
Materials and methods
Study design
To evaluate intra- and interobserver variability of SCFE diagnosis among different medical specialties, three groups of physicians at tertiary referral centres voluntarily participated in the study: 1) three board-certified paediatricians; 2) three board-certified, fellowship-trained paediatric radiologists; and 3) three board-certified fellowship-trained paediatric orthopaedic surgeons. These medical specialties were chosen because paediatric patients are mostly referred to the orthopaedics department by their paediatrician and radiographs are evaluated by paediatric radiologists at our institution. To evaluate if the level of experience played a role in the diagnosis of a SCFE based on radiographic images, three physicians were recruited in each group, one with 0 to four years of experience, one with five to nine years of experience and one with ten or more years of experience. All nine physicians were asked to review AP and frog-leg lateral hip radiographs of 50 patients distributed via an online survey platform called LibWizard (https://www.springshare.com/libwizard/, Springshare LLC, Miami, Florida). The survey was distributed to each participant twice, one month apart from the first time the physicians took the survey, and the order of the cases was randomized between the first and second survey.
Cases
After obtaining institutional review board approval, records of 95 patients who presented with hip pain or groin pain to a paediatric orthopaedic clinic between 2009 and 2016 were retrospectively reviewed. Patients’ medical charts and radiographs were reviewed for age, gender, diagnosis, chief complaint and other hip pathologies. 50 patients were selected based on diagnosis, availability and good quality AP and frog-leg lateral hip radiographs. Patients were separated into two groups, 25 patients who were diagnosed with a SCFE and 25 patients who were not diagnosed with a SCFE. A diagnosis of a SCFE was based on the radiographic diagnosis using Klein's line, a line drawn along the superior border of the femoral neck, which will not intersect the femoral head in a child with a SCFE, but does in a normal hip, clinical symptoms and surgical treatment with stabilization across the physis by in situ pinning. Patients diagnosed with a SCFE were selected based on the severity of the slips using the Southwick criteria: 30 Grade I < 30°, Grade II 30° to 50° or Grade III > 50°. The vast majority of the selected patients (88%) had either a Grade I or Grade II slip (Table 1), which is similar to the distribution of slip grades found in other studies.31,32 Of the 25 patients who were not diagnosed with a SCFE, patients had diagnoses of Legg-Calvé-Perthes disease (eleven), femoroacetabular impingement (four) or no hip pathology (ten). Legg-Calvé-Perthes disease, femoroacetabular impingement or no pathology are common diagnoses of paediatric patients presenting with hip/groin pain. In order to include radiographic images of patients without a SCFE, these cases were selected. Characteristics of the cases selected are shown in Table 1.
Radiographic cases
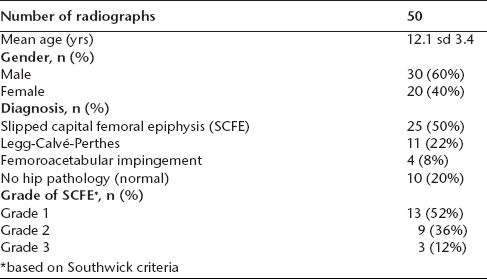
based on Southwick criteria
AP and frog-leg lateral hip radiographs of the affected side for each patient were included in the survey. Age, sex and chief complaint were provided to the survey participants. An example of the user interface is shown in Figure 1.
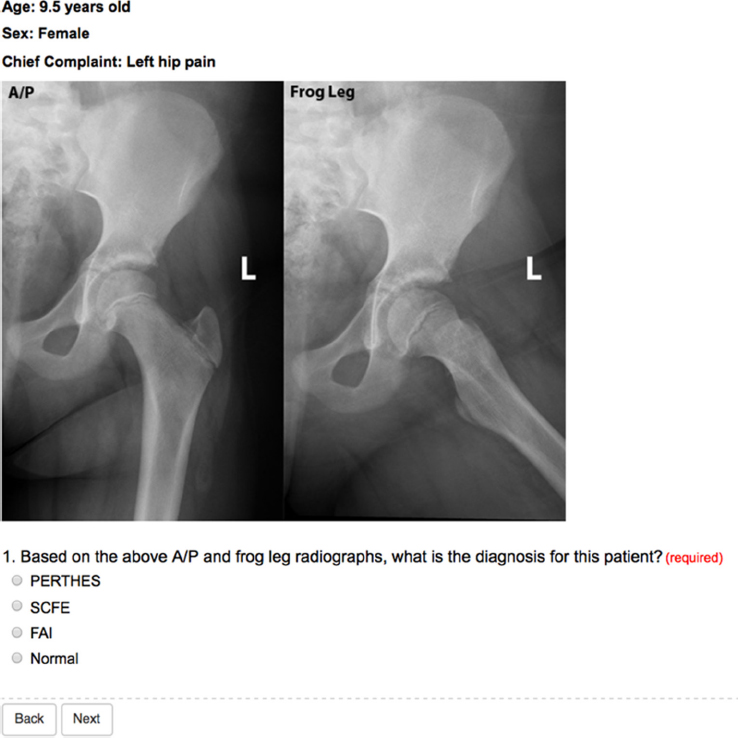
User interface of surveys 1 and 2 showing a representative case scenario provided to participating physicians, as created by the LibWizard programme.
Statistics
Cohen's kappa coefficients (κ) were used to assess interobserver agreement across the three medical specialties (paediatricians, paediatric orthopaedic surgeons and paediatric radiologists) and intraobserver agreement on diagnosing a SCFE. A κ > 0.8 indicated almost perfect agreement, a κ between 0.6 and 0.8 indicated substantial agreement, a κ between 0.4 and 0.6 indicated moderate agreement, a κ between 0.2 and 0.4 indicated fair agreement and a κ between 0 and 0.2 indicated slight agreement (Supplementary Table 1). 33 Accuracy, sensitivity and specificity were computed to assess the diagnostic accuracy of individual paediatricians, paediatric orthopaedic surgeons and paediatric radiologists relative to the benchmark for defining a true positive SCFE. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, North Carolina).
Results
Participants
Nine physicians, three paediatric outpatient physicians, three paediatric radiologists and three paediatric orthopaedic surgeons participated in the study. All physicians were board-certified, paediatric orthopaedic surgeons and paediatric radiologists were also fellowship-trained. All physicians completed surveys 1 and 2, one month apart.
Intraobserver reliability for SCFE diagnosis
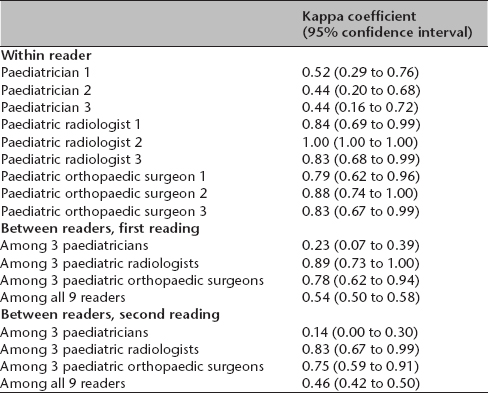
The intraobserver agreement was almost perfect for all three paediatric radiologists (κ range 0.83 to 1.00) and the two paediatric orthopaedic surgeons with more than five years of experience (κ range 0.83 to 0.88). Similarly, the intraobserver agreement was substantial for the paediatric orthopaedic surgeon with experience of 0 to 5 years post-fellowship (κ = 0.79). In contrast, the intraobserver agreement was moderate for the paediatricians (κ range 0.44 to 0.52). Table 2 shows the intraobserver (within reader) κ coefficients and confidence intervals (CI) for all observers.
Intra- and interobserver reliability
Interobserver reliability for SCFE diagnosis
In the first survey, the interobserver agreement was fair amongst the paediatricians (κ = 0.23, 95% CI 0.07 to 0.39), substantial amongst the paediatric orthopaedic surgeons (κ = 0.78, 95% CI 0.62 to 0.94) and almost perfect amongst the paediatric radiologists (κ = 0.89, 95% CI 0.73 to 1.00). Among all nine readers, the interobserver agreement was moderate (κ = 0.54, 95% CI 0.50 to 0.58).
In the second survey, the interobserver agreement was slight amongst the paediatricians (κ = 0.14, 95% CI 0 to 0.30), substantial amongst the paediatric orthopaedic surgeons (κ = 0.75, 95% CI 0.59 to 0.91) and almost perfect amongst the paediatric radiologists (κ = 0.83, 95% CI 0.67 to 0.99). Among all nine observers, the interobserver agreement was moderate (κ = 0.46, 95% CI 0.42 to 0.50).
Overall, there were no substantial changes in interobserver agreement between surveys 1 and 2. Table 2 shows the interobserver kappa coefficients and confidence intervals for both surveys (between readers, first and second reading).
Sensitivity, specificity and accuracy of a SCFE diagnosis
Sensitivity of an accurate SCFE diagnosis, (i.e. the proportion of a SCFE diagnosis correctly identified), was very high among paediatric radiologists (92% to 100%) and paediatric orthopaedic surgeons (88% to 100%) for each survey, but lower for the paediatricians (24% to 76%).
Specificity, the proportion of non-SCFE diagnoses correctly identified, was high among paediatric radiologists (72% to 84%) and paediatric orthopaedic surgeons (72% to 76%), but variable among paediatricians (56% to 80%).
The accuracy of a SCFE diagnosis was highest in the paediatric radiologists (84% to 92%), followed by the paediatric orthopaedic surgeons (80% to 88%) and paediatricians (48% to 78%).
Table 3 provides sensitivity, specificity and accuracy for all observers and surveys. Between survey 1 and 2, sensitivity, specificity and accuracy between paediatricians showed the greatest variations, whereas these parameters remained stable among the paediatric orthopaedic surgeons and paediatric radiologists.
Sensitivity, specificity and accuracy using slipped capital femoral epiphysis (SCFE) as benchmark (SCFE = 1 as event)
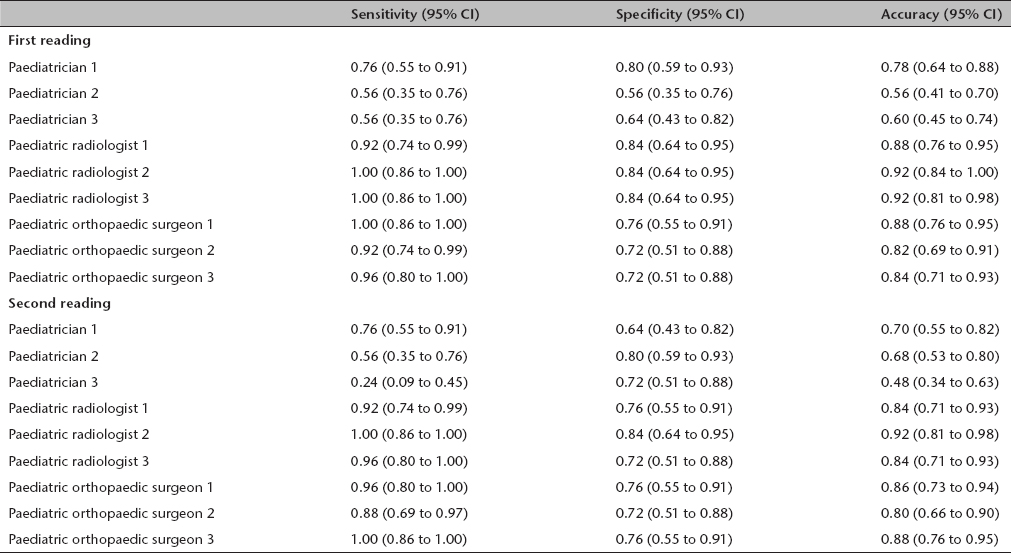
CI, confidence interval
Discussion
Although SCFE is the most common hip disorder in adolescents, 34 its diagnosis is frequently missed due to the subtle, misleading and often delayed symptomology. This has severe implications for slip severity and prognosis. Loder et al 35 demonstrated that patients with a delay of more than two months were 4.1 times more likely to have a moderate or severe slip. Various factors have been reported to explain the cause of longer delays, including knee and distal thigh pain, stable slips and insurance type and coverage.5,6,8,12
Both time from symptom onset to initial physician visit as well as time from initial visit to diagnosis contribute to the delay. Although the time from symptom onset to first physician visit was identified as a major contributor to the delay, this cannot be altered by clinicians. 11 However, healthcare providers can help decrease the time from the first visit to diagnosis. Several studies have reported on the impact that healthcare provider specialty has on delayed diagnosis of a SCFE. Green et al 7 evaluated the primary care system, which included the emergency department, urgent care setting and paediatricians, and found that in 102 patients, the average delay from their first visit with a primary care provider to the time of admission was 10.0 weeks. Hosseinzadeh et al 11 found in their series of 149 patients, that patients presenting to orthopaedic surgeons had a 0.4 week delay in a SCFE diagnosis compared with 13.4 weeks when the patient presented to non-orthopaedic providers. Similarly, Schur et al 10 reported that in their study of 481 patients, the time from first evaluation to diagnosis was significantly shorter for patients evaluated at an orthopaedic clinic (0 weeks) than patients evaluated by a primary care provider (four weeks) or at an emergency department (six weeks). In addition, other studies have identified significantly more diagnostic errors by non-orthopaedic primary physicians.6,7,25 In order to confirm the diagnosis of a SCFE, it has been recommended that both AP and frog-leg lateral views of the hips should be obtained. This is due to the varying nature of the slip. Characteristically, SCFE occurs when the metaphysis migrates anterosuperiorly relative to the physis. 4 In severe cases, this is easily seen in an AP view of a hip. However, in mild cases where minimal displacement occurs, this is not obvious and frog-leg lateral views of the hip become important. An initial presentation of knee or distal thigh pain is also associated with a significant delay of a SCFE diagnosis.8,11 Frequently, only radiographic images of the knees are ordered. Even when the initial examining physician screens the affected hips, reports have showed that only AP radiographs are ordered sometimes.28,29 These published reports have attempted to raise awareness for primary care providers to order the appropriate imaging studies in order to avoid missing the diagnosis of a SCFE.
Even if appropriate hip radiographs are taken when clinically warranted, the subtle nature of the findings can lead the examining physician to miss the diagnosis, even amongst fellowship-trained paediatric radiologists and orthopaedic surgeons as seen in the current study. In order to evaluate sensitivity, specificity and accuracy of SCFE-diagnosis of different medical specialists to diagnose SCFE, online surveys were used to distribute radiographs of SCFE and non-SCFE patients to the participants. Within the past decade, various studies have made use of online surveys such as Zoomerang (http://www.zoomerang.com, San Mateo, California) and SurveyMonkey (SurveyMonkey, Palo Alto, California) to distribute de-identified images to include a larger and more diverse group of physicians nationally and internationally.36–38
In this study, both paediatric radiologists and paediatric orthopaedic surgeons had the highest accuracy in diagnosing a SCFE, however, neither group had 100% accuracy. Individually, both paediatric radiologists and paediatric orthopaedic surgeons had substantial or almost perfect intraobserver agreement. Paediatricians had the lowest sensitivity, specificity and accuracy when diagnosing a SCFE. Furthermore, increasing experience amongst the paediatricians did not seem to make a difference. Rather, the paediatrician with the least experience had the most sensitivity and accuracy in detecting a SCFE and had the highest intraobserver agreement amongst the paediatricians.
There are several limitations to the current study. A SCFE diagnosis for radiographic images shown in the survey was established using the current standard radiographic diagnosis using Klein's line, clinical symptoms and surgical treatment with stabilization across the physis by in situ pinning. A clear control of the SCFE diagnosis by CT, MRI or open operation was not available. The observers in this study had limited clinical information regarding the cases and only the affected hip was presented, thus a comparison to the contralateral side was not possible. Secondly, radiographic findings could not be put into a clinical context, i.e. patient symptoms and physical examination, making the diagnosis potentially more difficult. Thirdly, a limited number of observers were recruited overall and per specialty. In addition, most of the observers were recruited from a single institution. We believe that the results of our study highlight the fact that orthopaedic providers are in the unique position to educate non-orthopaedic providers about the prevalence of SCFE, its risk factors and diagnostic tools available to decrease the delay in diagnosis.
Despite these limitations, some important conclusions can be made from this study. The results indicate that all medical providers are able to diagnose a SCFE from plain radiographs. However, due to the discrepancies found amongst the different specialties, and in order to improve early diagnosis of a SCFE, reduce the long-term complications and its impact on quality of life, increased educational initiatives regarding diagnostic skills for hip conditions should be undertaken in all types of paediatric physician training. Efforts to educate primary care providers should be emphasized and promoted by radiologists and orthopaedic surgeons. Whilst these efforts are carried out, primary care providers who are usually on the front lines of the child and adolescent initial patient evaluation should seek support from radiologists to improve the likelihood of an accurate diagnosis.
Footnotes
Acknowledgements
The authors thank Jamal C. Harris, MD, for his support of this project.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
JMA is a consultant for Axogen, Inc. and receives royalty payments from Springer International Publishing AG. All other authors have nothing to disclose.