
Abstract
Vascular ultrasound is a reliable non-invasive tool used for the routine assessment of vascular flow and patency in human recipients. We describe the use at three different time points (immediately, 1 week and 4 weeks postsurgery) of ultrasound studies and its validation by angiographic studies in 37 swine undergoing carotid graft replacement. We calculated predictive values (>92%), sensitivity (>85%) and specificity (>92%) with high results at all time points. Ultrasound appeared as an accessible non-invasive technique, providing rapid, safe, repeatable and reliable results. It is an excellent alternative to angiography, avoiding risks inherent to invasive methods and therefore contributing to animal welfare.
Ultrasound is a non-invasive diagnostic tool widely used in human and veterinary medicine under clinical conditions, to visualize soft tissues and internal organs. A very comprehensive anatomical and functional evaluation may be achieved by the combination of three basic techniques: bi-dimensional (2D), M-mode and Doppler with or without colour. Ultrasound studies start with a proper 2D anatomic assessment, complemented by M-mode and Doppler studies. This latter is the cornerstone of the functional evaluation, particularly concerning the characteristics of flow within cardiac or vascular structures. Cardiovascular pathologies account for one-third of deaths throughout the world 1 and among these pathologies, vascular disease is a major problem. Although the surgical replacement of affected vessels is a common practice, availability of grafting material of choice (native autologous vessels) can be scarce in subjects who have already undergone vascular surgery or have very limited vascular reserves. Therefore, experimental and clinical research is targeting the development of new materials, degradable or not, that could replace autologous vessels in human recipients. Due to anatomical and physiological similarities with humans, swine are good models in cardiovascular research. 2 They are used to study a wide variety of morbid processes, e.g. myocardial infarction, congenital heart diseases, heart transplants, haemodynamics and shock, atherosclerosis, hypertension, for the development of intravascular devices (stents) and vascular surgery and grafts. 3–6 The number of animals involved is important; according to the European Biomedical Research Association (EBRA), in the European Union, the 2002 statistics indicate that 61,164 pigs were part of laboratory experiments 7 and non-invasive techniques could benefit a large part of these individuals.
The importance of having reliable diagnostic resources derives from the fact that after vascular surgery it is essential to assess the patency of the vessel and its blood flow characteristics. The reference tool or gold standard for this assessment is the angiography. However, this invasive method may carry significant consequences, particularly in animals, namely longer anaesthesia, localized pain at the site of puncture, bleeding, lameness, supplementary stress and higher costs and in the case of our swine, early sacrifices due to humane endpoints related to the aforementioned complications.
All these secondary events become even more important in the chronic follow-up, where several examinations might be needed. Ultrasound studies, like 2D and Doppler imaging could become a reliable replacement method to the angiography. Yet, little has been published about the importance and efficacy of this non-invasive method in the postoperative vascular assessment in animals and particularly in the pig. Ultrasound has the potential to be further exploited under research conditions for different organs and studies. Alongside to a vascular graft implantation project, our aim was to implement and validate the vascular ultrasound as a non-invasive alternative to angiography in the pig.
Materials and methods
We performed this prospective study between October 2003 and March 2007. The animals included in this project were part of a parallel experiment on vascular surgery (vascular graft implantation). All the protocols were approved by the Ethics Committee of the University Hospital in Geneva and the local and Federal Swiss Veterinary Office, according to European Community (EC) Directives, Federation of European Laboratory Animal Science Associations (FELASA) and Swiss Federal regulations.
Animals
Thirty-seven female Yorkshire pigs, weighing approximately 30 kg, were purchased at a local farm and good health status was confirmed by a veterinarian before admission to the animal facility (‘Animalerie du Centre Médical Universitaire’, CMU) in Geneva four days prior to the surgical intervention. They were housed individually and remained in these premises during one week for the postoperative period and then transferred to an experimental farm of the University of Geneva, where they were also housed individually, until the end of the protocol. They were then transported back to the CMU for final examinations and euthanasia. In both facilities, water was supplied ad libitum and Nutriporc® (Provimi, Cossonay-Gare, Switzerland, growing pigs 25–100 kg feed) was provided according to their weight to maintain a proper nutritional programme; the light cycle was 12 h of light for 12 h of darkness, with a relative humidity of 38–40% and a temperature of 22 ± 2°C. As an enrichment factor, the animals were supplied with wood blocks and chains; they were also within short visual and audible distance of each other. The cages had concrete flooring, which was cleaned daily and, due to University protocols, no bedding material was used.
Anaesthesia
The animals were fastened 12 h prior to the vascular surgery. Premedication was provided by intramuscular injection with a mixture of azaperone (6 mg/kg; Stresnil®, Jansen Biomedika, Crissier-Lausane, Switzerland), midazolam (500 mcg/kg; Dormicum®, Roche Pharma, Reinach, Switzerland) and atropine sulphate (0.05 mg/kg, Bischel Interlanken, Switzerland). Anaesthesia was induced by mask with isoflurane 5% (Abbott, Baar, Switzerland). Endotracheal intubation with a 6 mm silicone tracheal tube (Hi-ContourTM, Mallinchrodt, Ireland) followed for the maintenance of anaesthesia with isoflurane 1.5–2% and oxygen 40%, under volume-controlled-assisted ventilation (Servo Siemens 900D®, Elema, Sweden). All the animals received prophylactic antibiotics (Zinacef®, 750 mg, Glaxo Smith Kline, AG Munchenbuschee, Switzerland) and fentanyl infusions during surgery (Syntenyl®, 40 µg/kg/h, Sintetica SA, Switzerland). Ringer lactate solutions were administered during the surgery as maintenance fluids. Postoperative pain control was achieved by intramuscular injections of buprenorphine (Temgesic®, 0.2 mg/kg, Essex, Luzern, Switzerland) twice a day for 48 h.
The ultrasound examinations were performed under a lighter anaesthetic protocol, without intubation. After the aforementioned premedication, isoflurane 3% and oxygen 40% were administered by facial mask for the duration of the procedure.
At the end of the experiment, the animals were brought back to the CMU for final ultrasound and angiographic examinations, followed by euthanasia. Premedication was as previously mentioned, followed by intubation. For this terminal procedure, the anaesthetic protocol used was the same as for the vascular surgery. At the end of the procedure (after ultrasound and angiographic studies were performed), isoflurane was increased to 5% and a bolus of fentanyl was administered, until a stage IV of anaesthesia was attained. Euthanasia was then performed by intravenous injection of potassium chloride 7.5% (Sintetica-Bidren, Couvet, Switzerland).
Surgical procedures
Cardiovascular surgeons performed all the vascular replacements under strict aseptic conditions.
A bilateral carotid interposition was achieved via a median neck incision to implant two grafts, expanded polytetrafluoroethylene (ePTEE) on one side, and a contralateral bare or coated graft of a different material (e.g. vascular endothelial growth factor [VEGF] or titanium). Detailed surgical techniques have been described in the literature by Walpoth et al. 8 and Cikirikcioglu et al. 9
Angiographic examinations
Angiographic studies were carried out immediately (5–10 min) postoperatively, at one week and/or at four weeks, as per the following algorithm:
Immediately postsurgery (15 pigs, n = 30 sides examined); One week postsurgery (5 pigs, n = 10 sides examined); Four weeks postsurgery (28 pigs, n = 56 sides examined).
Before euthanasia, cardiovascular surgeons performed the angiographies (General Electric, Cardiac Series 9800, Salt Lake City, UT, USA), under strict aseptic conditions, via the left or right femoral arteries and blindly in regard to the results of the ultrasound. Femoral catheterization was performed through an oblique incision in the inguinal plication. After proximal and distal clamping of the artery, a small incision was made to introduce a 6Fr Terumo® catheter (Terumo Corporation, Yamanashi, Japan), guided by a hydrophilic guidewire (Radiofocus Angled Guide Wire, 0.89 mm/150 cm, Terumo Corporation). The catheter progressed within the vessel until reaching the carotid bifurcation, and then an angiographic catheter (Cordis MPA 1 multipurpose catheter, 0.97 mm/100 cm, Cordis Corporation, Hialeah, FL, USA) was exchanged over the guidewire. The final position of this latter for selective carotid angiographies was attained by injecting small amounts of radio opaque solution. We then injected by hand 10–15 mL of angiographic solution and recorded the images, on digital subtraction angiography (General Electric, Cardiac Series 9800). After completing angiographies on both carotid sides, the catheter was pulled out and the arteriotomy was closed with two 7/0 prolene suture points, followed by declamping of the artery and closure of muscle and skin, by planes.
Ultrasound examinations
Two cardiologists (cardiologist A completed the 2 first ultrasounds immediately after surgery and cardiologist B all other examinations) performed ultrasound studies, with a linear Vingmed® 10 MHz probe, to obtain 2D images, followed by colour Doppler images (VingmedTM CFM800C System Ltd, Horten, Norway), hence acquiring simultaneous flow information and greyscale images.
Ultrasound studies were carried out immediately postoperatively, at one week and/or at four weeks:
Immediately postsurgery (15 pigs, n = 30 sides examined); One week postsurgery (5 pigs, n = 10 sides examined); Four weeks postsurgery (28 pigs, n = 56 sides examined).
For this purpose, the animals were anaesthetized, according to the previously described protocol, and set in dorsal recumbency. A 5 mm thick layer of ultrasound gel (Aquasonic 100®, Parker, Fairfield, NJ, USA) was applied topically, in the previously shaved area distal to the mandibular condyle, along the jugular furrow. With the probe perpendicular to the skin and transversal to the vessel axis, a set of sweep images was obtained. The operator adjusted the sound beam perpendicular to the far wall of the graft, focusing on the acquisition of two parallel echogenic lines corresponding to the lumen interfaces. In order to optimize the image and reduce artefacts, we used the lowest possible pulse repetition frequency (PRF) without aliasing, and maximum colour and power gain without background noise. If no adequate flow was seen under standard conditions, further adjustments were made to gain quality (increase of transmission power and decrease of wall filter and PRF). To assess the pulsed Doppler velocity profile, we chose an angle of insonation inferior to 60°, and standardized sequential longitudinal and axial views of the entire extracranial carotid system, using greyscale, colour and spectral modalities.
The gain setting was adjusted to visualize 2D images for proximal and distal walls, separated by an echo/free space, associated with a linear Doppler colour flow inside the graft, defining the degree of patency (Figure 1). A stenosis was defined as any narrowing of the lumen or at the site of the arterial anastomosis with or without a turbulent Doppler colour flow (Figure 2). An occlusion was defined as an obstruction of the graft lumen by thromboses, represented as a large 2D echogenicity, without any detectable flow by Doppler (Figures 3a and b). Vascular tissue dilation was defined as an enlargement of the vessel.
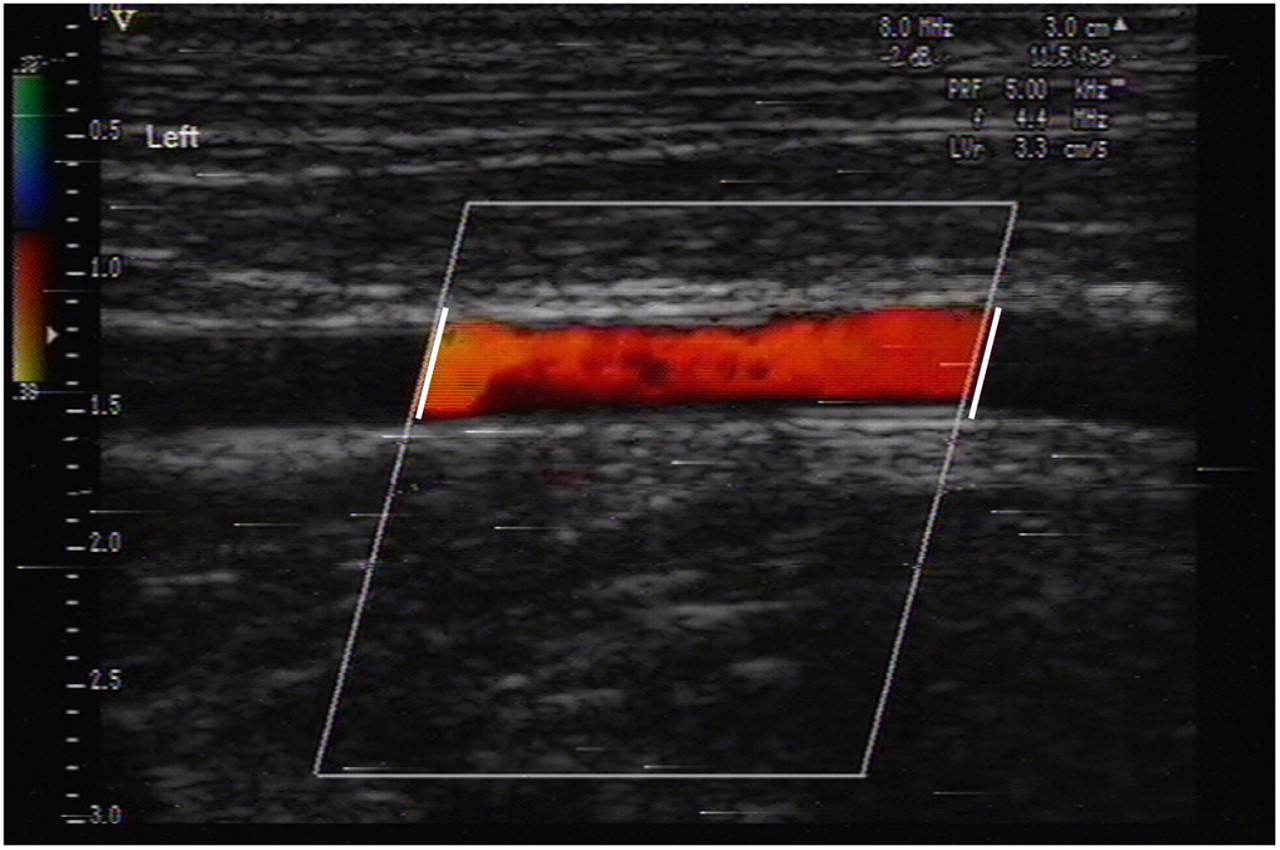
High-resolution B-mode and colour Doppler imaging showing a patent graft demonstrated by a colour laminar flow (between white lines)
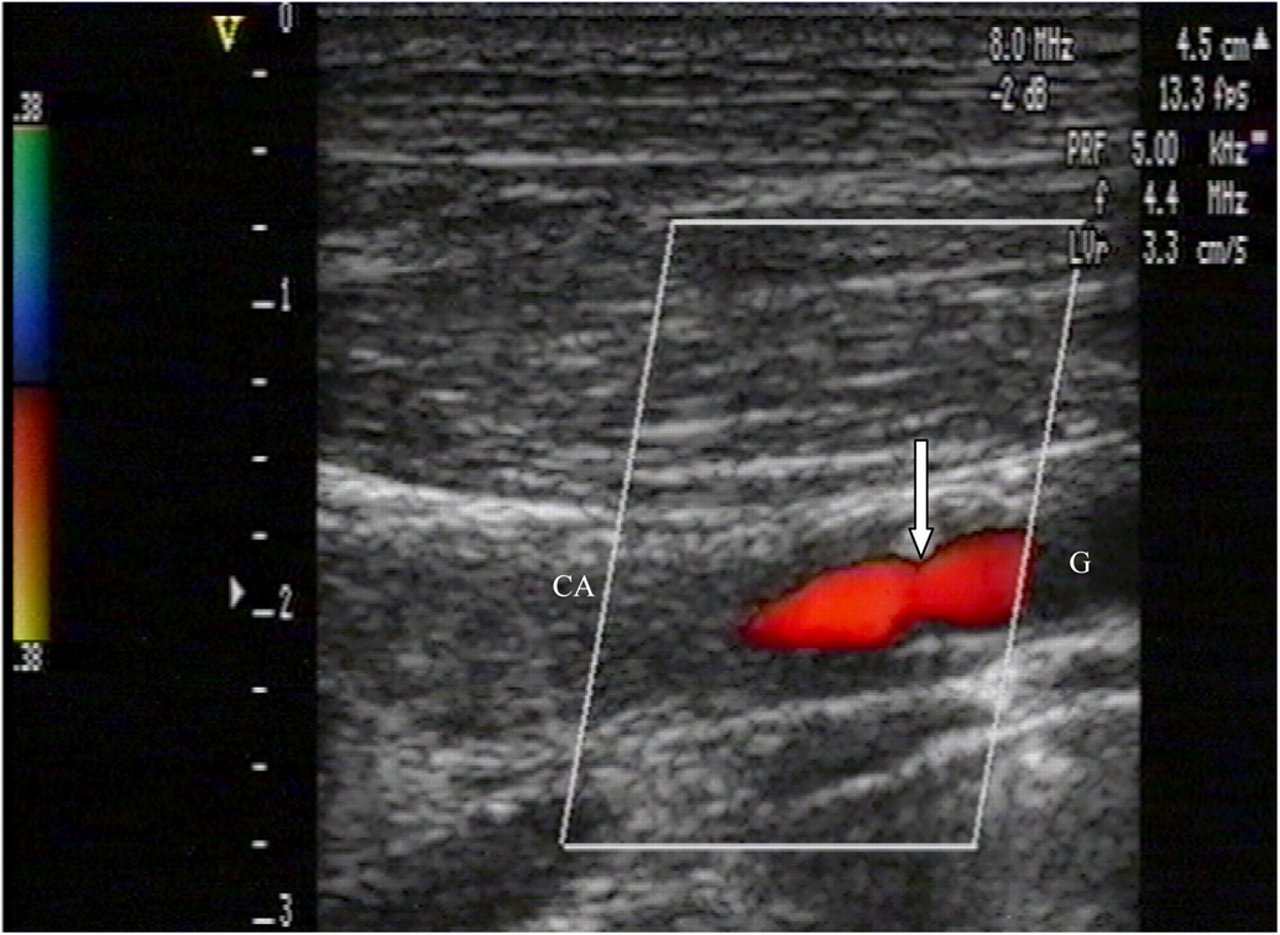
High-resolution B-mode and colour Doppler imaging showing a middle narrowing of the anastomosis between the graft and the native carotid artery (arrow) without any turbulent flow
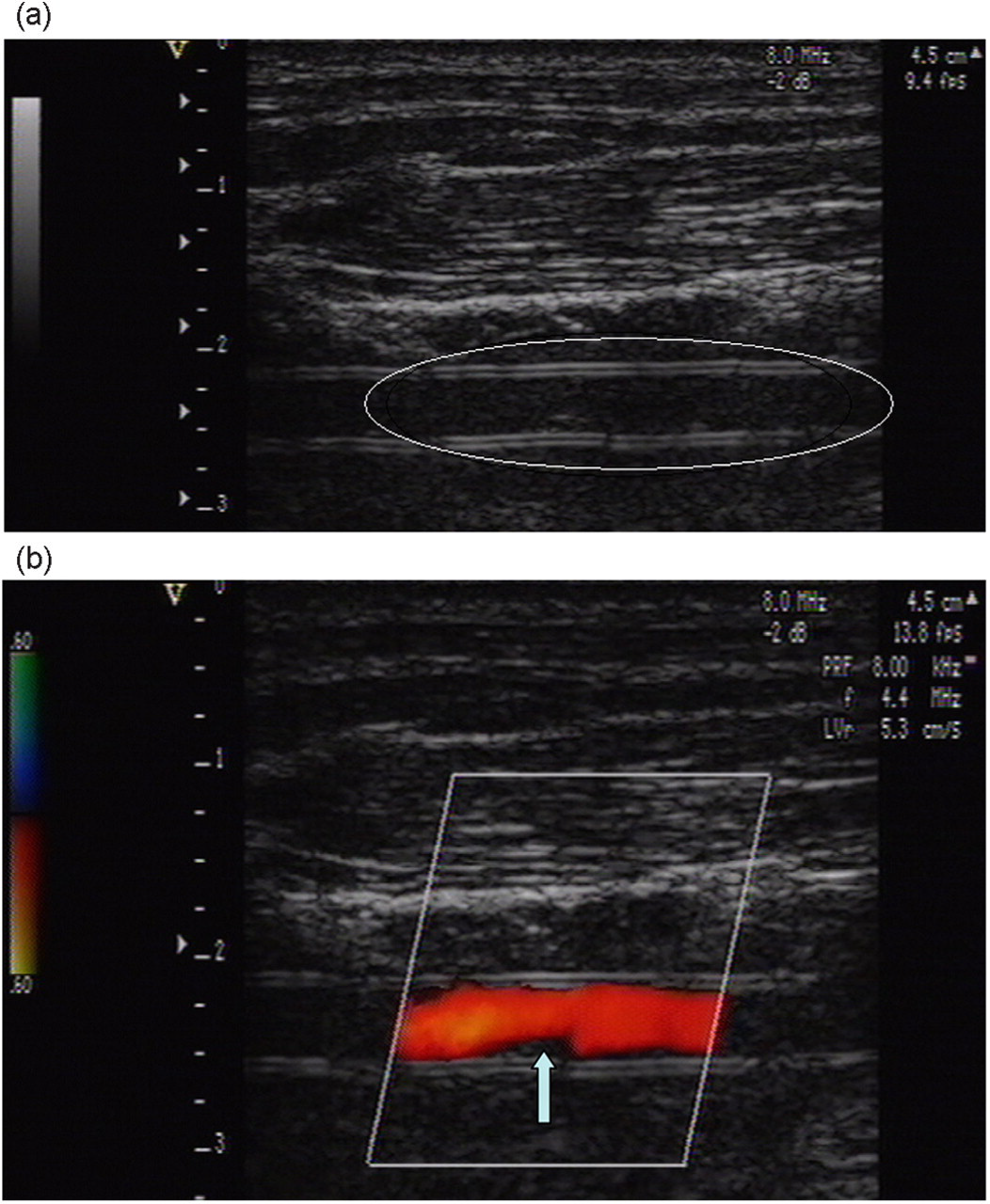
An abnormal echogenicity (a) described one week postsurgery inside the lumen of the graft without any turbulent flow in colour Doppler (b) corresponding to a postoperative microthrombosis
Statistical analysis
The animals included in this project were part of a parallel experiment on vascular surgery. Positive predictive values (PPV), negative predictive values (NPV), sensitivity and sensibility tests were calculated for each time point (
Results
Statistical results indicate a high sensitivity and specificity.
Immediately after surgery (n = 30), the results between ultrasound and angiography corresponded in 28/30 measurements (2 false positives), with NPV = 100%; PPV = 67%; sensitivity = 100%; specificity = 92%. In one of the cases, the ultrasound result diagnosed an occlusion but the angiography showed that, although an important stenosis was present, there was still a very marginal blood flow. The other case was probably due to a mechanical problem of the ultrasound machine, since due to a poor signal the examiner could not confirm the diagnosis. A single observer, cardiologist A, less experienced in ultrasound techniques, performed both of these cases. Angiographic examinations, performed under full anaesthesia, lasted 30–45 min.
At one week (n = 10), there was a 100% correspondence between the ultrasound and the angiographic results. NPV = 100%; PPV = 100%; sensitivity = 100%; specificity = 100%.
At four weeks (n = 56), the angiography confirmed ultrasonographic findings in 53/56 examinations (with 1 false positive and 2 false negatives). The false-negative results correspond to a doubtful diagnosis of stenosis, but the angiography confirmed a very small flow still present. NPV = 95%; PPV = 92%; sensitivity = 86%; specificity = 92%.
Two pigs had ischaemic complications as a consequence of angiography, one of which had to be euthanized before the end of the protocol. Four animals presented limping after angiography.
All ultrasound examinations were performed under rapid sequence mask anaesthesia with a duration less than 30 min. No complications related to the anaesthetic were observed after the procedures.
Different types of ultrasound findings can be described. The laminar flow in Figure 1 indicates a patent graft. A stenosis at the anastomosis can be observed in Figure 2. Figure 3a shows an abnormal echogenicity inside the lumen of the graft, we can also clearly differentiate the walls of the graft. Figure 3b shows a microthrombus attached to the wall of the graft. The precision of the Doppler allows a clear view of the anastomosis, where suture points can be differentiated and pointed out (Figures 4a and b). An intraluminal thrombus is evident in Figure 5a, Figure 5b represents the matching angiographic image, where one side is clearly patent and the other occluded, corresponding to the thrombus detected by the ultrasound.
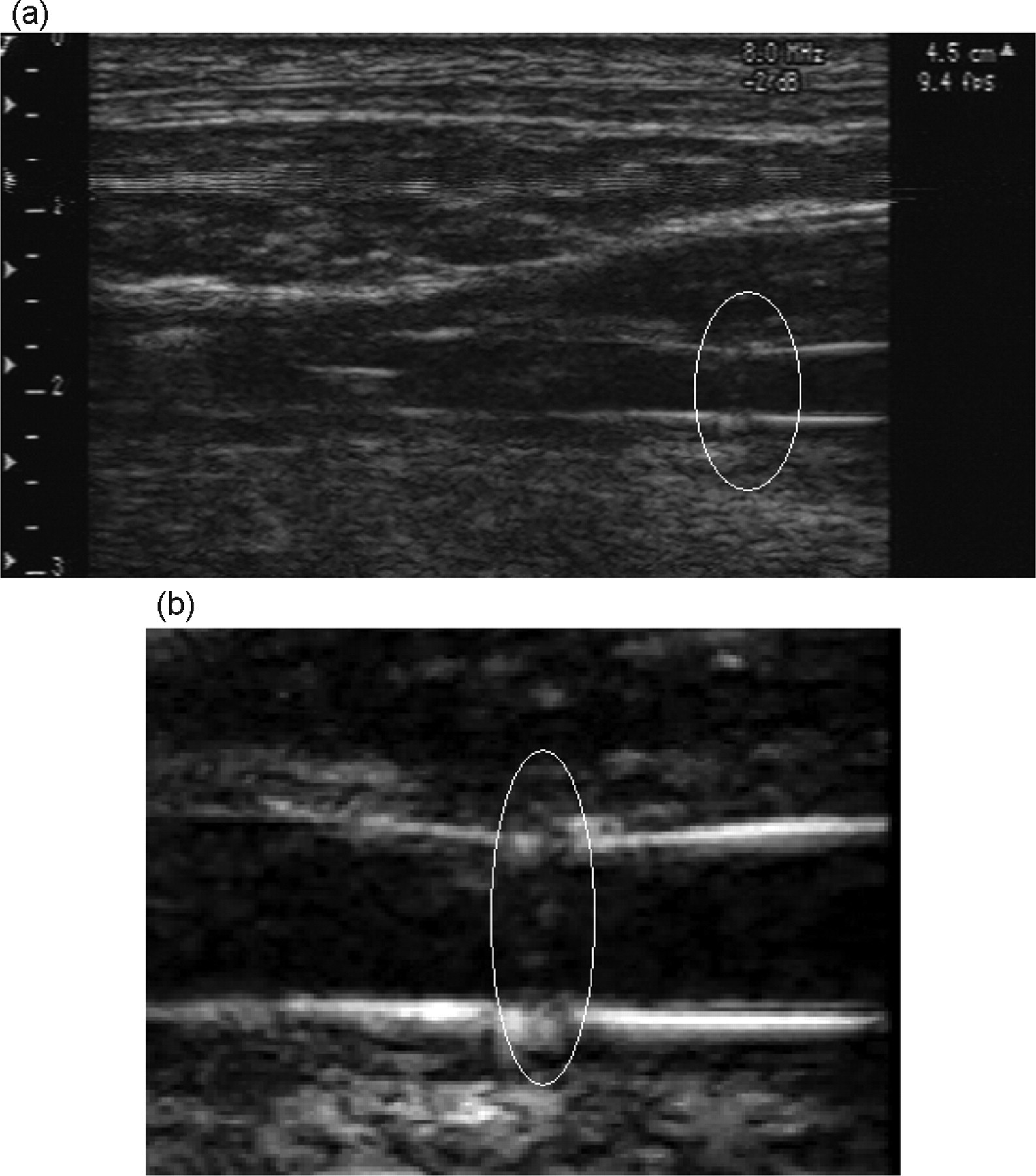
High-resolution B-mode showing the suture points and a small narrowing of the vascular anastomosis. (a) General view. (b) Anastomosis detail using a zoom view
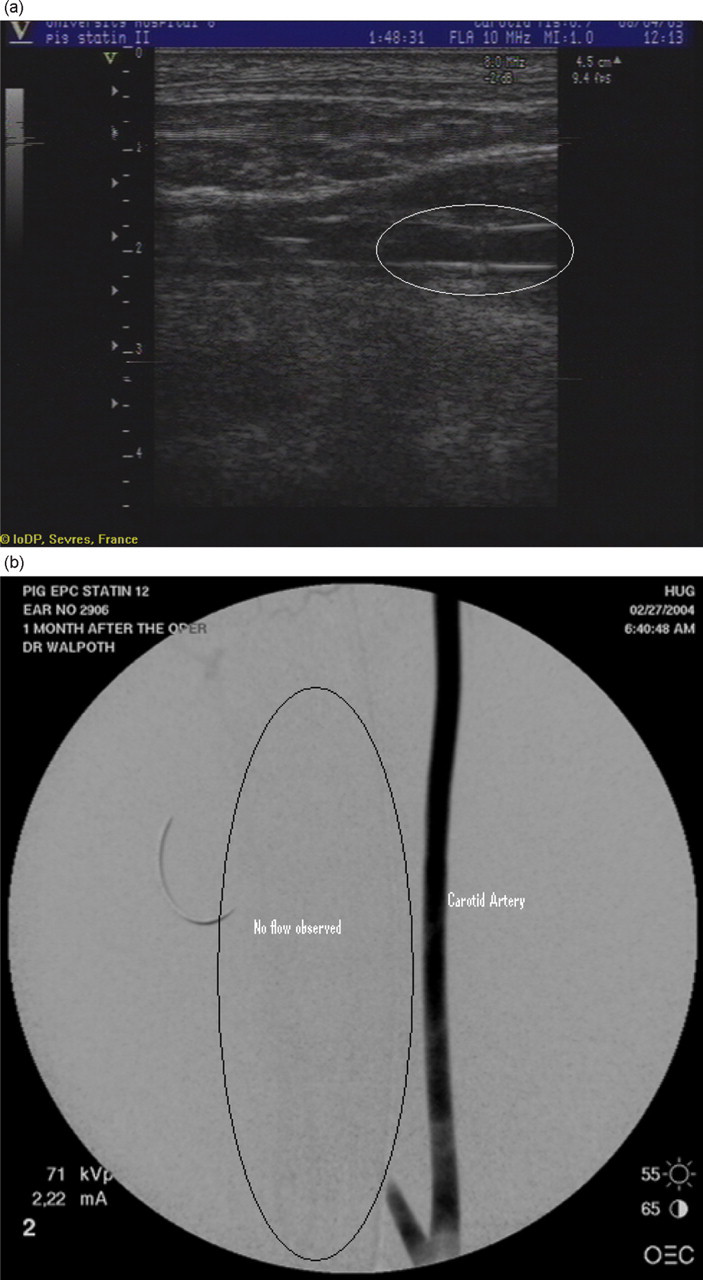
(a) An abnormal echogenicity corresponding to a carotid thrombus, (b) and corresponding angiographic image, one side occluded (no flow) one side patent
Discussion
Vascular ultrasound techniques have been well validated and are widely used in human subjects. In animal models under experimental conditions, this useful tool seems to be underutilized regardless of its potential benefits. We have studied the use of vascular ultrasound at three different time points after vascular surgery in the pig. Predictive values, sensitivity and specificity are high at all time points.
The negative predictive values found, all of them above 93% and specificities above 92%, confirm the excellent capacity of the ultrasound to rule out occlusions. Another important and positive point of the ultrasound examination is the possibility to study flow characteristics and soft tissues surrounding the area of surgery. Through this technique, we identified stenoses (Figure 2), occlusions and thrombosis (Figures 3a and b). The precision can be sufficiently high to identify suture points and suture lines (Figures 4a and b). In the case of stenoses or doubt about patency, 85% or more of sensitivity at all time points provides a confident test to identify the real patent vessels, therefore limiting the use of angiographies to only doubtful cases. This will reduce complications due to the angiographies, such as limping, bleeding, infections and discomfort (i.e. by shorter anaesthesias, shorter recovery times) for the animal and the workload for the team.
Like any procedure, ultrasound demands a learning curve and in our case, the lower results observed for the PPV (66.67%) could possibly be explained by the fact that at this time point (immediately after surgery) two different cardiologists performed the tests and limited experience of one of them might have influenced some of the results (particularly in case of false positives). Oedema and swelling around the implanted prosthesis are also factors that have to be taken into account at this time point, since they can render the examination difficult by decreasing the quality of the image acquisition.
Although one week after surgery, the values of the statistics are perfect (100% for all the tests performed), it must be mentioned that most of these examinations were performed to confirm or rule out a problem, which even under blind conditions, might have somehow biased the results, by inciting the technician to perform a more comprehensive examination. Another limitation at this time point is the small number of animals (n = 10, 5 animals and 10 vessels). Nevertheless, it is for this type of situations that vascular ultrasound could be more useful, since it would permit a follow-up examination with minimal consequences and discomfort for the animal and the handler.
Four weeks after surgery, the PPV, NPV, sensitivity and specificity were again very high. By this time, inflammation had virtually disappeared thus facilitating the ultrasound examination. Once more, the possibility of assessing the flow and the patency of the graft at this time point shows the very important potential of ultrasound for chronic studies.
We concluded that ultrasound is an accessible non-invasive technique, providing rapid, safe, repeatable and reliable results, at any time point after vascular surgery. It is an excellent alternative that avoids risks related to angiography or longer anaesthesia, therefore contributing to animal welfare. It optimizes the standards, and allows an easy evaluation of the surgical results. Ultrasound also provides excellent quality image, good assessment of soft tissues, allowing for reliable evaluation and follow-up of the graft and flow characteristics at lower financial costs. Stress, inconveniences, evaluation time and supplementary postangiographic risks were reduced. Further prospective studies are required in order to optimize the use of this technique and to validate it in other animal models.