
Abstract
Purpose
Intra-operative imaging plays a key role in screw placement for slipped capital femoral epiphysis (SCFE). Complications have been associated with inadequate screw position. The purpose of this study was to evaluate computed tomography (CT) (3D fluoroscopy) and standard fluoroscopy (C-arm) images as compared with direct anatomic measurement to determine final screw position in a cadaveric SCFE model.
Methods
Osteotomy with pinning was performed at the physeal scar in ten cadaveric hips. A standardised approach-withdrawal technique was performed with C-arm images taken at 15° increments. We also obtained a CT (3D fluoroscopy) scan of each hip. The screw tip-subchondral bone (STSB) distance was measured on digital imaging software and also with a digital calliper directly when the femoral head was cut in plane to expose the STSB distance anatomically. Statistical analysis included t-tests and Fisher's exact test.
Results
Moderate SCFE osteotomies were achieved with a mean Southwick angle (39.5° ± 7°). The 60° fluoroscopic image was found to be the most representative image (41% of the time) compared with both anteroposterior (AP) and lateral images (8% and 21%). Both fluoroscopy (2.7 ± 0.8 mm, p < 0.001) and CT (1.6 ± 0.7 mm, p = 0.03) overestimated the STSB distance compared with direct measurement (0.94 ± 0.51 mm). Two-thirds (67%) of CT measurements were within 1 mm of the cadaveric measurement, while only 20% of C-arm measurements fulfilled this criterion (p = 0.04).
Conclusions
Both standard fluoroscopy and CT overestimated the STSB distance when compared with direct measurement in a cadaveric model of SCFE. Surgeons should be aware of the limitations of intra-operative imaging to determine the STSB distance. We suggest that using the known pitch of a screw (2.9 mm in a 7.3-mm cannulated screw) as an intra-operative tool to help guide screw placement.
Introduction
Slipped capital femoral epiphysis (SCFE) is the most common hip condition among adolescents.1,2 In situ pinning is the treatment of choice in many institutions for stable SCFE and is also a widely used option for an unstable SCFE.3–5 In situ pinning complications include femoral neck fracture, avascular necrosis (AVN) and chondrolysis.6,7 Errant screw placement is also considered a major risk factor for complications.8,9 AVN is most commonly associated with unstable slips, but both AVN and chondrolysis can result from unrecognised screw penetration into the subchondral bone or hip joint. 4 The literature suggests a safe screw tip-subchondral bone (STSB) distance in the range of 2.5 mm to 5 mm.10,11 This distance is balanced by the need for an adequate number of threads crossing the physis to maintain fixation while minimising the risk of the epiphysis growing off the screw. 12
Intra-operative imaging plays an essential role in determining accurate screw placement in SCFE fixation. Various methods have been proposed in the literature including mathematical models13,14 and the approach-withdraw technique. 15 Many surgeons use the approach-withdraw technique in judging the STSB distance. It is performed by rotating the hip or the C-arm during live fluoroscopy to obtain images that show the screw tip approach the subchondral bone and then subsequently withdraw from the subchondral bone. This point of intersection between the approach and withdraw of the screw tip relative to the subchondral bone defines the smallest distance between the screw tip and the subchondral bone. Although many surgeons use this technique intra-operatively in SCFE fixation, no consensus exists regarding the optimal intra-operative radiographic method for accurate screw tip placement, and the majority of the techniques used are largely based upon surgeon preference. In a recent study, Senthi et al assessed final screw tip placement with intra-operative radiographs as compared with a post-operative computed tomography (CT) scan. 16 They found that the intra-operative radiographs significantly overestimated the STSB distance when compared with the post-operative CT scans. Furthermore, 10% of the hips were found to have unrecognised screw penetration into the hip joint on the post-operative CT imaging. All of these patients required a revision surgery to correct the intra-articular penetration of the screws. Given the additional radiation associated with intra-operative CT imaging, we felt that additional studies evaluating the true accuracy of standard fluoroscopy (C-arm) imaging and CT (3D fluoroscopy) imaging was warranted. The purpose of our study was to compare standard fluoroscopy (C-arm) and CT (3D fluoroscopy) with direct visualisation or direct anatomic measurements using a digital calliper in a cadaveric model to measure the STSB distance.
Materials and Methods
A total of six cadavers were used in this study. Two hips had previous arthroplasty (one total hip arthroplasty and one hemiarthroplasty), thus a total of ten cadaver limbs were utilised. A Smith-Peterson approach was used to access the hip joint. The rectus femoris was detached and reflected distally for better exposure and an anterior capsulotomy was performed. The hips were then dislocated anteriorly with adduction and external rotation of the leg. An oscillating saw was used to create an osteotomy at the level of the subcapital femoral neck. A small portion of the posterior neck was then removed at a 45° angle. Smooth 2.0 mm K-wires were placed in the periphery and perpendicular to the osteotomy to temporarily maintain the slipped ‘epiphysis’ (Fig. 1). Three radial cuts were then made in the labrum to facilitate reduction of the femoral head while preventing undue forces across the osteotomy site. One 7.3 mm cannulated screw was then placed per standard operative technique under direct fluoroscopic guidance. For final screw placement, we attempted to place the screw tip in a centre-centre position within the epiphysis and 3 mm short of the subchondral bone. We used the known screw pitch of a 7.3 mm cannulated screw (2.9 mm) as a visual estimate.

Osteotomy of the femoral head creating the slipped capital femoral epiphysis lesion in cadavers.
After final placement of the screw, a standardised approach-withdrawal technique was performed and fluoroscopic images (GE OEC 9900 Elite Mobile C-arm, General Electric Company, Fairfield, Connecticut) were taken with the C-arm at 0° (anteroposterior (AP) to the hip in neutral position), 15°, 30°, 45°, 60°, 75° and 90°. We measured the STSB distance on plain fluoroscopic imaging in these 15° increments. Subsequently, we obtained a scan of each hip using a Siemens Orbic 3D Fluoroscopy machine to obtain axial, coronal and sagittal images (CT equivalent) (Fig. 2). The STSB distance was measured on each standard and CT image using a digital imaging software system (Imagecast, General Electric Company). A proximal femoral osteotomy was performed at the inferior border of the lesser trochanter. 17 A cut parallel to the screw in the coronal plane was made through the femoral neck and head of each specimen to expose the screw tip (Fig. 3). A digital micrometre was used to take a direct measurement of the STSB distance on the anatomic specimen. Standard fluoroscopy and CT (3D fluoroscopy) were then compared with each other and with the direct anatomic cadaveric measurements. For standard fluoroscopy, the image with the smallest STSB distance value was used for our comparative analysis and termed C-arm Composite Value. The C-arm Composite Value was chosen to most closely represent the clinical scenario of an approach-withdrawal technique. Statistical analysis was performed with two-tailed t-tests for continuous variables and Fisher's exact tests for dichotomous variables.
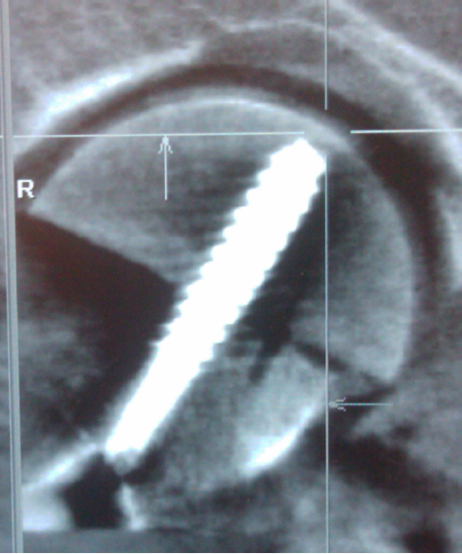
CT (3D fluoroscopy) imaging in coronal plane used to measure the screw tip-subchondral bonedistance.

Example of anatomic specimens used for direct visual measurements of the screw tip-subschondral bone distance using a digital calliper.
Results
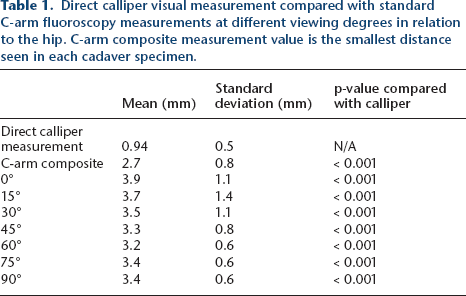
A total of ten hips were included in our study with 50% from female cadavers. The mean specimen age was 68 years. The mean Southwick angle for our SCFE model was 39.5° ± 7° with a range from 31° to 55°. With standard fluoroscopy (C-arm), the mean STSB distance in the AP image (0°) was 3.88 mm ± 1.04 mm and 3.34 mm ± 0.53 mm in the lateral image (90°), respectively. The 60° image had the smallest STSB distance 41% of the time, while the AP and lateral images had the smallest STSB distance only 8% and 21% of the time, respectively (Table 1). There was no concern for subchondral bone penetration in any of the cadaveric hips based on standard fluoroscopic imaging.
Direct calliper visual measurement compared with standard C-arm fluoroscopy measurements at different viewing degrees in relation to the hip. C-arm composite measurement value is the smallest distance seen in each cadaver specimen.
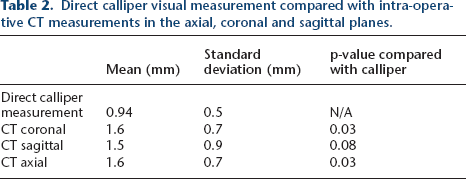
The mean STSB distance on the CT images (3D fluoroscopy) was 1.6 mm ± 0.7 mm in the coronal series, 1.6 mm ± 0.7 mm in the axial series and 1.5 mm ± 0.9 mm in the sagittal series (Table 2). For the cadaveric measurements obtained with the digital calliper under direct visualisation, the mean STSB distance was 0.94 mm ± 0.5 mm. Additionally, the cadaveric specimens, mean cartilage thickness was 2.1 mm ± 0.5 mm. The thickness of the subchondral bone region was < 0.5 mm in all specimens. There were no instances of screw penetration past the cartilage surface. However, there was one specimen that had a subchondral bone disruption by the screw tip. For this specimen, the mean STSB distance was 2.05 mm on the AP image, 2.74 mm on the lateral image and 0.8 mm as measured on CT.
Direct calliper visual measurement compared with intra-operative CT measurements in the axial, coronal and sagittal planes.
When we compared the two imaging measurements with each other and with the direct cadaveric measurements, we found that the STSB distance was less in cadaveric measurements (0.94 mm ± 0.5 mm) as compared with either standard fluoroscopy (2.7 mm ± 0.8 mm, p < 0.001) or CT (1.6 mm ± 0.8 mm, p < 0.005). Two-thirds (67%) of CT (3D fluoroscopy) measurements were within 1 mm of the cadaveric measurement, while only 17% of standard fluoroscopic measurements were within 1 mm (p = 0.036). Compared with the direct cadaveric measurement, both standard fluoroscopy and CT (3D fluoroscopy) overestimated the STSB distance by an average of 170% and 71%, respectively (p < 0.005).
Discussion
To our knowledge, this is the first study to compare intra-operative imaging with a cadaveric measurement for accurate placement of cannulated screws in SCFE. Furthermore, we could not find any literature assessing the relationship between intra-operative imaging and cadaveric dissection of a paediatric hip implant. In SCFE, accurate interpretation of intra-operative imaging studies is crucial for optimal placement of cannulated screws during in situ pinning. For pinning with one screw, the ideal location of the screw tip is thought to be in a centre-centre position within the epiphysis. 18 The importance of accurate implant placement increases with implant density. In the setting of unstable SCFE, multiple authors recommend fixation with two screws.19,20 Two-screw fixation increases the distance of the screw tip from the centre of the epiphysis, which narrows the gap between the physis and subchondral bone (given the spherical shape of the femoral epiphysis), thus increasing the risk of screw penetration. While we focused our study on in situ pinning with one screw, the implications and results of this study will also apply to a two-screw scenario as well.
Optimal STSB distance is quite varied in the literature, ranging from 2.5 mm to 5 mm.10,11 There is a balance between the need for sufficient screw threads to cross the physis to confer stability while minimising the risk of screw tip penetration into the hip joint.12,21 It should be noted that there is no consensus for either the ideal STSB distance or the ideal number of threads within the epiphysis. To standardise our screw placement, we sought to place the screw tip at one screw pitch distance away from the subchondral bone. This distance, as dictated by the pitch of the screws used in our study, was 2.9 mm for the 7.3-mm cannulated screw (Synthes, West Chester, Pennsylvania). For practical purposes, we found that knowledge of the screw pitch for the particular screw used is a helpful intra-operative tool to guide placement of cannulated screws. As the magnification of the C-arm imaging changes with the distance of the limb to the C-arm plate, using the known screw pitch distance to judge the STSB distance is an excellent technique to help avoid screw tip penetration into the hip joint.
Multiple methods of screw tip assessment have been proposed.10,15,22 CT technology has been used to assess implant placement post-operatively.11,16 Additionally, intra-operative navigation has also been proposed as a method to improve implant placement.11,23,24 Given the concerns regarding radiation dose with different imaging techniques, we sought to compare CT with traditional fluoroscopy using direct cadaveric visualisation measurements as the standard for these comparisons. We found that CT (3D fluoroscopy) (1.6 mm ± 0.8 mm) more closely approximated our direct cadaveric measurements (0.94 mm ± 0.5 mm) than the C-arm fluoroscopy measurements (2.7 mm ± 0.8 mm). We acknowledge that the difference between CT (3D fluoroscopy) and standard fluoroscopy is relatively small and therefore we do not recommend that advanced image technology be used as a standard imaging technique for in situ pinning with SCFE. Both imaging techniques overestimated the STSB distance. Thus, it is essential for the surgeon to allow a minimal distance of the screw's pitch (2.9 mm) to the subchondral bone to prevent screw penetration to the hip joint. We recommend that the surgeon be one pitch or a minimum of 3 mm away from the subchondral bone (7.3-mm cannulated screw). Furthermore, it is notable that the AP and lateral standard fluoroscopy images obtained rarely had the smallest STSB distance. The 60° image was found to be the most frequent image with the smallest STSB distance. This finding emphasises the importance of using multiple images intra-operatively, such as an approach-withdrawal technique to assess placement of a cannulated screw in SCFE.
Regarding the number of recommended threads crossing the physis, children have variably sized epiphyses and therefore a strict recommendation on threads across the physis is limited. From our perspective, it is recommended to have as many threads as possible across the epiphysis while maintaining a safe 3 mm distance away from the subchondral bone. It is also important to note that when two screws are used in an unstable SCFE, the distance between the physis and the subchondral bone decreases due to the spherical nature of the epiphysis. The screws cannot be placed in a centre-centre position as in the case of one-screw fixation. Therefore, there is a higher risk of subchondral bone penetration and caution is warranted. From our perspective, if the surgeon knows the exact pitch of the screw that he is using (2.9 mm on a 7.3-mm cannulated screw), this distance will be essential to help judge the real STSB distance independent of the magnification of the C-arm.
This study has several limitations. SCFE is a paediatric condition. The average age of the cadavers was 68 years, which may have led to differences in the thickness of the cartilage and subchondral bone quality when compared with children. Also, many patients with SCFE are overweight but we only had access to thin cadaveric specimens, 2 thus the radiographic images in our study may have been higher in quality than images obtained clinically. The in vitro nature of this investigation may have led to differences in the quality of our imaging. There were also a small number of specimens used in this study as limited by access. None of our specimens were found to have a history of SCFE. Therefore, our study necessitated the creation of an artificial SCFE via osteotomy. We also did not specifically assess whether the difference between the C-arm and the actual distance measured anatomically differed based on the Southwick angle. Furthermore, the proximal femoral anatomy is three-dimensional in nature. Both imaging studies are two-dimensional which is another limitation of the study. Additionally, we used increments of 15° to measure the STSB distance, which may have missed the point of maximal proximity of the screw tip to the subchondral bone. Finally, inter-observer and intra-observer variability were not assessed and we did not evaluate the amount of radiation that is associated with the CT (3D fluoroscopy technique) compared with the standard fluoroscopy technique.
In conclusion, we found that intra-operative imaging studies overestimate the STSB distance with in situ pinning of a cadaveric SCFE model. We suggest using the known pitch of a screw (2.9 mm in a 7.3-mm cannulated screw) as an intra-operative tool independent of the magnification to help guide screw placement. Our study does not support the use of CT with 3D fluoroscopy technology for routine SCFE cases. Multiple image methods such as the approach-withdrawal technique should be performed intra-operatively to determine the closest point of the screw tip to subchondral bone to avoid penetration into the hip joint. Surgeons should be aware of the limitations of fluoroscopy, even with the use of the approach-withdrawal technique, given the propensity for overestimation of the STSB distance.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
The Orthopaedic Research Education Fund (OREF) funded this study through a research grant. The article does not contain any studies with animals performed by any of the authors. This article does not contain any studies with human participants performed by any of the authors.
XL reports financial support outside the current work in the form of consultancy fees for Mitek Inc., and Tournier Inc. Additionally, unrelated to this study, he is on the editorial board of Journal of Medical Insight (JoMI) and holds equity in the company. He also is on the editorial board of World Journal of Orthopaedics and Orthopedic Reviews. Additionally, unrelated to this paper, he is on the Electronic Social Media Board of the American Journal of Sports Medicine.