
Abstract
Purpose
We aim to retrospectively evaluate patients with non-ossifying fibroma (NOF) of the distal femur by radiographs, CT and MRI, and to provide a theory describing the reasoning for the distal femur NOF's location and aetiology.
Methods
Charts of patients with NOFs between 2003 and 2014 were retrospectively reviewed. Inclusion criteria encompassed a diagnosis of NOF of the distal femur by imaging, and histologically, if available. Radiographs, CT and MRI were used to characterise the relationship of the NOF lesions with the surrounding soft tissues.
Results
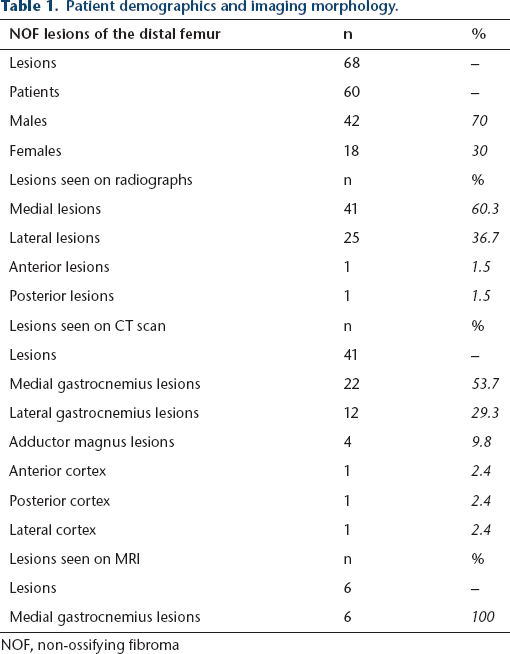
The 68 NOFs from 60 patients were included. By radiograph, 41 (60.3%) of the 68 lesions appeared at the medial and 25 (36.7%) at the lateral aspect of the distal femur. In total, 41 lesions had CT scans, showing 22 NOFs (53.7%) attached to the origin of the medial gastrocnemius, 12 (29.3%) to the origin of the lateral gastrocnemius and four (9.8%) at the attachment of the adductor magnus. Of the CT scans, 93% identified the NOF's relationship with an adjoining tendon of the distal femur. Six had MRIs, all of which showed attachment at the medial gastrocnemius.
Conclusion
The study reveals a relationship between tendinous structures and NOFs. NOFs of the distal femur occur most commonly at the origin of the medial and lateral gastrocnemius. They may originate from the physis/metaphysis but they do not always attach to the physis, as we observe them ‘migrating’ as patients grow. More research is required to understand the exact aetiology of NOFs.
Background
In 1942, the non-ossifying fibroma (NOF) was initially described by Jaffe and Lichtenstein. 1 It was noted to be a ‘benign marrow-connective tissue tumor’ and to have a characteristic eccentric location typically in the bone that adjoined the cortex and was near the physis, typically in long bones. 1 Since the first recognition of the NOF, some characteristics have further been defined:
the NOF lesion is eccentric in location in the metaphysis and will typically have a sclerotic rim and appear multiloculated;
the most common locations are: (1) distal femur, (2) distal lateral tibia and (3) proximal medial tibia;
NOFs occur during childhood and are rarely seen after the age of 20 years;
some lesions will resolve on their own, usually at adolescence;
some lesions will enlarge, and because of size or a cortical breach cause pathologic fractures of the long bones;
smaller lesions may be watched, while enlarging lesions may require surgery2,3 to prevent a fracture.
Despite these gains in knowledge of NOF, its aetiology remains poorly understood. Leading theories include those that suggest that NOFs arise from bone marrow cell lineage or that they arise from the physis itself.1,4,5 In 1986, Ritschl and Karnel 6 showed that areas in long bones where tendons insert into the perichondrium of the epiphyseal plate are the only location that NOFs occur and went on to suggest that the lesions are a result of an ‘unknown pathogenesis’ that causes a disorder of metaphyseal bone growth.2,6 The idea that there is a connection between fibrous metaphyseal defects and tendon insertion has also been described with cortical desmoids of the distal medial femur; these so-called ‘tug lesions’ result from traction at the origin of the of the adductor magnus. 7 Abnormal pull or anchorage of the tendon has also been implicated in focal fibrocartilaginous dysplasia. 8 In this case, anchorage of the lesion into the bone (usually proximal tibia) results in a tethering and bending of the bone. Some might hypothesise that the NOF, a lesion considered to be a divergent lesion of other fibrous cortical defects including cortical desmoids, may begin in a related fashion. 7 Recently, NOFs in the distal tibia were proposed to originate as tug lesions from the interosseous membrane. 9 It is possible that the lesions in the distal femur originate similarly.
While the ‘tug lesion’ theory seems plausible at the distal femur (the most common location of NOFs), there has not been a large-scale study dedicated to proving or disproving it as a cause of NOF aetiology in the literature. In this study, we aim to evaluate retrospectively a large group of patients with NOFs solely of the distal femur by radiographs, CT and MRI. We plan to use these data to provide a theory describing the reasoning for the distal femur NOF's location and aetiology.
Materials and methods
Institutional review board approval was obtained for this study. Charts from Rady Children's Hospital in San Diego, California were obtained between January 2003 and March 2014 and retrospectively reviewed. Charts provided had ICD-10 codes consistent with NOF (M84 to M85.9) 10 and/or CPT codes consistent with curettage/grafting of bone lesion (27355, 27356, 27357). 11 These charts were reviewed in depth for those patients specifically with a diagnosis of distal femur NOF (as determined by radiographic findings and confirmed with histological findings if available). Patients who did not have at least one form of imaging were excluded from the study. Study patients were analysed for presence or absence of pathologic fracture, location of the lesion, as well as demographical data. Radiographs from the time of diagnosis were reviewed. CT and MRI scans previously obtained for further evaluation were reviewed as well to further characterise the relationship of the NOF lesions with the surrounding soft tissues.
Results
A total of 68 NOFs from 60 patients were included in the study because of complete patient data and radiographs. Patient demographics showed a male predominance of 2.33:1. Age at first diagnostic radiograph was in the range of four to 19 years, with an average and median age of 12 years. Of these 60 patients, ten (17%) were diagnosed with NOFs by pathologic fracture, 11 (18%) were diagnosed due to pain and 37 (62%) were diagnosed incidentally, leaving two patients in whom chart review did not reveal a cause for initial presentation.
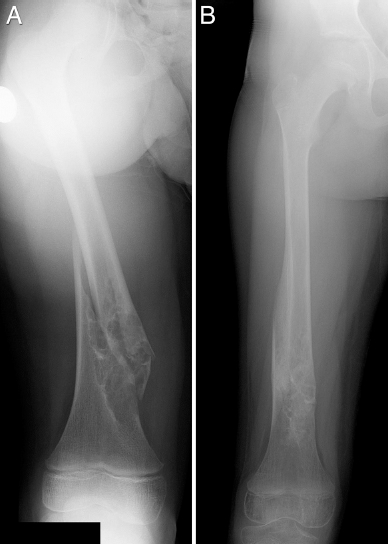
Two-thirds of the 68 lesions appeared at the medial aspect of the distal femur. One-third of the lesions were at the lateral aspect of the distal femur. Only one lesion appeared directly anterior and one lesion appeared directly posterior in the distal femur (Fig. 1).

Radiographs with non-ossifying fibromas (NOFs) at different locations: (
Of the 68 lesions that were identified on radiographs, 41 had CT scans and six had MRI available for review. This advanced imaging was used to determine the relationship of the NOF to the surrounding tendons. Of the CT scans, 93% identified the NOF's relationship with an adjoining tendon of the distal femur. The CT scans showed over half of the NOFs (54%) attached to the origin of the medial gastrocnemius, about one-third to the origin of the lateral gastrocnemius (29%), and about 10% at the attachment of the adductor magnus (Figs 2 to 4). Only three CT scans showed NOF lesions that were not seemingly connected to a tendinous structure (Fig. 5). Of the six MRI scans, all showed attachment at the medial gastrocnemius to the cortical defect of the medial distal femur (Fig. 6). Table 1 provides a summary of the aforementioned data.
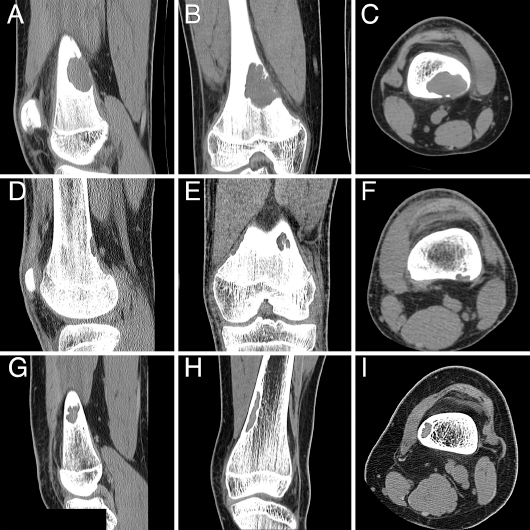
CT scans demonstrating tendinous involvement with the non-ossifying fibromas (NOFs): (
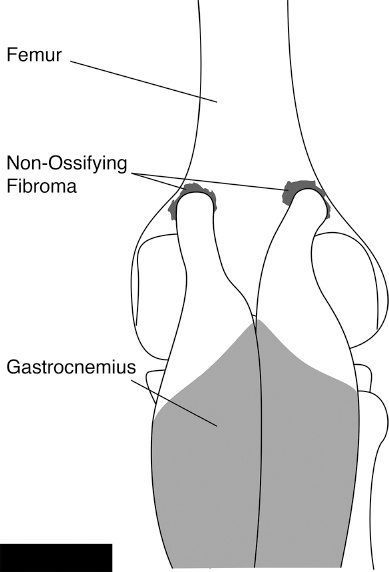
A drawing demonstrating the aetiology of the tug lesions at the origin of the medial and lateral gastrocnemius.
One patient with both lateral and medial non-ossifying fibromas (NOFs) of the distal femur: (

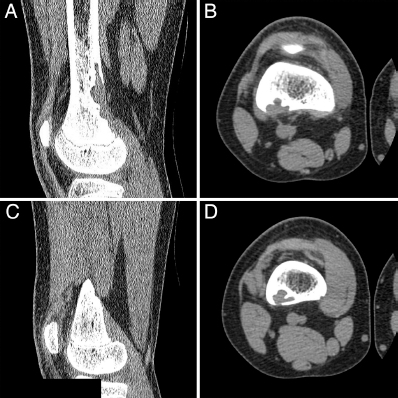
CT scans of the only three patients with non-ossifying fibromas (NOFs) that did not show connection to a specific tendinous structure: (

Non-ossifying fibroma with connection to the head of the medial gastrocnemius demonstrated on MRI (
Patient demographics and imaging morphology.
NOF, non-ossifying fibroma
Discussion
What is the aetiology?
While the classic description of the NOF is an eccentric lesion at the cortex near the physis in long bones, the aetiology behind these lesions remains poorly understood.1,4,5 The most common location of NOFs is the distal femur, which is the reasoning behind the focus of this study. This is possibly due to the anatomy of the distal femur, as the posterior cortex is thin with a concave shape of the posterior condyles. There are several vascular passages in this area that may provide for further weakening. 12 Recently, Muzykewicz et al 9 from our institution published a study on the aetiology of distal lateral tibia NOFs in a large number of children (n = 47). They found communication of the distal interosseous membrane in 97% of these lesions on CT scan and 100% on the lesions by MRI. This suggested that these lesions may arise as a tug from the interosseous membrane. Several papers have suggested that distal femur NOFs typically arise as ‘tug lesions’ at the origin of the medial head of the gastrocnemius, similar to cortical desmoids arising at the insertion of the adductor magnus.7,8,12 NOFs at the origin of the lateral gastrocnemius have been mentioned in the literature, but only rarely. It has been suggested that the origin more frequently occurs at the medial gastrocnemius due to its insertion being broader and thicker with a more transverse shape than the lateral gastrocnemius.7,8,12
The present study shows the distal femoral lesions to have an eccentric location in three distinct locations. Just over half (53.7 %) arise at the head of the medial gastrocnemius and nearly one-third (29.3%) arise at the head of the lateral gastrocnemius. Nearly 10% of the lesions occurred at the origin of the adductor magnus. As remodelling occurs with growth, we see the lesions travel proximally towards the diaphysis away from the physis and the tendinous origin (Fig. 7). Our data imply that NOFs occurring at the origin of the lateral gastrocnemius are more common than previously thought. There were three NOF lesions, or about 7% of the 41 lesions that had CT scans, in this study that did not appear to connect to any fibrous structure on CT scan. The one lateral lesion could potentially be connected to the vastus lateralis, but there are no structures to hypothesise the location of the anterior and posterior lesions. The pathology reports of all three of these lesions that did not have an apparent fibrous connection confirmed the diagnoses of NOF, suggesting further causation to their aetiology.
(
Ritschl and Karnel 6 made the claim in 1986 that NOF lesions are only found in long bones where tendons insert into the perichondrium of the epiphyseal plate. 2 Our findings do not necessarily support this notion. First, while these lesions do originate from the physis/metaphysis, they do not attach to the physis, as we observed them migrating along the diaphysis of long bones as the patients grew. Secondly, three of these lesions did not originate from a tendinous or fibrous location, suggesting that there is further cause for the origin of these lesions. The anterior NOF was in a child who also had a NOF at the ipsilateral lateral gastrocnemius. Perhaps this child was particularly prone to forming NOFs, making him more likely to form one without the ‘tugging’.
Histologically, NOFs consist of benign fibroblastic cells that are arranged in fascicles and whorls with benign multinucleated giant cells and lipophages throughout the lesion with a hemosiderin pigment.13,14 While this histologic pattern is well reported, it does not necessarily provide aetiologic clues. If we propose that these lesions are, in fact, ‘tug lesions’, it is reasonable to also consider the histology of the tendons themselves. Increased fibroblast production in tendons has been reported to increase the production of matrix metalloproteinases (MMP) -2 and -9 at the site of attachment to a type-I collagen matrix (similar to bone). In turn, these MMPs are expected to participate in a catalytic process on the matrix. 15 Further research is needed to determine if a similar mechanism is occurring in the tendons at the site of NOF tug lesions.
There is a significant terminology debate for lesions of the distal femur. Are NOF, fibrous cortical defects and cortical desmoids one and the same? Typically, cortical desmoids are considered to be within the cortex and NOFs are enlarged cortical defects that have expanded into the medullary cavity. 16 In the radiology literature, they are considered distinctly different lesions: both Resnick and Greenway 17 and Ritschl et al 2 agree that NOFs are specific to the metaphyseal region, whereas cortical desmoids are specific to the insertion of the adductor magnus tendon at the medial rim of the linea aspera. Resnick and Greenway 17 go on to suggest that NOFs are excavations, forming lytic, concave lesions at the gastrocnemius attachment, whereas cortical desmoids are proliferative cortical irregularities, related to adductor magnus aponeurosis attachment.17,18 While cortical desmoids are typically described as having a relationship with the adductor magnus aponeurosis, there are cases that have been described as arising at the medial head of the gastrocnemius. 18 In the present study, we found NOFs primarily at the origin of the medial or lateral gastrocnemius, but also found four lesions that were radiographically and/or histologically described as NOFs at the insertion of the adductor magnus. Histologically, all of these lesions are the same.13,14 Therefore, the authors of this paper prefer to suggest that all these lesions should be termed NOF or, if preferred, fibrous cortical defects, and omit the term desmoid, since they are radiographically similar and histologically the same.
The strength of this study lies in the fact that it is the largest cohort of specifically NOFs of the distal femur to be presented. By presenting a cohort of 68 NOFs, 40 of which had CT scans and six of which had MRIs, we present a unique look at NOFs and are able to point out striking similarities that lead to hypotheses regarding their origin and aetiology. A weakness of this paper lies in its retrospective design. Another weakness is the predominant use of CT scans over MRIs. Given the relationship between muscular origin/insertion points and bony lesions, there is arguably a benefit to both types of imaging, as CT is generally taken to be better for bone lesions and MRI for soft tissue; however, many authors agree that there is a beneficial role of CT scan in the visualisation of soft tissues.19–22 With 93% of our CT scans and 100% of our MRIs showing a relationship between the NOFs and muscular attachments, we suggest that there is both reliability and accuracy in both forms of imaging.
The present study suggests that there is a clear relationship between tendinous/fibrous structures’ pull on bone and the origin of NOF lesions in 93% of the distal femoral lesions, however, their origin and behaviour are more complex than the original ‘tug lesion’ theory that suggests that the lesions only occur where tendons insert into the perichondrium of the epiphyseal plate supporting Ritschl et al's 2 theory. These lesions may occur at the origin of the head of the lateral gastrocnemius much more frequently than previously thought. They are also seen to travel into the diaphysis of the bone as the patient grows. Finally, our three lesions that do not appear to have a tendinous attachment suggest that there is an additional factor in the aetiology of NOFs that can rarely cause them to occur without a ‘tug’. Given our description of NOFs at the attachments of the medial gastrocnemius, lateral gastrocnemius and adductor magnus, as well as the knowledge that NOFs are histologically identical to cortical desmoid lesions, we propose that a single consensus term should be used to describe this pathology in order to limit confusion. The often-used term ‘fibrous cortical defect’ may, in fact, be a better term for all of these lesions. More research is required to determine the exact cause of the NOF and why it presents with its particular histologic pattern.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.