
Abstract
Purpose
To determine the prevalence of osteonecrosis (ON) in children following treatment of acute lymphoblastic leukaemia (ALL), characterise these cases and review treatment methods.
Methods
All children diagnosed and treated for ALL between 01 January 2003 and 31 December 2013 at our centre were retrospectively reviewed. Logistic regression was used to investigate risk factors for ON occurrence.
Results
Of 235 children treated for ALL, 48/235 (20.4%) children suffered musculoskeletal symptoms necessitating radiological investigation. A total of 13 (5.5%) had MRI-diagnosed ON, with a median diagnosis time of 12 months (interquartile range 10 to 14) following initiation of chemotherapy.
ON affected 40 joints in 13 children. The most commonly involved joints were hips (14 joints in eight patients) and knees (12 joints in seven patients).
Older age at ALL diagnosis was associated with significantly increased risk of development of ON per year (odds ratio 1.35, 95% confidence interval 1.17 to 1.57, p < 0.001).
Eight children underwent at least one surgical intervention. Joint arthroplasty was undertaken in nine joints of four children at a mean age of 18.3 years. All patients who underwent hip arthroplasty had previously received core decompression, with a mean time of 27.8 months (18 to 33) between treatments.
Conclusions
ON is a significant complication of ALL treatment. Our results suggest risk stratification for development of ON by age, and targeted monitoring of high-risk joints is possible. ON treatment is varied with little evidence base.
Keywords
Introduction
Acute lymphoblastic leukaemia (ALL) is the most common childhood cancer with an estimated 400 new diagnoses per year in the United Kingdom, and over half of these made in children under five years of age. 1 Remarkable progress in the understanding of tumour cell biology and optimisation of ‘risk directed therapy’ has taken cure rates from 20% to in excess of 90% over the last fifty years. 2 Internationally, most treatment protocols include relatively intense upfront therapy (induction, consolidation and one or more intensification block) followed by a prolonged period (two to three years) of lower dose maintenance chemotherapy.
Corticosteroids are a key component of induction, intensification and maintenance chemotherapy, and contribute to the current excellent survival rates. However, this high exposure to glucocorticoids comes at a cost of increased bone toxicity and risk of osteonecrosis (ON).3,4 Evidence from successive clinical trials (UKALL97/01, UKALL2003) demonstrate dexamethasone significantly improved event-free survival compared with prednisolone, 5 particularly in regard to risk of central nervous system disease relapse; leading to prednisolone being phased out of current ALL treatment regimens (UKALL2011). However, dexamethasone has been shown to cause more adverse effects than prednisolone, including ON, fracture and infection 6 in American although not European trials. 7
The pathogenesis of ON is multi-factorial and other important treatment related risk factors include non-glucocorticoid anti-leukaemic drugs, haematopoietic stem cell transplantation, total body irradiation and chronic graft-versus-host disease.8,9 Of the non-iatrogenic risk factors, age at ALL diagnosis between 10 to 20 years of age remains the most consistently identified and strongest risk for development of ON. 10
Improved survival from ALL emphasises the need for greater focus on prevention and management of the longer-term sequelae of ALL treatment; of which ON is one of the most common and devastating. Understanding of the burden of musculoskeletal morbidity following ALL treatment is evolving. A total of 24% of children presenting to a United Kingdom centre between 1997 and 2007 and treated for ALL suffered subsequent fracture or ON. 11
Study justification
The burden of musculoskeletal disease secondary to ALL and treatment of the disease has not been characterised in detail to date. Musculoskeletal pain is a common complaint of children receiving chemotherapy for ALL. However, recognition clinically of significant musculoskeletal symptoms is difficult: firstly, glucocorticoids can mask pain, and secondly, therapy-specific patterns of musculoskeletal morbidity have been difficult to delineate given the varied risk factor-specific ALL treatment regimens.
Treatment options for ON are varied and significant heterogeneity between studies and the lack of consistent findings means that no consensus exists on the management of ON following ALL treatment.12–14
We therefore sought to retrospectively determine the burden of ON in children with ALL who were treated with contemporary United Kingdom chemotherapy protocols, comparing our findings with the most recent United Kingdom published literature.11,15 Furthermore, we also aimed to characterise the history, presentation and treatment of our cases of ON, to provide direction for future targeted investigation.
Patients and methods
All children (0 to 18 years) diagnosed with and treated for ALL at Southampton Children's Hospital between 01 January 2003 and 31 December 2013 were retrospectively identified from our centre's Paediatric Oncology database. This period was selected to allow for reasonable follow-up (until January 2017) after completion of treatment, based upon standard treatment times for ALL in the United Kingdom (approximately three years for boys and two years for girls), together with evidence suggesting ON typically develops at the end of the first year of treatment. 11
Business objects software 6.5 SP4 (SAP, Newton Square, Pennsylvania) was used to identify children with a diagnosis of either ‘avascular necrosis’ or ‘osteonecrosis’ (using these search terms). A second search was conducted using the hospital's electronic clinical software for clinic letters, radiographs, MRI and CT scans of all children with ALL, to verify cases found by business objects software, and identify any additional cases. ON was defined by the development of symptoms and confirmation by MRI.
Patients with ALL admitted to hospital acutely whilst receiving chemotherapy but not routinely under the care of our centre's oncological services were excluded from this study. Patients were excluded if they had any primary oncological diagnosis other than ALL.
Patient age at ALL diagnosis, gender, ALL subtype, ALL treatment regimen, age at diagnosis of ON, onset of ON from time of commencing treatment, anatomical site of ON and treatment received for ON were recorded (Table 1). Where ON occurred at multiple sites, date from start of ALL treatment to first diagnosis of ON was calculated.
Osteonecrosis (ON) case characteristics
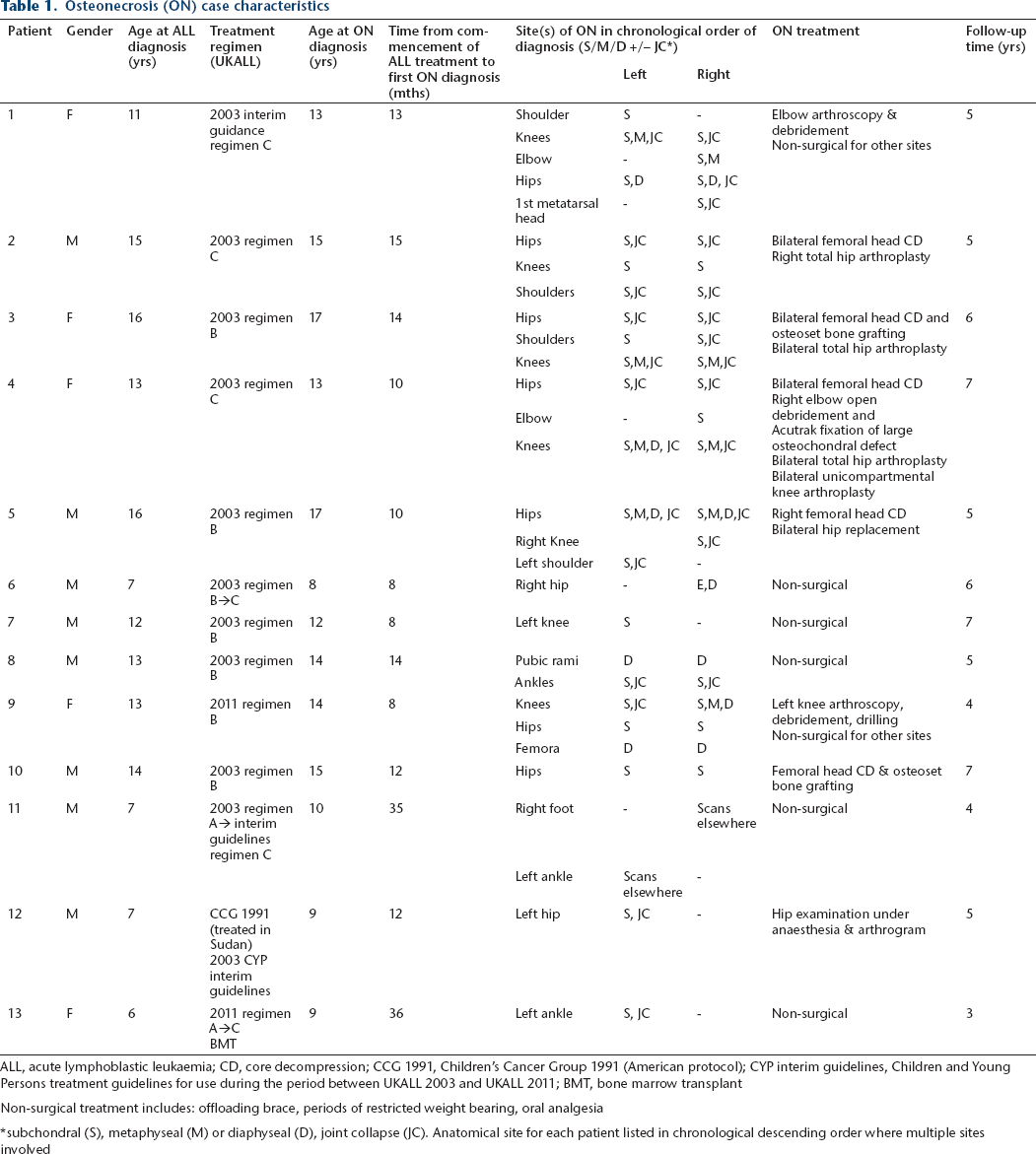
ALL, acute lymphoblastic leukaemia; CD, core decompression; CCG 1991, Children's Cancer Group 1991 (American protocol); CYP interim guidelines, Children and Young Persons treatment guidelines for use during the period between UKALL 2003 and UKALL 2011; BMT, bone marrow transplant
Non-surgical treatment includes: offloading brace, periods of restricted weight bearing, oral analgesia
subchondral (S), metaphyseal (M) or diaphyseal (D), joint collapse (JC). Anatomical site for each patient listed in chronological descending order where multiple sites involved
The MRI scans of all affected hips and knees were evaluated using a novel classification system designed by Niinimäki et al 15 to assess joint involvement at any anatomical site (Fig. 1).
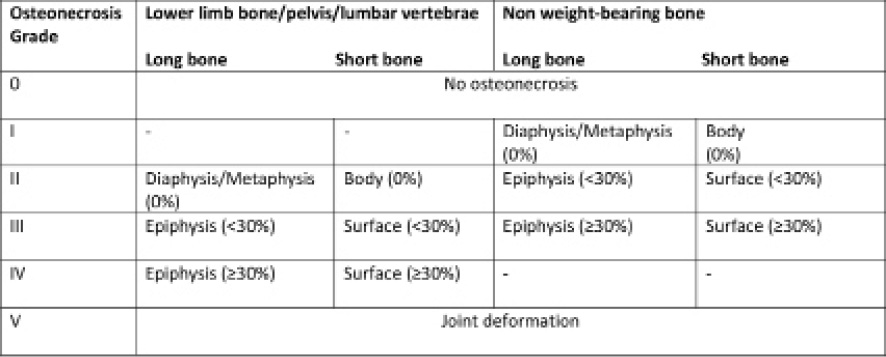
Summary of a new comprehensive radiological classification system for osteonecrosis, applicable to any anatomical site. 15
Statistical analysis
As the recorded data was skewed, results are presented as medians with interquartile ranges (IQR). Statistical analysis was performed using Microsoft Excel 2013 (Microsoft, Redmond, Washington) and IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, New York). Logistic regression models were used to assess association between exposures and ON.
Results
Musculoskeletal disease burden
Between 2003 and 2013, 235 children were diagnosed with and treated for ALL at our hospital. A total of 13 children (5.5%) had MRI confirmed ON (M:F 1.6:1).
Clinic letters showed 20.4% (48/235) children suffered musculoskeletal pain and underwent subsequent radiological investigation. Of these 48 symptomatic children, over a quarter (27.1%) had a diagnosis of ON at a median follow-up time of five years (IQR 5 to 6) from ALL diagnosis.
Age and timing of ON diagnosis
The median age at ALL diagnosis for the whole cohort was four years (IQR 2 to 7.5).
The median age of ALL diagnosis in patients who subsequently developed ON was 13 years (IQR 7 to 14). The median age of ALL diagnosis in patients who did not develop ON was four years (IQR 2 to 7) (odds ratio (OR) 1.35, 95% confidence interval (CI) 1.17 to 1.57, p < 0.001). Children diagnosed with ALL over the age of ten years were at a significantly higher risk of developing ON compared with those diagnosed at less than ten years of age (OR 10.54, 95% CI 3.04 to 36.48, p < 0.001).
The median time from commencement of ALL chemotherapy to first diagnosis of ON was 12 months (IQR 10 to 14).
Gender distribution
Of 235 children treated for ALL, 137 were boys and 98 girls (M:F = 1.4:1). Of the 48 children who suffered musculoskeletal symptoms and underwent radiological investigation, almost twice as many boys (31/48, 64.6%) were affected compared with girls (17/48, 35.4%). Despite this, the prevalence of ON in boys was 6.0% (8/133) and 4.9% (5/102) in girls.
The median age at diagnosis of ON in boys was 12.5 years (IQR 7 to 14.25) and 13 years (IQR 11 to 13) in girls.
Anatomical site of ON
ON at multiple joint levels affected 7/13 children. Two of the 13 children suffered bilateral ON at only one joint level. Four children suffered unilateral, single joint disease.
In total, ON was diagnosed in 40 joints (Fig. 2), and in two children affecting the diaphyseal bone only (one in the pubic rami and the other in the femora). ON most frequently affected the hips (14 joints in eight children) and knees (12 joints in seven children). In cases of multi-level ON (seven children), hips were the first joints to be affected in 5/7 children.
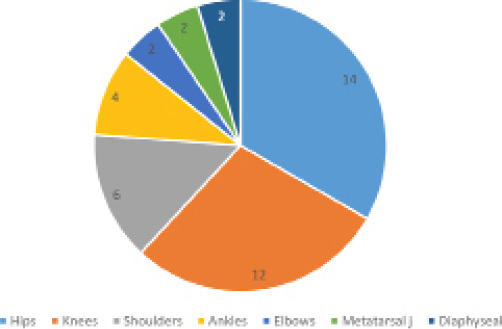
Pie chart representation of anatomical distribution of joints affected by osteonecrosis (number of joints).
ON treatment
Five of the 13 (38.5%) children affected received non-surgical treatment only. Eight children (8/13, 61.5%) underwent at least one surgical intervention (Table 1). Six of these children had evidence of articular surface collapse on pre-operative scans (Fig. 3). Any treatment requiring a general anaesthetic was included as a surgical intervention and these consisted of examination under anaesthesia, arthrogram, arthroscopy and debridement, core decompression, bone grafting and joint arthroplasty.
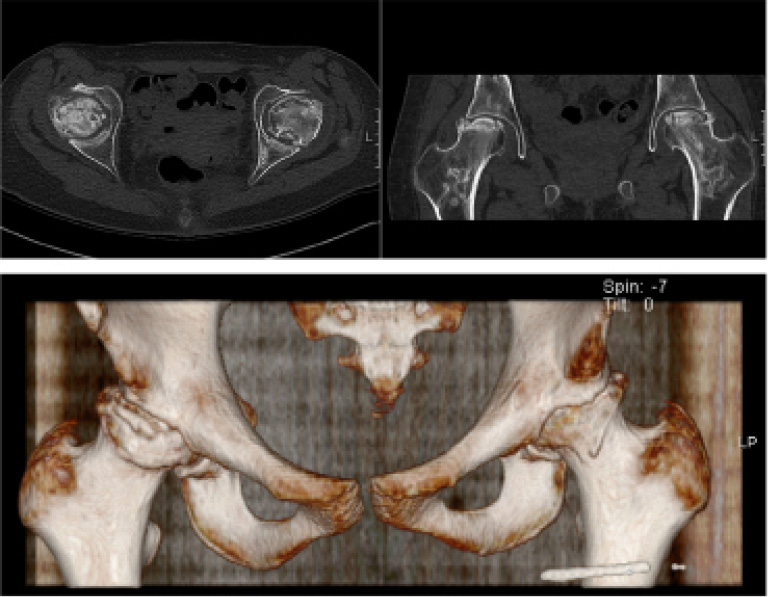
CT axial, coronal and 3D reconstruction images of one 16-year-old patient with bilateral osteonecrosis, taken 32 months following commencement of chemotherapy. Necrosis and associated impaction type fractures to the superolateral femoral heads are present. This is associated with superior joint subluxation. Multiple focal areas of lucency with sclerotic borders are seen within both acetabuli and proximal femoral necks consistent with bone infarction.
At a median follow-up time of five years (IQR 5 to 6), joint arthroplasty had been undertaken in nine joints of four children (seven total hip arthroplasties and two unicompartmental knee arthroplasties) at a mean age of 18.25 years.
Hips
All four patients who underwent hip arthroplasty had previously undergone core decompression, with the decision to proceed to total hip arthroplasty made at a mean of 27.8 months (18 to 33) following core decompression. Core decompression was undertaken in nine hips of five patients at a median of 11 months (IQR 10 to 14) following commencement of chemotherapy.
One patient underwent core decompression (and osteoset bone grafting) with no subsequent surgical intervention. This patient had an intact joint surface at the time of core decompression and at seven-year follow-up (September 2015) was asymptomatic and actively participating in sport. The other four patients who all underwent bilateral core decompression showed evidence of joint collapse, and ultimately total hip arthroplasty was undertaken in seven out of eight joints (Table 2).
Summary of hip and knee osteonecrosis (ON) radiological grading and management of these joints
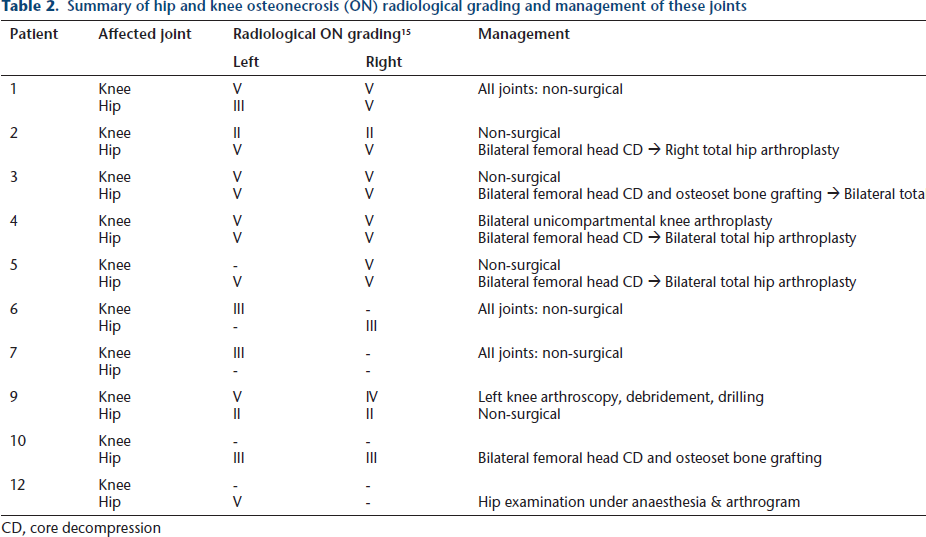
CD, core decompression
Knees
Of the 13 knees in eight patients affected, two patients underwent surgical intervention; one received bilateral unicompartmental knee arthroplasty and the other underwent arthroscopy, debridement and drilling. All three joints showed pre-operative Niinimäki grade V ON changes on MRI (Table 2).
Other sites
ON affecting all other joints and diaphyseal sites was managed non-surgically apart from two elbow debridements; one arthroscopic and one open (Table 1).
Surgical complications
No complications including wound problems and soft-tissue or joint infections occurred in the eight children who underwent surgical intervention. This included multiple procedures undertaken during chemotherapy and steroid treatment phases.
ALL subtype and treatment regimen
All the cases of ON had precursor-B cell or common ALL.
Of the 13 patients with ON, nine completed treatment on the UKALL 2003 regimen (recruitment 01 October 2003 to 20 June 2011), two received 2003 interim guidance regimens (21 June 2011 to 25 April 2012) and two were treated according to UKALL 2011 (recruitment 26 April 2012 to 30 April 2018) guidelines.
In UKALL2003, interim and UKALL2011 treatment regimens dexamethasone is the only steroid used. The 2011 treatment guidelines introduced two randomisation options compared with the 2003 regimens, in part with the aim of reducing toxicity of the steroid component of therapy:
Comparison of a shorter (14-day) course of high dose (10 mg/m
2
) dexamethasone with the standard (28-day) lower dose (6 mg/m
2
) administered during the induction phase. Comparison of standard maintenance therapy with: high dose systemic methotrexate instead of standard intrathecal methotrexate, maintenance chemotherapy without vincristine and dexamethasone pulses.
Due to a small sample size of 13 patients with ON, subsequently smaller numbers within each treatment arm (A, B or C) and smaller numbers still after UKALL trial randomisation, statistical analysis for associations between different treatment regimens and outcome was not performed.
Discussion
One-fifth of children with ALL (48/235) suffered musculoskeletal symptoms requiring subsequent radiological investigation. This is lower than previous United Kingdom data showing almost half of ALL patients in one cohort necessitating investigation (88/186, 47%). 11 This may be associated with changes to ALL treatment protocols since these most recent publications (UKALL97, UKALL97/01 and UKALL2003 in the 2010 study 11 versus UKALL2003, interim and UKALL2011 in this study). However, the newer protocols included in this study solely use dexamethasone which has been associated with a higher incidence of musculoskeletal morbidity than prednisolone; suggesting other factors such as different thresholds for investigation, non-steroidal chemotherapy drugs and population-based factors need to be considered. More importantly, the focus of this study was the prevalence of symptomatic ON, which was higher in this study: 27.1% (13/48) symptomatic patients versus 20.5% (18/88) symptomatic patients in the 2010 study. 11 Our crude prevalence rate of 5.5% (13/235) is consistent with a larger 2008 study 16 reporting a rate of 4.0% (42/1053).
In keeping with previous findings that age at ALL diagnosis of nine or ten years is a significant threshold in risk of developing ON,3,7,11,17 we found age over ten years to be associated with a significantly increased risk of ON (OR 10.54, 95% CI 3.04 to 36.48, p < 0.001). Our third consistent finding was onset of ON; 11 diagnosed typically at the end of the first year of chemotherapy.
We speculate that corticosteroids and chemotherapeutic drugs play a key role in the pathogenesis of ON in children who are most susceptible during typical ‘growth spurt’ age − due to mismatch in epiphyseal blood supply and demand and/or direct damage to bone microarchitecture. Corticosteroids disrupt normal bone biology both indirectly via the hypothalamic-pituitary-adrenal axis and directly through both deranged osteoblastogensis and bone resorption, however, the interplay between corticosteroids, bone turnover and susceptibility to ALL and ON remains poorly understood and intriguing. This is the first orthopaedic study, to our knowledge, studying ON in ALL patients treated according to UKALL2003 and subsequent trial protocols, detailing anatomical distribution and surgical management.
Approximately half (7/13) of children affected by symptomatic ON suffered multi-level disease, with less than a third (4/13) affected at a single joint. Only one of the four children who underwent arthroplasty had single joint arthroplasty (the other three children had two or more joints replaced). This suggests detection of disease in its advanced stages and/or observation of aggressive disease phenotypes affecting multiple joints.
Core decompression of the femoral head carries the longest and largest experience as a technique to prevent progression to joint collapse. Of our five patients who underwent core decompression (two with osteoset grafting), four proceeded to total hip arthroplasty (bilateral in three patients). Small numbers and variation in practice with or without bone grafting preclude meaningful interpretation of these findings. However, as seen in core decompression for idiopathic avascular necrosis where most benefit is gained from intervention prior to joint collapse, 18 these results suggest that once joint collapse is present, core decompression was not protective of progressive collapse. As summarised in the most recent review of core decompression techniques, larger prospective, randomised studies are needed to elucidate the role of core decompression in joint preservation surgery. 19
Study limitations
All children in this study received dexamethasone as steroid treatment, somewhat unifying drug exposure compared with previous studies looking at older protocols that randomised children to receive prednisolone or dexamethasone. There do however remain differences between the doses and durations of dexamethasone treatments between UKALL2003, interim and UKALL2011 protocols, which would need to be controlled for in a larger study to test for association and to better understand the relationship between dexamethasone and ON.
The selected study period of 2003 to 2013 allowed for a maximum of 13 years follow up by the time of writing. Outcome of these patients after transition to adult orthopaedic services is therefore limited and longer follow-up studies are required.
The retrospective design of this study limits accuracy of timings to dates supplied by clinic letters and radiological investigations. Both the retrospective study design and limited follow up into adult services may contribute to underestimation of the true prevalence of ON in this population.
Clinical impact and study recommendations
Identification of the 5.5% children affected by symptomatic ON prior to articular collapse may allow earlier initiation of joint preserving strategies, with potential to delay or prevent childhood arthroplasty surgery.
Suggestions for attainable changes in practice include standardised joint examination protocols and fast-track pathways from oncology to orthopaedics for ALL patients with musculoskeletal symptoms.
These results strongly suggest that risk stratification for ON by age at commencement of chemotherapy is feasible and may justify greater surveillance in those deemed higher risk. Our results strongly support a role for routine focused examination of larger weight-bearing joints (specifically the hips, knees, shoulders and ankles) at outpatient appointments throughout and following treatment, specifically approaching the end of the first year of chemotherapy for ALL.
The British Osteonecrosis Study is a prospective multi-centre study currently underway to examine the natural history of ON in ALL. 20 Similar long-term follow-up studies are required to compare and fully correlate between treatment methods, to inform a treatment consensus. Tsukanaka et al 21 from Sweden last year produced the largest study to date on modern total hip arthroplasty in patients under the age of 20 years. Follow up of ALL patients into young adult hip clinics and beyond in the United Kingdom will be integral to accurately informing orthopaedic surgeons and their patients; aiding decision making, anticipation of revision surgery and management of expectations.
ON represents a significant and devastating but potentially preventable outcome following treatment for ALL. No benchmark treatment for childhood ON currently exists. Clinical trials to investigate the feasibility of age-based risk stratification for ON at the time of ALL diagnosis and further study of the natural history of ON in the context of ALL and its treatment, especially around puberty, is warranted.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.