
Abstract
Purpose
To report indications, outcomes and complications of instrumented cervical spinal fusion in a consecutive series of children at major university hospitals.
Methods
A retrospective, single surgeon series identified 35 consecutive children with a mean follow-up (FU) of 2.5 years undergoing instrumented cervical spinal fusion between 2005 and 2015.
Results
The main indications were skeletal dysplasia and trauma associated cervical instability. Surgical complications were observed in 12 (34%) patients with multiple complications in four (11%). Four (11%) children required at least one revision surgery, three for nonunion and one for graft dislodgement. All were fused at FU. Surgical complications were more common in children undergoing occipitocervical (OC) fusion than in those avoiding fusion of the OC junction (60% versus 24%) (p = 0.043). Complications were found significantly more in children operated on under the age of ten years than above (50% versus 18%) (p = 0.004). The risk of complications was not dependent on the indications for surgery (skeletal dysplasia versus trauma) (p = 0.177),
Conclusion
Skeletal dysplasia associated cervical instability and cervical spine injuries represented the most common indications for instrumented cervical spinal fusion in children. Complications were observed in one-third of these children and 11% required revision surgery for complications. OC spinal fusion and spinal fusion before the age of ten years are associated with higher risk of surgical complications and increased mortality than non-OC fusions and cervical spinal fusions at an older age. We urge surgeons to employ caution to the patient, timing and procedure selection when treating paediatric cervical spine.
Introduction
Cervical instability needing surgical stabilisation is a rare procedure during childhood. Typical conditions associated with cervical instability include cervical spine trauma, and various metabolic bone diseases affecting the quantity and quality of bone such as skeletal dysplasias. There are relatively few adequate follow-up (FU) studies on the indications, need and surgical outcomes of instrumented spinal fusion in children.1–10 Even less is published on instrumented cervical spinal fusion before the age of ten years.4,11,12 Many studies have included both pediatric and adult populations, with upper and lower cervical spine instability, with non-instrumented and instrumented spinal fusion. 13 Common themes are that surgical treatment is complicated by the petite and fragile osseous spinal elements, 14 and there is a low bone formation rate in skeletal dysplasia. 2
In a recent meta-analysis, cervical screw constructs had significantly higher fusion rates with lower complication rates than wiring techniques did in children with a wide range of cervical spine pathologies. 3 Atlantoaxial (C1 to C2) spine fusion with screws is possible even after spinal cord decompression (C1 laminectomy). 15 Therefore, use of rigid cervical instrumentation might be beneficial for children even though it is challenging due to diminutive osseous and ligamentous structures and anatomical variations. 15
Recent advances in occipitocervical (OC) spinal fusion allow rigid fixation over the craniocervical junction with high fusion rates, 16 but the disadvantages of limited neck movement and long-term morbidity are less known.
Our goals were to report indications, outcomes and complications of OC and non-OC instrumentation in children below and above the age of ten years. We hypothesised that avoiding craniocervical junction would increase the spinal fusion rate with lower risk of post-operative complications.
Materials and methods
A retrospective, single surgeon series study was performed in consecutive children operated at two major university hospitals for cervical instability between 2005 and 2015. Instrumented cervical spine fusions represented 6.3% (35/553) of all instrumented paediatric spinal fusions during the study period of the two university hospitals. Using a prospectively collected pediatric spine register 35 children (aged < 18 years) undergoing instrumented cervical spine fusion were identified by the authors (Table 1).
Pre-operative demographic, imaging and functional data
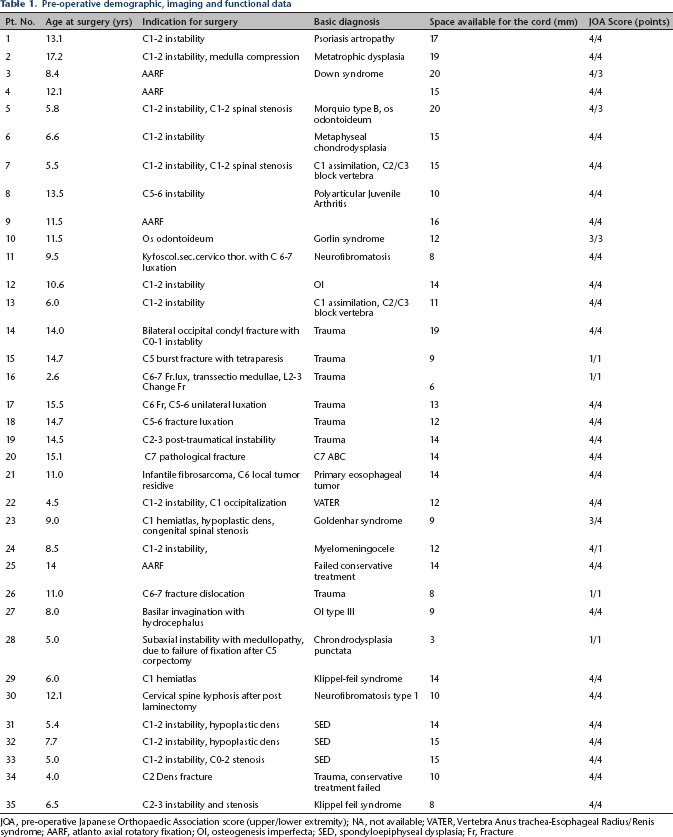
JOA, pre-operative Japanese Orthopaedic Association score (upper/lower extremity); NA, not available; VATER, Vertebra Anus trachea-Esophageal Radius/Renis syndrome; AARF, atlanto axial rotatory fixation; OI, osteogenesis imperfecta; SED, spondyloepiphyseal dysplasia; Fr, Fracture
We collected the following clinical data: clinical presentation leading to diagnosis; presence or absence of neck pain, torticollis or head tilt; and neurologic function pre-operatively, post-operatively and at final FU according to the motor function scoring system of the Japanese Orthopedic Association (JOA). 17
All patients had pre-operative lateral cervical spine radiographs or advanced imaging with CT or MRI. These were evaluated for the presence or absence of: cervical kyphosis; odontoideum or dysmorphic dens; spinal fusion; instrumentation breakage; and junctional kyphosis. In total 31 (89%) patients had pre-operative neutral cervical spine magnetic MRI. From radiographs and imaging, we collected data on: 1) the space available for the cord at tightest interval; and if present for 2) a high signal area in the spinal cord; 3) a spinal cord syrinx; 4) a high-riding vertebral artery; 5) vertebral dysplasia; 6) for dural ectasia.
Evidence of spinal union was assessed from lateral radiographs for continuous bony bridging between the posterior elements at final FU. The indication for spinal fusion was defined as increased atlantoaxial distance ≥ 5 mm 18 or space available for the cord < 13 mm; 19 Basilar invagination was defined as the tip of dens above the level of foramen magnum. 20 Subaxial kyphosis of 60° or more was regarded as an indication for cervical deformity surgery. 4
All procedures performed are described in detail in Table 2. The 28 patients underwent posterior spinal fusion; 26 with rigid internal fixation with pedicle screws, lateral mass screws (LMS) and transarticular screws and two with non-rigid fixation with sublaminar wires and laminar hooks. OC fusion was performed with occiput plate. Spinal cord and nerve root decompression was performed as necessary. Six patients underwent combined approach and one anterior-only approach all with discectomy and plate fixation. Of the six patients who underwent a combined approach, all underwent corpectomy and received anterior structural bone autograft.
Demographic and surgical data at final follow-up
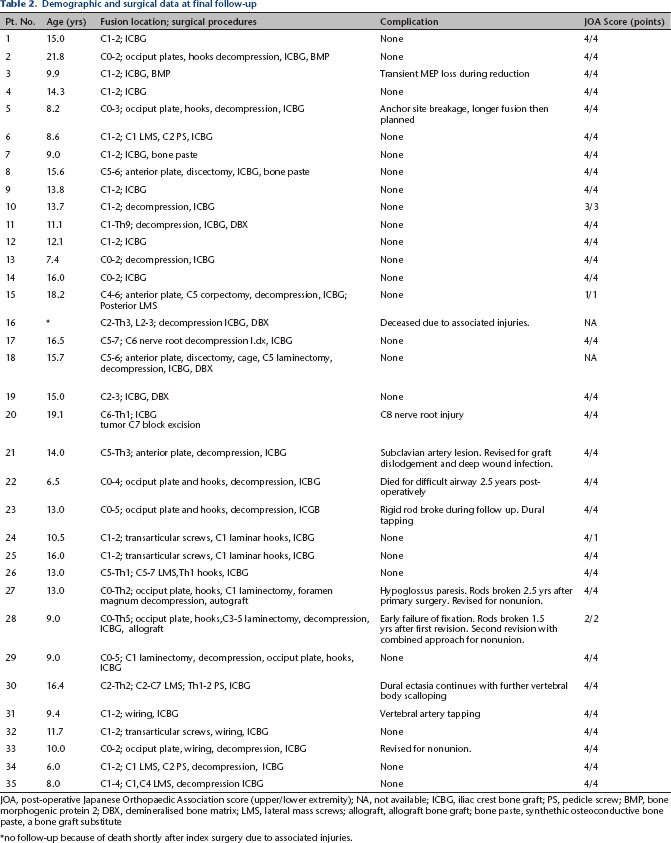
JOA, post-operative Japanese Orthopaedic Association score (upper/lower extremity); NA, not available; ICBG, iliac crest bone graft; PS, pedicle screw; BMP, bone morphogenic protein 2; DBX, demineralised bone matrix; LMS, lateral mass screws; allograft, allograft bone graft; bone paste, synthethic osteoconductive bone paste, a bone graft substitute
no follow-up because of death shortly after index surgery due to associated injuries.
OC fusion was performed in ten patients: four C0 to C2 (one C1 assimilation, one spondyloepiphyseal dysplasia, one metatrophic dysplasia, one post-traumatic instability), one C0 to C3 (instability in Morquio type B), one C0 to C4 (C1 to C2 instability due to VATER syndrome), two C0 to C5 (two C1 hemiatlas in Klippel-Feil syndrome and Goldenhair syndrome), one C0 to Th2 (basilar invagination due to osteogenesis imperfecta type III), one C0 to Th5 (subaxial instability with medullopathy due to early failure of fixation of C5 corpectomy, chodrodysplasia punctate).
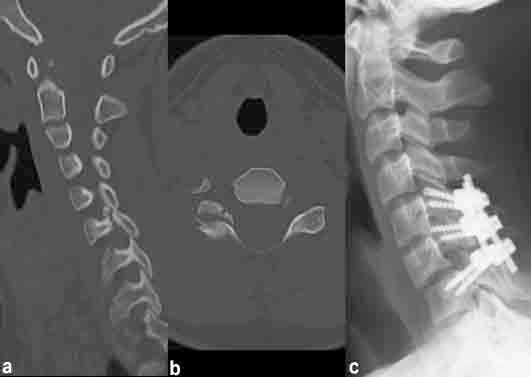
Cervical fusion below the OC junction was performed in 25 children: 13 C1 to C2 (one instability due to psoriasis artropathy, two atlanto axial rotatory fixation, one instability in metaphyseal chondrodysplasia, one C1 assimilation), two C5 to C6 (one instability in polyarticular juvenile arthritis, one post-traumatic instability C5 to C6), one C1 to Th9 (instability in neurofibromatosis), one C4 to C6 (post-traumatic instability after C5 burst fracture), one C2 to Th3 (post-traumatic instability after C6 to C7 fracture luxation), one C5 to C7 (post-traumatic instability after C6 fracture) (patient 17, Fig.1), one C2 to C3 (post-traumatic instability at C2 to C3), one C6 to Th1 (pathological fracture of C7 aneurysmatic bone cyst), one C5 to Th3 (infantile fibrosarcoma in C6), one C5 to Th1 (post-traumatic instability after C6 to C7 fracture), one C2 to Th2 (instability in neurofibromatosis type I), one C1 to C4 (instability in Klippel-Feil syndrome).
(
Intra-operative neurophysiological monitoring was done with motor evoked potentials (MEP), somatosensory evoked potential and electromyography in all patients. All patients received bone grafting during posterior spinal fusion (Table 2). Additionally, four patients received demineralised bone matrix.
Statistical comparisons were performed with a Chi-squared test for categorical parameters and unpaired or paired t tests for continuous variables. P values of 0.05 or below were considered statistically significant.
Ethical committee approval was obtained at both university hospitals. No patients or parents were contacted in the course of the study, and therefore no informed consent was requested by ethical committees.
Results
The main indications and outcomes are gathered on Tables 1 and 2. The main indications for instrumented cervical spinal fusions in children in the current series were skeletal dysplasia associated cervical instability and cervical spine injuries (Fig. 1).
A total of 23 children were operated on for skeletal dysplasia. A total of 21 were primary spinal fusions and two were revisions, with the mean patient age at initial surgery 9.9 years (5.0 to 17.2). The mean estimated blood loss was 297 ml (20 to 1500) and the mean operative time was three hours 27 minutes (1 hour 45 minutes to 10 hours 10 minutes). Four patients underwent pre-operative halo traction to reduce cervical deformity at a mean of 21 days (10 to 69 days) before surgery. In total, 20 patients were post-operatively immobilised with a body jacket for a mean 90 days (60 to 120) and three were immobilised with a rigid collar for a mean 90 days (60 to 120). Mean FU was 2.8 years (1.5 to 4.0). In total, 16 complications were observed in nine (39%) patients, and four (36%) children required at least one revision surgery: three patients for symptomatic non-union and one for graft dislodgment (patients 21, 27, 28, 33, respectively; Table 2). There was only one operation-induced persistent nerve root lesion in the current series (patient 20). A patient with a C7 aneurysmatic bone cyst and a pathological fracture was treated with C7 block excision and fusion. The child suffered a C8 nerve root lesion with permanent sensory deficit on ipsilateral arm without motor deficit. One patient suffered an isolated hypoglossus paresis after OC spinal fusion for basilar invagination, which resolved within two weeks (patient 27).
A total of 12 children were operated on for trauma. All were primary spinal fusions with the mean patient age at initial surgery 9.4 years (2.6 to 15.5). The mean estimated blood loss was 218 ml (100 to 350) and the mean operative time was three hours six minutes (two hours to four hours 15 minutes). One patient underwent pre-operative halo traction to reduce cervical deformity for ten days. Five patients were post-operatively immobilised with body jacket for a mean 105 days (90 to 120) and seven were immobilised with rigid collar for a mean 90 days (60 to 180). Mean FU was 2.1 years (1.0 to 5.0) in surviving patients. Three complications were observed in three (25%) patients (Table 2). One two-year-old child with C6 to C7 level traumatic C1/C2-level spinal cord transection and a L2 to L3 change fracture died two days after the operation for trauma associated hypoxic brain injury (patient 16).
All surviving patients were fused at final FU.
OC spinal fusion carried a higher risk of complication than non-OC fusions (60% (6/10) versus 24% (6/25); p = 0.043). Overall there were 11 complications found in the ten patients who underwent OC fusion compared with the eight in the 25 patients in whom the fusion of the craniocervical junction was avoided (Tables 2 and 3). Three patients had rigid rods broken during FU, all with OC fusion and spanning five or more vertebrae (patients 23, 27, 28). There was only one spinal cord injury due to operative treatment in the current series (patient 28). This patient was operated on primarily outside our facility with C5 corpectomy from the anterior approach with biodegradable plate. Early failure of the fixation resulted in severe spinal cord compression with tetraplegia. He was revised with OC fusion and later needed second revision with combined approach for nonunion. In FU, the neurological deficits had improved (JOA score upper and lower extremity pre-operatively 1 and post-operatively 2).
One child with VATER syndrome died 2.5 years after OC fusion in a minor procedure for congenital anorectal malformation under general anesthesia for difficult airway management (patient 22).
Half (18) of the patients in this series were under the age of ten years at first operation (Table 1). Complications were found significantly more in children initially operated on under the age of ten years than above (50% (9/18) versus 18% (3/17); p = 0.004) (Table 3).
The intra-operative neurophysiological monitoring was unaffected except in one patient who experienced a transient MEP loss during reduction without any new post-operative neurologic deficit (patient 3).
Complications summary
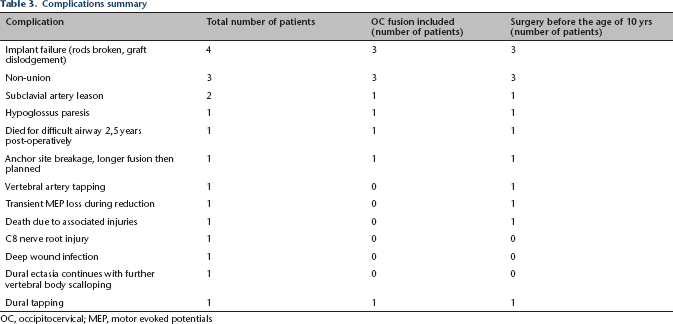
OC, occipitocervical; MEP, motor evoked potentials
The risk of complications was not dependent on the indications for surgery (skeletal dysplasia versus trauma) (p = 0.177) or surgical approach (p = 0.372). The JOA score did not show insignificant improvement during the study. Kyphosis was not associated with higher risk for complications (p = 0.943). Pre-operative halo traction was not associated with a lower risk of complications (p = 0.191).
Discussion
Cervical instability due to trauma or congenital pathologies are the most common indications leading to instrumented spinal fusions in children. The main indications for instrumented cervical spinal fusions in the current series were instability due to skeletal dysplasias and trauma. Fusion is sometimes necessary to treat and/or prevent neurologic deficits from developing. 21 Rigid internal fixation with screw constructs has found favour over previous semi-rigid wiring techniques and has been documented to be superior in terms of lower complication rates5–7 and higher fusion rates.5–7 The biomechanical stability of C1 to C2 fusion has also been found to be in favour of a screw system over wiring techniques in cadaver studies.22,23 It is also thought that rigid internal fixation will diminish the need and duration of long post-operative external stabilisation devices, thus quickening the recovery. However, the long-term consequences of C1 to C2 and OC fusion are less known. Kennedy et al 8 reported that the mean vertical growth over the fused levels in nine C1 to C2 fusion patients represented 30% of the growth of the cervical spine, and in 31 OC fusion patients the majority had substantial growth at the fused levels. Of the series, 85% had good skeletal alignment at FU. Anderson et al 9 reported that the long-term maintenance after C1 to C2 and OC fusion is good.
In Kennedy et al's 9 series there were eight cervical spine fractures or dislocations requiring instrumented spinal fusion with fusion rates of 100%, as was the fusion rate in the current series for trauma patients of whom the information was available without revision operations. The mortality rate was 14% cervical injuries, similar to Eleraky et al 24 who reported a mortality rate of 16% in 102 cervical injuries.
The upper cervical spine (C0 to C4) is more at risk in small children with high energy trauma. 25 Carreon et al 26 reported that the incidence of cord injury is higher in younger children and that they have a higher risk25,26 of death than older children, with even higher complication rates in polytrauma and surgical patients. In this series, the only child who died during the immediate post-operative period was a 2.5-year-old child with polytrauma.
The complication rate in the current series was 34% with multiple complications in 11% (Table 3). This is a little higher than in previously published series (Table 4), with higher risk in OC (60%) than in non-OC (24%) and in children initially operated on under the age of ten (50%) than at an older age (18%). Hwang et al
3
reported, from a literary review and own series, a complication rate of 26% in 914 adolescent instrumented cervical fusion patients, with multiple complications in 5% and a mean age of 8.3 years. Rajasekaran et al
11
published a report on the safety of pedicle screws in 16 children and noted six pedicle screw breaches, most of these (67%) were found in patients under the age of ten years. Helenius et al
4
reported outcomes of spinal fusion in 22 children with neurofibromatosis associated cervical kyphosis. In this series, 31% of the complications were observed in patients under the age of ten years. Couture et al
12
published a series of 22 instrumented OC fusion patients where all complications were found in patients operated on before the age of ten years (mean age at surgery 4.9 years). Gluf and
Previously published works on cervical spine instrumented fusion in children
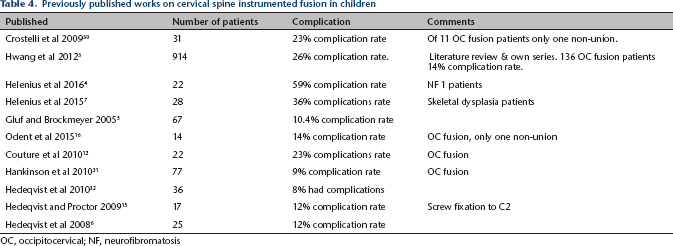
OC, occipitocervical; NF, neurofibromatosis
In previous studies, rigid internal fixation has shown excellent results in providing solid union for C1 to C2 instability in children with skeletal dysplasia.15,16 Hwang et al 3 reported an overall fusion rate of 94.4%; with OC fusion rate with screw fixation 99% and with wiring 95%. With non-OC fusion, the fusion rate was 99% with screws and 83% with wiring. In the current series, the majority of children were operated on with rigid posterior spinal instrumentation, and all surviving patients showed union at final FU (although three children required revision surgery for symptomatic nonunion). These nonunions were associated with OC spinal fusion using rigid fixation.
In Helenius et al's 4 series, all new persistent post-operative neurological deficits were C5 nerve root related. In the current series there was only one, a C8 nerve root injury. Theologis and Burch 27 reported a series of 21 adults operated on for cervical pathologies of one C5 nerve root palsy and two cases of C8 radiculopathies.
Although C1 to C2 transarticular screw fixation is suitable for a large portion of paediatric patients, 28 the vertebral artery injury is a known risk. To diminish the risk of vertebral artery lesion, C1 lateral mass screws (LMS) and C2 pedicle screws (PS) can be used, in addition to careful pre-operative assessment from pre-operative imaging. 7 In the current series, there was one vertebral artery injury with an attempted C2 PS. Gluf and Brockmeyer 5 had two vertebral artery injuries. Yoshihara et al 29 reviewed screw related complications in the subaxial cervical spine, including both an adult and paediatric population, noting a higher risk for vertebral artery damage with pedicle screws than with lateral mass screws. In the current study, subaxial pedicle screws were not used between C3 and C6 where anatomical dimensions between the spinal cord, nerve root and vertebral artery typically make their insertion difficult. 22
In accordance with previous studies, we have noted that rigid fixation enhances fusion rates.5–7 Like Crostelli et al 30 we have found that rigid adult instrumentation can be used to treat pediatric cervical spine instability. Similarly, the anatomical dimension rather than age is the most decisive factor when planning fixation, although sometimes challenging to perform. The youngest child in this series to receive rigid instrumentation was a 2.5-year-old child (patient 16).
Recommendations
We recommend careful pre-operative advanced radiographic evaluation of the anatomical dimensions to describe suitable bone anchor locations, e.g. C2 pedicle and the proximity of the vertebral artery. CT navigation seems to be a useful tool. 11 Careful dissection with bipolar diathermy of bony landmarks during surgery is of paramount importance. This is especially useful in the placement of C1 lateral mass screws and C2 pedicle screws. For C1 we recommend C2 nerve root displacement and transsection if necessary, and direct identification of the C1 lateral mass. Similarly, the medial wall of the C2 pedicle exposure is useful for pedicle screw placement. Use of combined approach enhances bony healing for subaxial deformities. Even rigid fixation should be protected using adequate post-operative immobilisation (often with halo body jacket).
Limitations
Children requiring instrumented cervical spinal fusion are few (Table 4). We were able to examine records for only 35 such patients. Although the indications for surgery were clearly determined, this series represents the work of a single paediatric orthopedic surgeon, apart from the one patient whose primary operation was done elsewhere, and was revised in our hospital. Thus, the generalisability of these findings is limited secondary to individual patient selection and surgeons’ preferences for certain surgical techniques. There were no predetermined indications for a combined anteroposterior approach, which was solely determined by the treating orthopaedic surgeon. The small patient numbers, selection and the single study retrospective design are additional limitations of this report. The length of the FU in some cases, and the variety in the aetiology leading to cervical instability requiring spinal fusion, limits the generality of the results. However, the indications, outcomes and complications are carefully described, and many of these children represented a unique clinical history.
Skeletal dysplasia associated cervical instability and cervical spine injuries represented the most common indications for instrumented cervical spinal fusion in children. Complications were observed in one-third of these children and 11% required revision surgery for complications. OC spinal fusion and spinal fusion before the age of ten years carried a higher risk of surgical complications and mortality than non-OC fusions and cervical spinal fusions at an older age. We urge surgeons to apply caution to patient, timing and procedure selection when treating paediatric cervical spines.
Footnotes
Although none of the authors has received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article, benefits have been or will be received but will be directed solely to a research fund, foundation, educational institution, or other non- profit organization with which one or more of the authors are associated.
Disclosure: Markus Lastikka: no financial relationships. Jasmin Aarnio: no financial relationships. Ilkka Helenius: consultant for Medtronic; grants and research funding received from Medtronic International, Baxter International, outside the submitted work.