
Abstract
Background
Sinonasal inverted papillomas (IP) are benign tumours arising from the mucosal lining of the nasal cavity and paranasal sinuses with a high propensity for recurrence and malignant transformation. Advances in endoscopic surgery and improved radiologic navigation have increased the role of endoscopic surgical resection in the treatment of IPs. The current study aims to evaluate the rate of IP recurrence after endoscopic endonasal resection and to evaluate factors which impact recurrence.
Methods
This was a single-centre retrospective chart review of all patients who underwent endoscopic sinus surgery for management of IP between January 2009 and February 2022. Primary outcomes were the rate of IP recurrence and time to IP recurrence. Secondary outcome measures were patient and tumour factors that contributed to IP recurrence.
Results
Eighty-five patients were included. The mean age was 55.7 and 36.5% of patients were female. The mean follow-up time was 39.5 months. Of the 85 cases, 13 cases (15.3%) had recurrence of their IP and the median time to recurrence was 22.0 months. All recurrent tumours recurred at the attachment site of the primary tumour. The univariate analysis did not identify any significant demographic, clinical, or surgical predictors of IP recurrence. There were no significant changes in sinonasal symptoms at the time IP recurrence was detected.
Conclusion
Endoscopic endonasal resection of IPs represents an effective surgical approach, however, the relatively high rate of recurrence and lack of symptomatic changes at the time of recurrence necessitates long term follow up. Better delineation of risk factors for recurrence can help identify high-risk patients and inform postoperative follow up strategies.
Introduction
Inverted papillomas (IPs) are benign tumours arising from the Schneiderian mucosa of the nasal cavity and paranasal sinuses with either single or multifocal sites of origin [1]. Clinically, patients with IPs present with unilateral sinonasal symptoms such as nasal obstruction and are classically found to have “unilateral nasal polyps” on nasal endoscopy [2–4]. Although IPs are benign tumours, the malignant transformation rate ranges from 5 to 15%, necessitating complete surgical resection and continued surveillance [5–7]. With the advances in endoscopic technology and surgical skills, the mainstay of surgical resection has become a complete endoscopic endonasal resection with identification of the attachment point(s). Open or combined approach is often reserved for complex tumours with extensive frontal sinus involvement, anterolateral and/or inferior maxillary sinus lesions and cases of carcinoma transformation or extra-sinus extension [8–11]. However, the surgical management of IP is challenging with a high recurrence rate ranging from 13 to 35% [12–15]. Notable factors that may increase the chance of recurrence are the multifocality of the tumour attachment and prior surgery [8, 16–18]. The objective of this study is to evaluate the clinical outcomes of endoscopic IP resection and assess clinical factors that may impact the recurrence at a high-volume Canadian tertiary centre.
Methods
Study design and patient population
Approval for this study was granted by the Unity Health Toronto Research Ethics Board (REB #20-012) at St. Michael's Hospital, Toronto, Ontario, Canada. A retrospective review of all adult patients with a diagnosis of IP and who underwent endoscopic resection between January 2009 and February 2022 at St. Michael's Hospital was conducted. All endoscopic endonasal resections were performed by the study's senior surgeon (JML), a fellowship trained rhinologist. Patients were included if they were 18 years of age or older and had a histopathologically confirmed inverted papilloma. Patients who were under 18 years of age and patients who had a diagnosis of squamous cell carcinoma at the time of the initial consultation were excluded from this study.
All patients underwent computed tomography (CT) scans of the sinuses preoperatively. Contrast-enhanced MRI was completed when there were areas of skull base, orbital or carotid artery dehiscence around the suspected tumour site. Additionally, MRI was ordered for all suspected frontal sinus and sphenoid sinus involvement to help ascertain the extent of disease and site of attachment for surgical planning. All patients were seen at regular postoperative visits at 1 week, 1 month, 3 months, 6 months, 1 year, and annually thereafter unless closer follow-up was clinically necessary. Patients completed a 22-item Sino-Nasal Outcome Test (SNOT-22) at each follow-up visit.
Surgical approach and follow up protocol
The general surgical approach has been described previously [19]. Intraoperative frozen sections were used to confirm a pathological diagnosis of IP. The IP was debulked with a microdebrider leaving the attachment site intact. The goal of the surgery was to identify attachment sites and remove the mucosa and underlying periosteum to decrease the chance of recurrence. Angled endoscopes, curved instruments, microdebriders, bipolar cautery and burrs were used for tumour resection and the attachment site ablation. Standard resection included maxillary antrostomy, ethmoidectomy, sphenoidotomy, and frontal sinusotomies. The site of attachment was drilled drown and cauterized with bipolar cautery. Where possible, the bone near the site of attachment was completely removed. Medial maxillectomy, sphenoid drill out and frontal sinus drill out (Draf III) were employed for diseases with attachment sites at the medial maxillary sinus wall, sphenoid sinus, or frontal sinus, respectively [11]. Postoperatively patients are seen every 3 months for the first year and then every 6 months for the next two years. After 3 years, patients are seen annually or sooner if they have symptoms [20]. Patients were typically followed for a lifetime.
Outcome measurements and data collection
Baseline characteristics were collected and included age, gender, and disease presentation status (primary or residual/revision). Primary tumour attachment site(s) was defined as the attachment site(s) identified on initial endoscopic examination in the operating room at the time of first surgery at our institution, although CT images was used preoperatively to gauge the site of attachment. Similarly, Krouse classification was done retrospectively through review of the operative notes [21]. In addition, surgical technique(s), time to recurrence, and follow-up time were extracted. The SNOT-22 score was collected from follow-up notes in order to characterize the association between the severity of IP symptoms both prior and after endoscopic endonasal resection.
Primary outcomes were the rate of IP recurrence and time to IP recurrence. Secondary outcome measures were patient and tumour factors that contributed to IP recurrence.
Statistical analysis
Descriptive statistics were used to summarise continuous and categorical variables. Differences in baseline characteristics between groups were compared using the Chi-squared or independent samples t-test for means, and the Mann–Whitney U test for medians.
Time to recurrence was calculated as the time between the first surgery and the date in which recurrence was identified. Evaluation of recurrence and factors contributing to recurrence of IP was performed with Kaplan–Meier methodology and Cox proportional hazards model.
All available preoperative and postoperative SNOT-22 scores were included in the central tendency calculation. Only patients who had documentation of at least one preoperative and one postoperative SNOT-22 score were included in the calculation of postoperative SNOT-22 changes. Preoperative and postoperative SNOT-22 scores were compared using the Wilcoxon signed rank test. All analyses were performed using SPSS software (version 28.0; SPSS Inc, Chicago, IL, USA), with two-sided statistical significance set to p < 0.05.
Results
Baseline patient characteristics
Demographic characteristics

CI confidence interval; HR hazard ratio; IP inverted papilloma; IQR interquartile range; SD standard deviation
Clinical and surgical characteristics of patient cohort
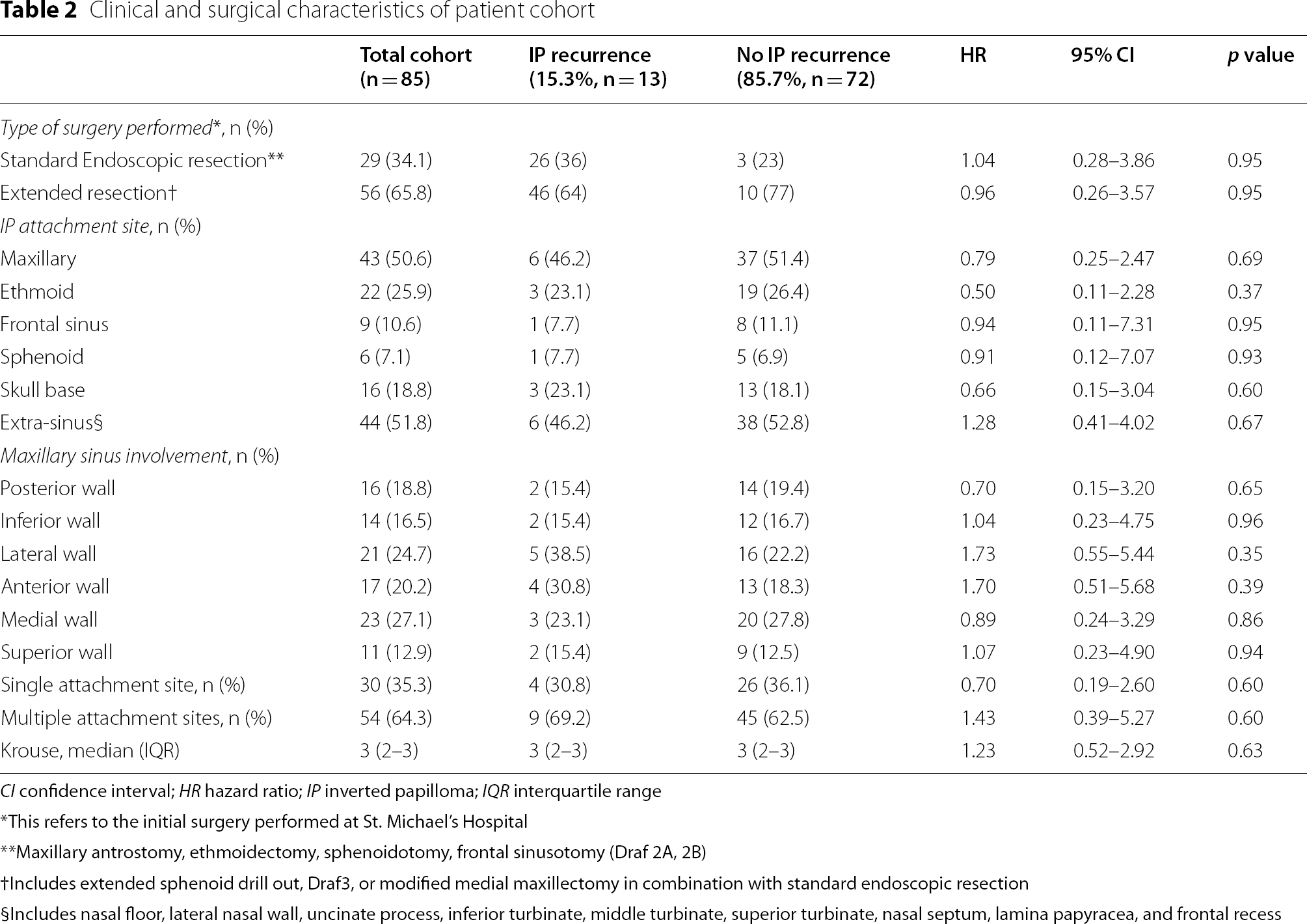
CI confidence interval; HR hazard ratio; IP inverted papilloma; IQR interquartile range
*This refers to the initial surgery performed at St. Michael's Hospital
**Maxillary antrostomy, ethmoidectomy, sphenoidotomy, frontal sinusotomy (Draf 2A, 2B)
†Includes extended sphenoid drill out, Draf3, or modified medial maxillectomy in combination with standard endoscopic resection
§Includes nasal floor, lateral nasal wall, uncinate process, inferior turbinate, middle turbinate, superior turbinate, nasal septum, lamina papyracea, and frontal recess
Recurrence free survival analysis
Of the 85 patients who underwent endoscopic endonasal resection, the overall recurrence rate was 15.3% (13/85). The median time to recurrence was 22.0 months (IQR: 10.4 to 52.6). The probability of remaining free of recurrence at 1, 3, and 5 years was 95.5% (SD: 2.6%), 87.4% (SD: 4.6%), and 75.1% (SD: 6.9%), respectively (Fig. 1).

Kaplan–Meier curve for time to recurrence for patients with inverted papilloma
Recurrence and primary tumour location
Attachment of primary tumour
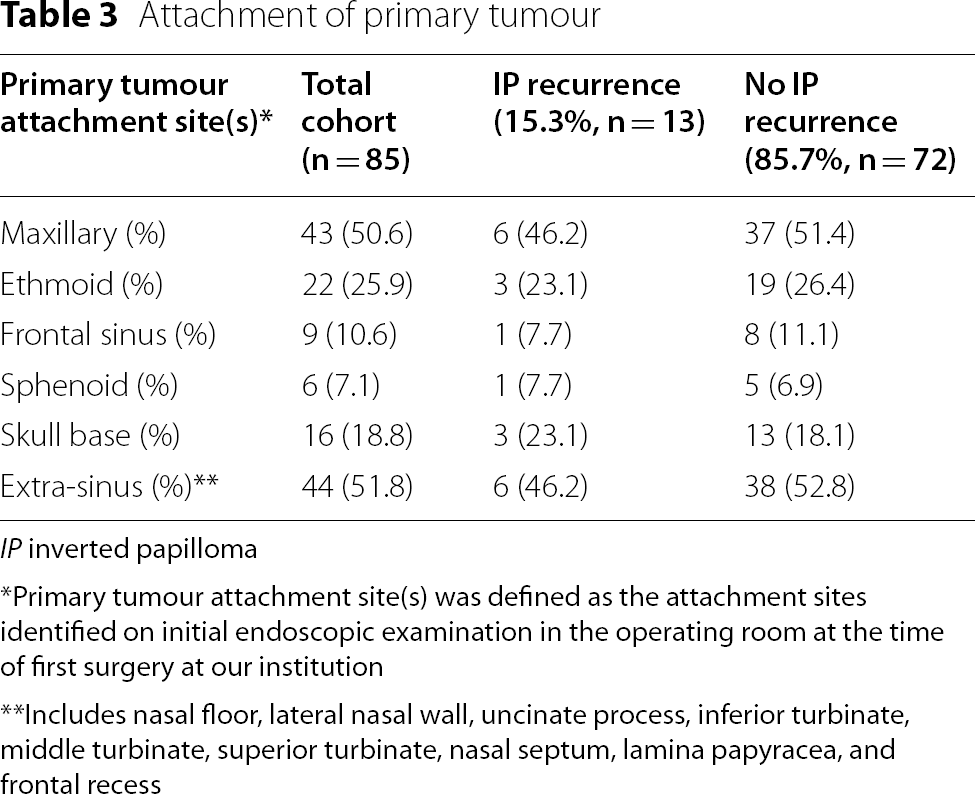
IP inverted papilloma
*Primary tumour attachment site(s) was defined as the attachment sites identified on initial endoscopic examination in the operating room at the time of first surgery at our institution
**Includes nasal floor, lateral nasal wall, uncinate process, inferior turbinate, middle turbinate, superior turbinate, nasal septum, lamina papyracea, and frontal recess
Postoperative SNOT-22 outcomes following endoscopic endonasal resection
In the overall cohort, there was a significant decrease in median postoperative SNOT-22 score when compared to preoperative SNOT-22 scores of 13.0 points (IQR: − 40.0 to − 3.5; p = 0.001) at 3 months, 18.3 points (IQR: − 37.7 to − 7.0; p < 0.001) at 6 months, and 12.0 points (IQR: − 36.0 to − 4.0; p = 0.002) at one year.
Figure 2 illustrates the median preoperative and postoperative SNOT-22 scores. There was no difference in SNOT-22 scores between the recurrence and the non-recurrence groups both preoperatively and at 1, 3 and 6 months postoperatively. Among the recurrence cohort, there was no significant increase in the SNOT-22 scores at the time when recurrence was detected when compared to postoperative scores.

Postoperative changes in SNOT-22 scores. The dark grey bars represent preoperative SNOT-22 scores. The white bars represent the SNOT-22 scores at 3 months postoperatively. The light grey bars represent the SNOT-22 scores at 6 months postoperatively. The black bars represent the SNOT-22 scores at 12 months postoperatively. The dashed bar represents the SNOT-22 score at the time of IP recurrence. *p < 0.05. IP = inverted papilloma; SNOT-22 = 22-item Sino-Nasal Outcome Test
Discussion
It is well established that sinonasal IPs have a high propensity for recurrence, with cited rates of 13–35% [9, 13–15]. Endoscopic surgical management of IPs has become the cornerstone of treatment for these patients due to advances in endoscopic tools and techniques. In fact, the endoscopic approach offers comparable outcomes with less morbidity when compared to external approaches [22]. Thus, the aim of the current retrospective review was to further evaluate recurrence rates, factors associated with recurrence, and quality of life outcomes for patients with IP who underwent endoscopic management at a high-volume Canadian tertiary care centre.
In this study, 15.3% of cases were found to have recurrent disease during a mean follow-up time of 36.4 months, with the median time to recurrence being 22.0 months. A recent meta-analysis of 23 studies including a total of 2451 patients reported a recurrence rate ranging from 1 to 30% for patients undergoing endoscopic resection of IPs during a follow-up time ranging from 14 to 55.5 months which demonstrates the heterogeneity in the existing literature regarding the recurrence rates of IPs [13]. Multiple factors can influence the reported recurrence rates in these studies including the length of follow up time, surgical technique, and the different types of IPs [19, 22, 23]. Our study found that the probability of remaining free of recurrence decreases with increasing length of follow-up. This finding is concordant with the existing literature which reports greater rates of recurrence beyond 3–5 years of follow up, with late recurrences occurring up to 15 years after primary resection [24–26]. The patient population in the current study is unique in that it included all locations of IPs in addition to a large proportion of patients (43.5%) who had prior sinus surgery, which is well documented as a risk factor for recurrent disease [8, 18]. This association is thought to result from incomplete resection, distortion of anatomy from previous surgery, scarring, or spread of disease to other locations in the case of misdiagnosed IP for nasal polyps [27, 28]. Thus, the results of this study may be more representative of the recurrence rates expected in a tertiary care referral centre given the large number of patients who have undergone previous surgeries.
Although there is a large body of literature describing risk factors for inverted papilloma recurrence, the results of these studies are conflicting and still debated [14]. In this study, site of tumour attachment and having multiple attachment sites were not associated with a higher rate of recurrence. Attachment of IP to the frontal sinus is a commonly reported association with increased recurrence rates of IP due to the technical difficulty of accessing the frontal sinus, limited visualisation via endoscopy, and difficulty obtaining a margin when up against critical structures [29]. Statistically significant recurrence rates up to 27.3% have been reported [16, 17, 29]. In contrast, our study found only 7.7% of recurrent cases to have had a primary tumour attachment site at the frontal sinus compared with non-recurrent cases which had a frontal sinus origin of 11.1%. This may be due to the usage of advanced frontal sinus techniques, such as Draf III procedures. In fact, there is emerging evidence that Draf III procedures in the context of IPs based in the frontal sinus or recess may reduce recurrence rates in addition to preventing external scarring and frontal outflow tract obstruction [30]. Similarly, maxillary sinus origin of IPs also have a reported association with increased IP recurrence due to more challenging visualisation and access of the anterior, medial and inferior maxillary sinus walls via transnasal endoscopic approach [17, 31, 32]. Although our study had a substantial amount of anterior, medial and inferior maxillary wall involvement (30.8%, 23.1% and 15.4%, respectively) amongst recurrent cases, we did not observe a significant association with IP recurrence and the location of maxillary sinus wall. Furthermore, in this study, 69% of patients who had recurrence and 63% of patients with no recurrence had multiple sites of attachment. Having multiple sites of attachment was not significantly associated with recurrence. In contrast, other large studies have found that having multiple sites of tumour attachment is significantly associated with recurrence [33]. The association between recurrence and multifocal disease is an area which certainly deserves further investigation as it is possible that complete resection would be made more challenging when multiple sites of attachment exist.
To further evaluate factors associated with recurrence, the IP tumour staging system proposed by Krouse et al. [5] was selected for statistical analysis in this study. Existing studies have shown inconsistent evidence on whether increasing Krouse tumour staging is associated with IP recurrence [12, 34–36]. Similarly, in the current study, increased Krouse stage was not found to be associated with recurrence. The Krouse staging system is determined by the extent of tumour periphery, which is less clinically meaningful than staging that the tumour attachment [14]. Tumours involving different paranasal sinuses may also be grouped into the same stage when they have variable associations with recurrence [8, 16–19, 31].
There is limited literature on the quality of life outcomes for patients undergoing endoscopic removal of IPs as many studies group all sinonasal and skull base tumours [37, 38]. van Samkar and Georgalas performed a study on the long-term quality of life outcomes in patients who underwent endoscopic removal of IP [39]. In a population of 27 patients, they found a postoperative SNOT-22 of 12.0 points during a median follow-up of 6 years, which was comparable with the average of 9.3 points reported by healthy people on SNOT-22 [39, 40]. Similarly, Bertazzoni et al. reported a mean postoperative SNOT-22 score of 5.3 points during a mean follow-up period of 66.3 months in 59 patients who had extended endoscopic maxillectomy for IP [41]. While both studies cite favourable postoperative SNOT-22 scores following endoscopic endonasal resection, no comparison was made with baseline preoperative SNOT-22 [39, 41]. More recently, Lin et al. reported no statistically significant improvements in SNOT-22 scores after endoscopic prelacrimal recess approach in 21 patients, although a downtrend was seen [42]. Our study found a statistically significant median decrease in SNOT-22 of 13 points at 3 months, 18 points at 6 months, and 12 points at one year. This demonstrates that undergoing endoscopic resection of IP does not predispose patients to subsequent symptoms of chronic rhinosinusitis and has benefit with respect to disease specific quality of life. Furthermore, this study demonstrated that there was no increase in SNOT-22 scores at the time of recurrence when compared to SNOT-22 scores after their initial resection. This was further validated by the fact that only 3 of the patients who recurred re-presented with sinonasal symptoms. To our knowledge, this is one of the first papers to investigate the change in sinonasal symptoms at the time IP recurrence is detected. The lack of change in symptoms in the majority of patients prior to recurrence further necessitates the need for long term follow up and serial endoscopic clinical examination to monitor for recurrence.
Limitations
This study has several limitations. Firstly, it is a retrospective, single-centre study which limits the generalizability of the results. In addition, 37 patients in this cohort had undergone endoscopic endonasal resection at other institutions prior to receiving care at our institution, which could have impacted surgical difficulty, rate of recurrence, and length of time to recurrence. Although we aimed to capture long-term data on IP recurrence within our cohort and had a mean follow-up of 36.4 months, this may not have adequately captured all cases of recurrence, as literature has suggested follow-up of at least 5 years [43]. Furthermore, there is a large degree of variability in our follow up period given that 33% of our patient population was operated on from 2017 and later. However, there was only one patient in our study who was lost to follow up. Finally, the SNOT-22 provides a relatively comprehensive assessment of sinonasal outcomes in chronic rhinosinusitis patients but is not currently validated in the IP population despite wide use in rhinologic literature [44]. The potential that this instrument fails to completely capture important and relevant symptomatology related to IPs must be considered.
Conclusion
In patients with IP who have undergone endoscopic surgical resection, this study found a recurrence rate of 15.3% with a median time to recurrence of 22.0 months. No demographic, surgical, or tumour variables were significantly associated with IP recurrence. These results suggest that endoscopic endonasal resection of IPs is an effective surgical approach despite potential surgical challenges associated with visualisation and access. However, the propensity for IPs to recur necessitates long-term follow up. To our knowledge, this is one of the largest single centre, single surgeon studies within recent years [14, 31, 34]. Completion of all surgeries at one institution by a single experienced senior surgeon reduces heterogeneity that may arise from varying surgical technique and institutional protocols to better elucidate the natural history of IP recurrence.
Footnotes
Acknowledgements
This study was presented as a poster presentation at the Canadian Society of Otolaryngology – Head and Neck Surgery annual meeting in Vancouver, British Columbia, 2022.
Author contributions
VW, EG and JML were involved in the conception of the study. SY, EG, DJL, VW and JML were involved in the design of the study, analysis, and interpretation of data. All authors were involved with the revision of the manuscript and have approved the final manuscript.
Funding
This study received no funding.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Abbreviations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Sheila Yu and Elysia Grose have contributed equally to this work and thus share co-first author