
Abstract
Background
Surgery is often indicated in the treatment of medically recalcitrant chronic rhinosinusitis (CRS). There is conflicting evidence on the impact of timeliness of sinus surgery on the degree of perceived symptom improvement in CRS.
Objective
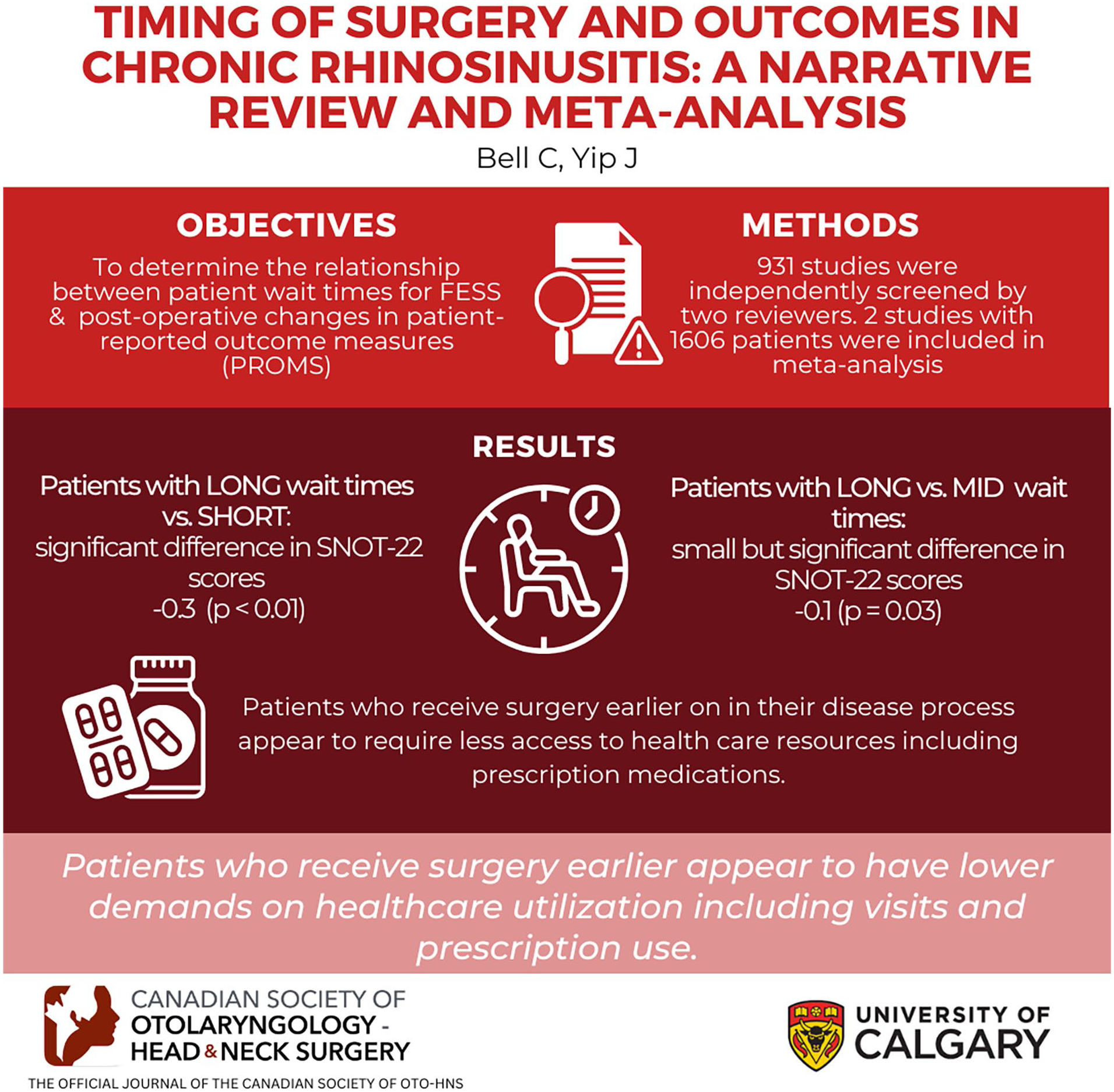
The goal of this study was to systematically evaluate the available literature on the relationship between patient wait times for endoscopic sinus surgery (ESS) and postoperative changes in patient-reported outcome measures.
Methods
Ovid, MEDLINE, CINAHL, and Cochrane Library of Systematic Reviews between January 2000 and September 1, 2023, were searched. A total of 931 studies were independently screened by 2 reviewers. Two studies were included in the meta-analysis, while 4 others were included in a narrative review.
Results
Two studies consisting of 1606 patients were included in the meta-analysis. A mean difference in 22-Item Sino-Nasal Outcome Test (SNOT-22) of −0.3 (95% CI = −3.9 to 3.3, I2 = 89%, P < .01 was observed between “long” and “short” groups, while a mean difference in SNOT-22 of −0.1 (95% CI = −2.5 to 2.3, I2 = 80%, P = .03) was observed between “long” and “mid” groups. Patients who receive surgery earlier on their disease process (ie, earlier from the time of diagnosis to eventual surgery) appear to require less access to healthcare resources including prescription medications, thus suggesting better disease control.
Conclusion
There is conflicting evidence to conclude whether timing of ESS affects disease-specific measures in patients with CRS. Patients who receive surgery earlier appear to have lower demands on healthcare utilization including visits and prescription use. Our study suggests there is a need for increased access to surgical specialists who manage patients with CRS, and better understanding by primary care specialists in how to manage CRS when specialist access is not available.
Keywords
Introduction
Surgery is often indicated in the treatment of medically recalcitrant chronic rhinosinusitis (CRS). The goal of surgery is not to cure patients of their disease, but rather to reduce the inflammatory load and create a “neo-cavity” through which topical medical therapies may exert greater efficacy. 1 Previous UK-based research has demonstrated that CRS patients who experience delayed access to surgery had higher rates of postoperative specialist visits, increased frequency of emergency visits related to CRS, number of prescriptions, and utilization of corticosteroids and antibiotics when compared to patients with a shorter duration from diagnosis to surgery. 2 Moreover, Benninger et al 3 reported higher rates of medication use and medical visits to outpatient clinics in patients who experience longer delays from diagnosis to surgery. In addition to increased healthcare utilization and direct medical costs, Smith et al4,5 suggested that patients with CRS who experience delayed access to appropriate therapy, such as surgery, often report worse quality of life outcomes.
The use of patient-reported outcome measures (PROMs) in CRS can help assess response to treatment, perceived symptom scores, health-related quality of life, overall quality of life, and disease-specific control. 6 Commonly-used PROMs, such as the 22-Item Sino-Nasal Outcome Test (SNOT-22) 7 and EuroQoL 5-Dimension Questionnaire (EQ-5D), 8 have been demonstrated as valid means of longitudinally assessing patient symptom severity and response to treatment. As it relates to surgical timeliness, few studies have assessed the relationship between surgical wait times and PROMs in CRS.
Previous attempts at understanding the relationship between surgical wait and patient outcomes appear to have conflicting results.9,10 Due to limited healthcare resources and access to surgical treatment, understanding the impact of surgical wait times may help manage patient expectations, allow for better patient-centered care, and improve physician advocacy for specific patient populations at systems level. Ultimately, this could help inform the development of quality indicators for the timing of endoscopic sinus surgery (ESS). Therefore, the goal of this study is to systemically summarize the currently available literature on the relationship between surgical wait times and PROMs in patients with medically recalcitrant CRS.
Methods
The systematic review and meta-analysis was conducted in accordance with the standardized reporting methods for both systematic reviews and meta-analyses [Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)]. 11 It was registered and published with the Prospective Register of Systematic Reviews (PROSPERO, CRD42022351722) prior to developing and implementing the database search strategy. Because of the nature of the study, Institutional Review Board approval was not sought.
Data and Search Strategy
In consultation with a postsecondary education-level librarian specializing in systematic reviews and database search strategies, a search strategy utilizing known common keywords, subject headings, and synonyms from previously published works was developed and implemented. Four electronic databases, including the Cochrane Library of Systematic Reviews, Ovid, MEDLINE, and CINAHL, were utilized. All databases were searched simultaneously and sequentially from January 2000 to September 1, 2023.
Eligibility Criteria
Studies were included in screening and subsequent analysis if they were original research articles published in English and conducted on adult patients (18 years of age or older) with CRS who were determined to have failed appropriate medical therapy (AMT) and subsequently underwent primary or revision ESS. Moreover, surgical wait time (ie, time from diagnosis of CRS to surgery, or time of decision for ESS to surgery) and a PROM (eg, SNOT-22, visual analog scale, EQ-5D) must have also been reported. Studies were excluded if the study population consisted of patients with CRS secondary to another condition (eg, primary ciliary dyskinesia, cystic fibrosis, immunodeficiency, vasculitis, or with odontogenic sinusitis) as these were considered distinct disease processes.
Study Selection and Data Extraction
Covidence, a third-party online tool for conducting systematic reviews was used to assist with study screening, selection, and initial data management. 12 All article abstracts were independently screened by both authors (CMB and JY) prior to full article review. Any disagreements in independent screening were remedied through discussion and mutual agreement was reached before proceeding further. An identical process was carried out for full-text review and data extraction. Extraction of data was performed by both authors after screening of all studies was performed. Data of interest were recorded in a separate Excel spreadsheet which was then used for statistical analysis. After screening all studies for narrative review and meta-analysis, Cohen’s kappa coefficient was calculated to measure inter-rater agreement. Studies that met initial inclusion criteria for full-text screening but not inclusion for the meta-analysis were included in the narrative analysis to aid in study production and power.
Risk of Bias Assessment
The Risk of Bias In Non-Randomized Studies—of Interventions (ROBINS-I; 2016) tool for assessing nonrandomized studies of interventions was used to perform an assessment of bias based on 7 domains. 13 Both authors independently graded each study as “low,” “moderate,” “severe,” or “no information” in each of the 7 domains, as well as an overall rating of risk of bias. A consensus for each domain, in the event of a disagreement, was made prior to establishing a final rating.
Statistical Analysis
Analysis of all data was performed by an independent PhD-level statistician through the Department of Surgery Office of Surgical Research, Cumming School of Medicine at the University of Calgary. Statistical analyses were conducted using R (Version 4.2.2; The R Foundation). When appropriate, data were pooled and evaluated using a fixed effects model for the meta-analysis. We compared previously defined time points from diagnosis of CRS to surgery: “short” (<1 year), “mid” (≥1 year but <5 years), and “long” (≥5 years).2,14,15 All SNOT-22 values were taken at 1 year postsurgery as this was the only common time point throughout the studies. Heterogeneity between studies was quantified using I 2 . A 95% confidence interval was used to report estimates, and an alpha of .05 was determined to be the threshold for statistical significance. When reporting results, mean difference in SNOT-22 was calculated. As an illustrative example, when “long” and “short” mean SNOT-22 scores are compared, if “long” minus “short” is greater than 0, “long’ has a greater change in SNOT-22 score favoring later surgery; however, if “long” minus “short” is less than 0, “long” has a lesser change in SNOT-22 score, favoring earlier surgery. This same principle was used when comparing “long” and “mid” SNOT-22 scores.
Results
A total of 931 studies were extracted from the databases of interest. After removing duplications, 814 studies were screened by title and abstract. A total of 807 studies were excluded, and a total of 7 studies were assessed for eligibility by full-text review for inclusion in the meta-analysis.2,3,9,10,14-16 Of the 7 studies, 5 were excluded based on: wrong outcomes (3/7) for Hopkins et al, 2 Newton et al, 9 and Yip et al, 10 wrong comparator (1/7) for Benninger et al, 3 and wrong intervention (ie, middle turbinate resection) (1/7) for Scangas et al, 16 leaving 2 studies to be included in the meta-analysis. Cohen’s kappa coefficient was calculated to be 0.87, indicating a high degree of agreement between raters. The 4 studies were included in further narrative review, but not meta-analysis included: Hopkins et al, 2 who retrospectively assessed a total of 2534 cohort-matched patients with CRS and healthcare utilization based on timing of ESS; Benninger et al, 3 who assessed a total of 2833 patients with CRS and evaluated healthcare utilization based on timing of ESS; Newton et al, 9 who assessed 150 patients with CRS undergoing primary ESS, but did not use the same definition of timing; and Yip et al, 10 who assessed 104 patients with CRS undergoing primary ESS, but did not have long enough follow-up to be included. One final study not included in either the meta-analysis or systematic review was a study by Scangas et al, 16 who only assessed timing of middle turbinate resection (Figure 1; Table 1).

PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summary of Studies Included in Meta-Analysis.

Abbreviations: BSIT, Brief Smell Identification Test; CRS, chronic rhinosinusitis; RSDI, Rhinosinusitis Disability Index; SNOT-22, 22-Item Sino-Nasal Outcome Test.
Two studies were included in the meta-analysis.14,15 A total of 1606 patients were followed prospectively from time of diagnosis of CRS to ESS. Both studies determined total duration of symptoms based on patient recall and all patients underwent primary ESS. Subjective and objective outcomes collected varied between studies including SNOT-22, Rhinosinusitis Disability Index, Lund-Kennedy endoscopy score, Lund-Mackay score, and Brief Smell Identification Test (Table 1).
The ROBINS-I tool was used to evaluate those studies included in the meta-analysis for risk of bias. 13 Based on both authors’ independent evaluations, bias due to confounding variables received a “moderate” risk rating, while all other criteria received a grading of “low” risk. The overall rating for risk of bias was “low-to-moderate” (Table 2).
The ROBINS-I Tool for Risk of Bias in Non-Randomized Studies of Interventions.

Abbreviation: ROBINS-I, Risk of Bias In Non-Randomized Studies—of Interventions.
The 2 studies included in this meta-analysis captured a total of 798 patients. Specifically, 599 patients were included in the “long group,” while 199 patients were included in the “short group.” Alt et al 15 captured a total of 55 patients with a mean difference in SNOT-22 between “long” and “short” groups of 12.9 (95% CI = 3.6-22.2). Meanwhile Hopkins et al 14 captured a total of 743 patients, and there was the mean difference in SNOT-22 between “long” and “short” groups was −2.7 (95% CI = −6.6 to 1.2). Combining both studies provided a mean difference in SNOT-22 of −0.3 (95% CI = −3.9 to 3.3, I 2 = 89%, P < .01). Based on the 95% CI line, there was no statistical difference between groups.
The 2 studies captured a total of 1372 patients, with 599 patients included in the “long group” and 773 patients in the “mid group.” Alt et al 15 captured a total of 51 patients with a mean difference in SNOT-22 between “long” and “mid” groups of 12.8 (95% CI = 1.2-24.4). Hopkins et al 14 captured a total of 1321 patients and had a mean difference in SNOT-22 of −0.7 (95% CI = −3.2 to 1.8). Combining both studies provided a mean difference in SNOT-22 of −0.1 (95% CI = −2.5 to 2.3, I 2 = 80%, P = .03). Based on the 95% CI line, there was no statistical difference between groups.
Discussion
Surgical Timing and Change in SNOT-22 Score
Our meta-analysis is the first of its kind to summarize the available data on the impact of wait times for primary ESS on patient reported outcomes; specifically, SNOT-22. The mean difference in SNOT-22 scores between the 2 comparison groups did not favor earlier or later surgery (Figures 2 and 3), as the observed differences in mean SNOT-22 scores were also very small. This is important to note, as the minimal clinically important difference for SNOT-22 score is 8.9,7,17 which our calculated mean difference did not meet in either meta-analysis. These results also should be interpreted with caution as postoperative follow-up data were only available in 69% and 78% of patients in the study of Alt et al and Hopkins et al, respectively, and it is unclear how this selection bias may have affected validity of findings.

Meta-analysis of mean difference in change in SNOT-22 between “long” versus “short” groups. SNOT-22, 22-Item Sino-Nasal Outcome Test.
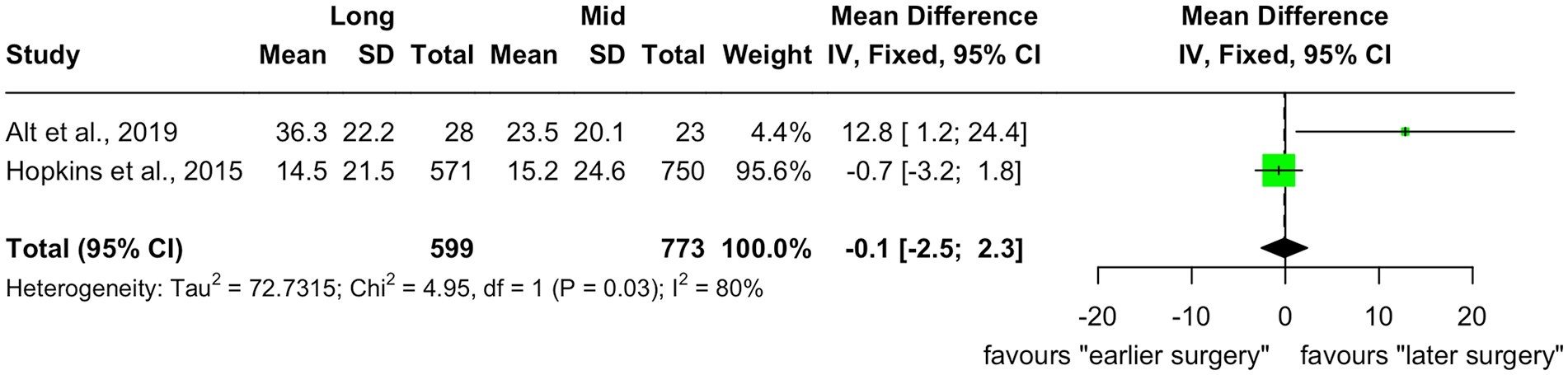
Meta-analysis of mean difference in change in SNOT-22 between “long” versus “mid” groups. SNOT-22, 22-Item Sino-Nasal Outcome Test.
While we could only include 2 studies in our meta-analysis, a thorough evaluation of studies included in our full-text review were reviewed in a systematic fashion. The studies not included in the meta-analysis captured a total of 5617 patients from countries including the United States, 3 Canada,9,10 and the United Kingdom, 2 all of which have different healthcare coverage and accessibility of services. Between these studies, the definition of timing varied in that Yip et al 10 assessed patients based on time from surgical consent to the date of surgery, while Benninger et al and Newton et al utilized time from first symptom onset to surgery 3 and time from incomplete symptoms improvement despite AMT to surgery, 9 respectively. Hopkins et al’s retrospective study 2 did not deviate from the prospective definition. 14 Of the 2 studies not included in the meta-analysis that assess wait times and changes mean SNOT-22 scores, surgical wait times varied from an average of 310.8 ± 155.910 to 1684.9 days. 9
Yip et al 10 found a significant negative correlation between both SNOT-22 aggregate, rhinologic, extranasal rhinologic, and ear/facial subdomains, while no correlation was noted between wait times and psychological or sleep subdomains suggesting that in a publicly-applied healthcare system, longer patient waits for ESS lead to less improvements in disease-specific quality of life. In contrast, Newton et al’s 9 linear regression model found that wait times for surgery was not significantly associated with their wait time after adjusting for potential confounders; however, they do indicate that patients with higher SNOT-22 scores preoperatively, based on quartile ranking, do experience greater change in postoperative SNOT-22 (−36.8% for the lowest quintile vs −45.2% change highest quintile). Newton et al argue that while their study contrasts with other studies of similar nature, it may indicate that patients under the care of an otolaryngologist may experience stabilization in their symptoms as an explanation for this conflicting observation. It also appears that patients with more poorly controlled disease preoperatively experience greater benefit postoperatively regardless of wait time to surgery. 9
In all, the lack of consensus may be due to varying definitions of wait times utilized. It may also reflect that surgical wait times is a poor surrogate marker for “delayed surgical intervention” and that a better measure could be duration of symptomatic disease. 16 Finally, extent of surgery was not consistently measured across studies, and it is unclear whether surgical philosophies were influenced by symptom duration and/or wait times.
Surgical Timing and Healthcare Utilization
While PROMs serve as a means of evaluating a patient’s response to surgery, this is but only 1 way to determine which groups of patients experience a benefit from earlier or later surgery. Two studies by Hopkins and Benninger have also evaluated timing of ESS and healthcare utilization.2,3 The 2 Hopkins studies used the same definitions for time to surgery, while Benninger used more narrow time frames from diagnosis to surgery which included 6 groups in total: group 1 (<1 year), group 2 (1 to <2 years), group 3 (2 to <3 years), group 4 (3 to <4 years), group 5 (4 to <5 years), and group 6 (5 years or more). Despite subtle distinctions between groups based on duration of symptoms, both Hopkins and Benninger clearly show that patients with longer duration of symptoms before undergoing ESS are more likely to have higher rates of healthcare utilization, including hospital visits related to their disease, and nearly all prescription medications including antibiotics, corticosteroids, antihistamines, and pain management (except for leukotriene modifiers) use related to their disease.2,3 This observation is also more common in patients with comorbid asthma compared to those without asthma2,3 in a relatively stepwise fashion year over year. These observations are also reflected in the prospective Hopkins study. 14 Moreover, this effect seems to carry over even after having undergone ESS, suggesting that patients may benefit from earlier surgery.
Study Limitations
The meta-analysis was limited as there was significant variation in the definition of wait time and PROMs across studies, thereby making direct comparison and inclusion of more studies not possible; moreover, of those studies we were able to include in our meta-analysis, a large proportion of the total population of patients came from 1 study, thus creating a risk of bias. The degree of heterogeneity between studies and small overall study size also limits our ability to draw strong conclusions. Finally, many confounding factors, such as socioeconomic status, barriers to care, and tissue remodeling, were not measured and may have had an impact on observations across studies.
Conclusion
There appears to be conflicting evidence, based on limited similar studies, to conclude whether timing of ESS affects disease-specific quality of life in patients with CRS. Certainly, however, the best available literature suggests that patients who receive surgery earlier appear to have lower demands on healthcare utilization including healthcare visits and prescription use. When timely access to surgery is not possible due to systemic bottlenecks in a healthcare system, easier access to appropriate specialists may also assist in improved disease control and less healthcare resource utilization. Because of this, understanding of disease processes by primary care physicians may lead to better disease control and less burden on surgical specialists and healthcare systems. Our study highlights an ongoing and significant gap in highly relevant research which ought to be explored further.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Golpira Elmi Assadzadeh (PhD) in the Department of Surgery Office of Surgical Research through the Cumming School of Medicine, University of Calgary for her help with statistics. The authors would also like to acknowledge Caitlin McClurg of the Health Sciences Library at the University of Calgary for her assistance with database searches.
Author Contributions
CMB and JY were involved in all aspects of study preparation including rationale, methodology, data analysis, and manuscript preparation.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Consent for Publication
All study authors express full consent for this article to be considered for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was exempt from ethics approval based on methodology and publicly available data.