
Abstract
Purpose
Previous studies have suggested an association between increased thoracic kyphosis and neural axis abnormalities in patients with adolescent idiopathic scoliosis (AIS). However, the basis for this finding is unclear, and this association has been mainly noted in retrospective studies on a non-consecutive series of patients. The purpose of this study was to assess the relationship between thoracic kyphosis and neural axis abnormalities in patients with AIS.
Methods
We studied a consecutive series of AIS patients treated with spinal fusion. Thoracic kyphosis (T2 to T12) was measured from preoperative lateral radiographs. All patients underwent a spine magnetic resonance imaging (MRI) prior to surgery, and MRI reports were reviewed to determine the presence of neural axis abnormalities. Statistical analyses included descriptive statistics and chi-squared analysis.
Results
This study included 210 patients with AIS. There were no significant differences in age or gender between patients with thoracic hypokyphosis (kyphosis < 20°), normal thoracic kyphosis (kyphosis 20° to 40°) and thoracic hyperkyphosis (kyphosis > 40°) (p > 0.05). Neural axis abnormalities were present in 17.9% of patients with thoracic hypokyphosis, 9.8% of patients with normal thoracic kyphosis and 13.6% of patients with thoracic hyperkyphosis (p = 0.60). There were no significant differences in rates of Chiari malformation, syrinx, intra-spinal masses and other central nervous system abnormalities between groups (p > 0.05).
Conclusions
Thoracic kyphosis was not associated with neural axis abnormalities in our consecutive series of patients with AIS. Increased thoracic kyphosis may not be a reliable indicator for the presence of neural axis abnormalities in patients with AIS.
Level of Evidence
IV
Introduction
Adolescent idiopathic scoliosis (AIS) is a three-dimensional deformity and its aetiology remains unclear. 1 Previous studies have attempted to describe the sagittal plane deformity in AIS1,2 and it has been classically associated with apical lordosis. While normal thoracic kyphosis in adolescents has been noted to be 20° to 40°, 3 several reports have suggested an association between increased thoracic kyphosis and neural axis abnormalities in patients with presumed AIS.4–12 One study suggested a relationship between neural axis abnormalities and thoracic kyphosis > 30°, 9 and another study found a mean thoracic kyphosis of 37° in AIS patients with abnormal MRI findings. 4 However, the basis for these observations is not well understood.
While the majority of patients with AIS are neurologically normal, some patients may have neural axis abnormalities.4,8 Neural axis abnormalities noted on magnetic resonance imaging (MRI) include syringomyelia and Chiari malformation; these abnormalities have been found in 2% to 28% of patients with AIS.4,8–11,13–20 Since these patients may have normal neurological exams, it is imperative to identify predictors of neural axis abnormalities in AIS patients. Identifying neural axis abnormalities preoperatively permits timely management of important conditions, and decreases the risk of complications during spinal deformity surgery. More specifically, it is well-known that neural axis abnormalities increase the likelihood of neuromonitoring difficulties and neurological complications after spinal deformity surgery. 21 In our practice, we commonly refer patients with a neural axis abnormality on MRI to a neurologist or neurosurgeon to assess operative risk and determine the need for neurosurgical management.
Increased thoracic kyphosis has been suggested as a predictor of neural axis abnormalities, however, this association has been noted in smaller retrospective studies or non-consecutive series using varying measures of thoracic kyphosis.4–13 To our knowledge, there have been no studies that have specifically assessed the ability of thoracic kyphosis to predict neural axis abnormalities in patients with AIS. In this study, we aim to assess the relationship between thoracic kyphosis and neural axis abnormalities found on MRI in patients with presumed AIS undergoing surgical correction. We hypothesize that patients with increased thoracic kyphosis will have an increased incidence of neural axis abnormalities on preoperative MRI. If thoracic kyphosis is shown to be predictive of neural axis abnormalities, patients with sagittal plane deformity on routine preoperative radiographs may benefit from advanced imaging and consultation before spinal deformity surgery.
Patients and methods
This study is a retrospective review of a consecutive series of patients with presumed AIS treated with spinal fusion by a fellowship-trained paediatric orthopaedic surgeon (RW). Chart review was conducted to identify these patients, and preoperative clinical, demographic and radiographic data was collected. Given the varying rates of neural axis abnormalities in the literature, all of these patients received a spine MRI prior to surgery in addition to routine preoperative scoliosis radiographs. Patients aged ten to 20 years with a presumed diagnosis of AIS and treated with posterior spinal fusion were included in this study. We excluded patients with other types of scoliosis (congenital, infantile, juvenile and neuromuscular), abnormal neurological exam, known pre-existing neurologic conditions, or missing preoperative radiographs, MRIs and MRI reports. This study was approved by our institutional review board.
Radiographic measurements
We measured thoracic kyphosis (T2 to T12) on the preoperative sagittal (lateral) radiographs using the Cobb method. 22 All measurements were made electronically in a picture archiving and communication system (PACS) by senior orthopaedic surgery residents (Fig. 1). These patients were then divided into three groups based on the degree of kyphosis: thoracic kyphosis < 20° (hypokyphosis), thoracic kyphosis 20° to 40° (normal), thoracic kyphosis > 40° (hyperkyphosis).
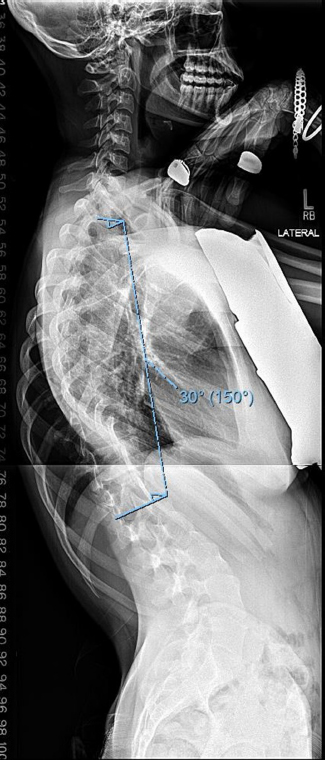
Example of thoracic kyphosis measurement (T2 to T12) on preoperative lateral radiograph.
MRI review
All patients underwent a preoperative MRI of their cervical spine, thoracic spine and lumbar spine prior to surgery. MRI reports were generated by the institution where the MRI was performed, and they were written by an attending radiologist. All MRI reports were reviewed in order to identify neural axis abnormalities, and these abnormalities were coded. The neural axis abnormalities of interest included Chiari malformation, syrinx, intra-spinal masses such as tumors, arachnoid cysts, hydromyelic cysts, and developmental clefts and other central nervous system (CNS) abnormalities such as cerebellar ectopia, cervical stenosis, T2 hyperintensity, gliosis/demyelination and clivus hypoplasia.
Statistical analysis
We divided patients by degree of kyphosis and reviewed their age and gender distributions in order to minimize the risk of confounding. We then determined and compared the rates of neural axis abnormalities for these three kyphosis groups. Descriptive statistics were reported in terms of means and ranges. One-way analysis of variance was used to determine differences in patient age. Chi-squared analysis was used to determine differences in patient gender, as well as to compare the rates of neural axis abnormalities between kyphosis groups. Statistical significance was set to 0.05, and all analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, New York).
Results
In total, a consecutive series of 279 patients with AIS were included in this study. We excluded 18 patients since they did not have MRIs in the PACS or MRI reports, and we excluded an additional 51 patients since they did not have preoperative radiographs in the PACS. As a result, data from 210 patients with AIS were analyzed in this study. All patients had preoperative radiographs and MRI reports, and they all had normal preoperative neurological exams. These patients were all treated with spinal fusion by a single surgeon at an academic medical center between 1996 and 2015. The average age of patients undergoing spinal deformity surgery was 14.7 years (10 to 20), 144 patients were female (69%) and 66 patients were male (31%). The average thoracic kyphosis in this group was 32.3º (2º to 81.4º). Thoracic kyphosis measured < 20° (hypokyphosis) in 39 patients, 20° to 40° (normal) in ١١٢ patients and > 40° (hyperkyphosis) in 59 patients. There were no significant differences in age and gender between all three kyphosis groups (p = 0.89 for age, p = 0.64 for gender) (Table 1).
Kyphosis groups including age and gender data

One-way analysis of variance was used to determine differences in patient age. Chi-squared analysis was used to determine differences in patient gender.
MRI abnormality rates were obtained and compared for all three kyphosis groups (Table 2). In the hypokyphosis group, three patients had a syrinx (7.7%), one patient had an intra-spinal mass (2.6%) and three patients had other CNS abnormalities (7.7%). In this group, four patients required a consultation with a neurologist for their neural axis abnormality prior to spinal deformity surgery (10.3%). In the normal kyphosis group, one patient had a Chiari malformation (0.9%), four patients had a syrinx (3.6%), two patients had an intra-spinal mass (1.8%) and four patients had other CNS abnormalities (3.6%). In this group, four patients required a preoperative neurology consultation (3.6%), and one patient required neurosurgical intervention for a large syrinx noted on MRI prior to spinal deformity surgery (Fig. 2). In the hyperkyphosis group, three patients had a syrinx (5.1%), one patient had an intra-spinal mass (1.7%) and four patients had other CNS abnormalities (6.8%). In this group, two patients required a preoperative consultation with a neurologist for their neural axis abnormality (3.4%).
Rates of neural axis abnormalities on magnetic resonance imaging

Chi-squared analysis was used to compare the rates of neural axis abnormalities between kyphosis groups.
includes cerebellar ectopia, cervical stenosis, T2 hyperintensity, gliosis/demyelination, clivus hypoplasia
sum of all neural axis abnormalities
CNS, central nervous system
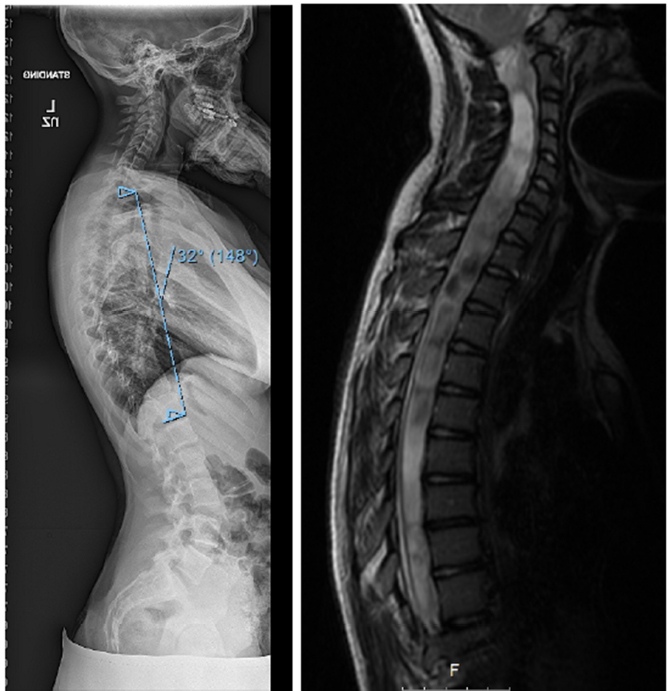
Example of patient with normal thoracic kyphosis and a large syrinx on magnetic resonance imaging.
In total, seven patients with thoracic hypokyphosis had a neural axis abnormality (17.9%), 11 patients with normal thoracic kyphosis had a neural axis abnormality (9.8%) and eight patients with thoracic hyperkyphosis had a neural axis abnormality (13.6%). There were no significant differences in rates of Chiari malformation, syrinx, intra-spinal masses and other CNS abnormalities between groups (p > 0.05). There was also no significant difference in the rates of combined neural axis abnormalities between groups (p = 0.60), as well as no significant difference in rates of patients requiring additional evaluation or management for their neural axis abnormality (p = 0.28). The average thoracic kyphosis in the patients with neural axis abnormalities was 32.6° (5.7° to 64.4°).
Discussion
The relationship between scoliosis and neural axis abnormalities is well known 8 and preoperative MRI has been typically recommended in cases of pain, neurological findings and atypical curve patterns, such as thoracic hyperkyphosis, left thoracic curves, rapid progression or short segment curves.8,9 In this study, we did not find a relationship between thoracic hyperkyphosis and neural axis abnormalities. However, our combined neural axis abnormality rates of 9.8% to 17.9% are within the range reported by previous studies.4,8–11,13–20 While there was a higher rate of neural axis abnormalities and abnormalities requiring additional evaluation or management in patients with thoracic kyphosis < 20º, these findings were not statistically significant. Our results suggest that thoracic kyphosis may not be a reliable indicator for the presence or absence of neural axis abnormalities in patients with AIS, and it should not be used as an absolute indication for preoperative MRI assessment.
Several recent studies have suggested a relationship between loss of thoracic apical lordosis or thoracic hyperkyphosis and neural axis abnormalities;4–13 however, the basis for these observations is not well understood. For example, Richards et al 4 reviewed data from the Spinal Deformity Study Group and found greater thoracic kyphosis (T2 to T12) in AIS patients with right thoracic curves and abnormal MRI findings. In addition, Qiao et al 9 reported that patients with neural axis abnormalities more frequently had thoracic kyphosis ≥ 30º (T5 to T12). In our study, patients with neural axis abnormalities had an average thoracic kyphosis of 32.6°, which is lower than previous reports.4,9 Similarly, Inoue et al 11 found thoracic hyperkyphosis (T5 to T12) to be predictive of neural axis abnormalities on MRI, but they also found strong associations with age at first visit, gender, curve pattern, presence of neurologic deficit and moderate or severe pain. They did not pursue a multivariate analysis of their variables. In contrast, our study controls for age and gender, and we excluded patients with neurologic deficits.
Previous studies have generally been limited to case reports, retrospective reviews and non-consecutive case series, used varying measures of thoracic kyphosis and focused on patients with specific neural axis abnormalities. More specifically, the majority of previous studies report results from a non-consecutive series of patients,4,8,9,13 which subjects their findings to selection bias and confounding. In addition, other studies have been limited to smaller sample sizes, 10 and use a variety of subjective and objective methods to measure thoracic kyphosis, 5 which limits their reproducibility. Furthermore, some studies focus specifically on radiographic abnormalities in patients with syringomyelia or Chiari malformation,5–7,12 which helps to generate hypotheses and guide future research but limits the application of their findings to other patients with scoliosis.
As a whole, the majority of previous studies do not provide prognostic data and evidence that can be applied directly to the clinical practice. In this study, we have attempted to systematically analyze a consecutive series of patients with preoperative radiographs and MRIs in order to validate these previous studies. Based on our findings, thoracic hyperkyphosis is not associated with neural axis abnormalities in patients with AIS, and contrary to recent trends, it should not be an absolute indication for preoperative MRI evaluation. 13 There may be several reasons for our findings including our study design, measurement of thoracic kyphosis and assessment of MRI abnormalities. More specifically, we divided our patients into three groups based on population normal values for thoracic kyphosis 3 and reported values of kyphosis in patients with neural axis abnormalities.4,9 In addition, we measured global thoracic kyphosis from T2 to T12. Alternatively, if we divided our patients into different groups or measured other radiographic parameters, our results may be different. Moreover, a more reliable and exact measurement of apical lordosis may offer additional insights into this relationship. However, our goal in this study was to provide a prognostic framework using established ranges and commonly measured radiographic parameters. Furthermore, our findings are consistent with Gupta et al 16 who reported an equal distribution of hyperkyphosis in a consecutive series of patients with and without intraspinal pathology.
Our study has several strengths. For example, this is one of the largest consecutive series of patients with AIS with preoperative radiographic and MRI data, which minimizes the risk for selection bias and improves our ability to generalize our findings to other populations. Secondly, there were no significant differences in age and gender between our kyphosis groups, which minimizes the risk of confounding. Thirdly, we have assessed radiographic values that can be readily measured. However, it is possible that we underestimated thoracic kyphosis which is commonly misrepresented on 2D radiographs, 1 and we may be inaccurately assessing apical lordosis with our radiographic measures. Lastly, we have included a comprehensive list of neural axis abnormalities, which builds upon the previous studies focusing on syringomyelia and Chiari malformation.5–7,12
This study has several limitations as well. For instance, we did not assess for other differences within groups including curve magnitude, progression and classification, and we did not study other radiographic parameters, including other measures of apical lordosis and coronal parameters. However, the purpose of our study was to focus solely on thoracic kyphosis as a prognostic indicator for neural axis abnormalities, and previous studies have looked at other predictors of neural axis abnormalities in patients with AIS. 8 Adequately powered and controlled studies are needed to better understand the interplay between risk factors and radiographic parameters, and clearly identify predictors of neural axis abnormalities. In addition, even though we studied a large number of consecutive patients with AIS, we excluded several patients due to missing radiographic or MRI data. A larger sample size would further decrease the risk of selection bias, and it may have resulted in our findings reaching statistical significance. A post hoc power analysis revealed that the combined neural axis incidence rate in the hyperkyphosis group would need to be 18% for the difference to be statistically significant. Additional studies using consecutive series of patients are needed to validate our findings. Lastly, thoracic kyphosis was measured by senior orthopaedic residents and we did not repeat these measurements to assess intra- and inter-observer reliability. However, the manual Cobb method has been shown to be a reliable measure.23–25
In conclusion, our study did not find a relationship between thoracic kyphosis and neural axis abnormalities in patients with AIS undergoing spinal fusion. This suggests that thoracic hyperkyphosis on lateral radiographs is not a reliable indicator or predictor of neural axis abnormalities on MRI. Our findings question the previously reported relationship between thoracic hyperkyphosis and neural axis abnormalities, and they will help to guide future research. Additional prospective studies using multivariate analyses are needed to better understand the predictors of neural axis abnormalities in patients with AIS.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.