
Abstract
Oral Submucous fibrosis (OSMF) has traditionally been described as “a chronic, insidious, scarring disease of the oral cavity, often with involvement of the pharynx and the upper esophagus”. Millions of individuals are affected, especially in South and South East Asian countries. The main risk factor is areca nut chewing. Due to its high morbidity and high malignant transformation rate, constant efforts have been made to develop effective management. Despite this, there have been no significant improvements in prognosis for decades. This expert opinion paper updates the literature and provides a critique of diagnostic and therapeutic pitfalls common in developing countries and of deficiencies in management. An inter-professional model is proposed to avoid these pitfalls and to reduce these deficiencies.
Introduction
Oral Submucous Fibrosis (OSMF) is a potentially malignant disorder which was described by Schwartz in 1952 as “Atropica idiopathica mucosae oris” and later by Jens J. Pindborg in 1966 as “an insidious, chronic disease that affects any part of the oral cavity and sometimes the pharynx [1]. Although occasionally preceded by, or associated with, the formation of vesicles, it is always associated with a juxtaepithelial inflammatory reaction followed by fibroelastic change of the lamina propria and epithelial atrophy that leads to stiffness of the oral mucosa and causes trismus and an inability to eat” [1]. OSMF is also characterized by reduced movement and depapillation of the tongue, blanching and leathery texture of the oral mucosa, progressive reduction of mouth opening, and shrunken uvula [2–4]. Other terms used to describe OSMF include idiopathic scleroderma of the mouth, juxtaepithelial fibrosis, idiopathic palatal fibrosis, diffuse oral submucous fibrosis, and sclerosing stomatitis [5–8].
Epidemiology (Table 1) (Fig. 1)
Worldwide prevalence studies on Oral Submucous Fibrosis


Global and Indian prevalence studies of Oral Submucous Fibrosis
Table 1 and Fig. 1 present published estimates of the prevalence of OSMF, which range from 0.1 to 30%, varying by geographical location, sample size, and sampling methodology. There is an urgent need for large well-designed epidemiological surveys to understand the true global and regional burden of OSMF.
Major etiology, contributing factors and etiopathogenesis (Tables 2 and 3) (Fig. 2)
Major aetiology of Oral Submucous Fibrosis

Contributing risk factors for Oral Submucous Fibrosis


Etiopathogenesis [44]
Diagnostic approach
Intra- and extra- oral manifestations of OSMF at different stages


Clinical expressions of Oral Submucous Fibrosis. Oral Submucous Fibrosis in a 27-year-old male with a history of gutkha chewing. Panel A shows sunken cheeks and prominent malar bone. Panel B shows significant blanching or marble-like appearance of the soft palate and faucial pillars. Note the altered, inverted shape of the uvula. Panels C & D show blanched bands of upper and lower labial mucosae and vestibule, which are stiff and palpable. Panels E, F & G: A 24-year-old female with a history of chewing baked areca nut. Panel E: significant blanching of soft palate and faucial pillars, and shrunken uvula. Panels F & G: thick fibrous bands and brown/black pigmentation on left & right buccal mucosae
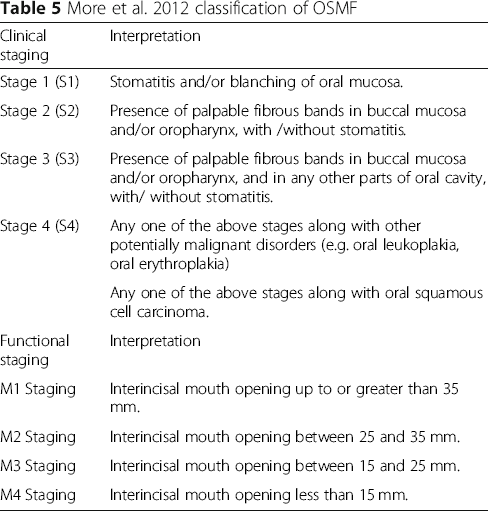
More et al. 2012 classification of OSMF
Approaches to non-surgical management
Treatments for OSMF

Malignant transformation of OSMF
OSMF is classified as an oral potentially malignant disorder (OPMD) [3]. Patients with OSMF have been reported with higher risk of developing oral squamous cell carcinoma (OSCC), compared to other OPMD's [71, 72]. Although 7.6% of OSMF cases transformed to oral squamous cell carcinoma (OSCC) in a 17-year follow up study reported in 1970 [73], other studies with smaller follow up periods report malignant transformation rates ranging from 1.9–9%, [74–76] depending on diagnostic criteria and duration of follow up [77].
Studies suggest that malignant transformation in patients with OSMF differs from those without OSMF. This difference is believed to arise from the mechanism of areca nut carcinogenesis. A retrospective study conducted in China reported that oral cancer originating from OSMF is clinically more invasive and exhibits higher metastasis and recurrence rates compared to “conventional” OSCC [78]. In contrast, Chaturvedi et al. found that OC arising in a background of OSMF represented a clinico-pathologically distinct entity, less aggressive than the “conventional” tobacco-related OC's seen in India [46]. Better prognostic features associated with OC occurring in a background of OSMF included early tumor stage, thinner lesions, fewer neck metastases with less extra-capsular spread, and more highly differentiated neoplasms. It was suggested that fibrosis in the oral mucosa and tumor stroma, with reduced vascularity, inhibits lymphatic and vascular spread [46].
Studies have shown higher risk of malignant transformation of OSMF when observed with simultaneous oral leukoplakia [77]. A wide array of studies was implemented recently to determine the possible mechanisms involved in malignant transformation, and many have focused their attention on molecular markers which could be helpful for early diagnosis and have possible, helpful therapeutic implications [79–81].
Proposed diagnostic and management approach
As with other lifestyle related diseases, primary prevention at population and individual levels needs to be improved. Space does not permit an exhaustive discussion of the approaches here but, in the case of OSMF, this involves education of the public regarding the dangers of areca nut and tobacco, and legislation to restrict the sale of gutkha and similar products [82–84]. Several Indian states have had success in this regard. Since May 2013, gutkha is banned in 24 states and 5 union territories of India, under the provision of centrally enacted Food Safety and Regulation (Prohibition) Act 2011 [85]. The ban is enforced by the State public health ministry, Food and Drug Administration and the local police. Although there is a significant reduction in the legal purchase of gutkha, the Supreme Court and higher enforcement bodies are still chasing to cease the illegal sale [85, 86].
What of the many millions already afflicted? Despite efforts to improve the management of OSMF, many come so late to diagnosis that cure is impossible, and interventions are of limited efficacy. So early diagnosis is of great importance. Further, most OSMF patients chew tobacco as well as an areca nut product, may imbibe unhealthy amounts of alcohol, and abuse other drugs. They often have dietary deficiencies. Therefore, they are at high risk of co-morbidities, including metabolic syndromes, respiratory, gastrointestinal/liver and cardiovascular diseases. (Fig. 4) [87, 88].

Oral and Systemic outcomes of OSMF possible in the absence of holistic management
Dependent on their dominant symptoms, patients may seek consultation from either primary care physicians (PCP) or dentists. When examined by a dentist, the diagnostic and treatment approach is likely to be focused on the oral signs and symptoms. Conversely, when patients present to a PCP, the focus of management is likely to be general, with the oral condition under-investigated and under-managed. In most of the world, these patients are not managed by a multidisciplinary team.
We propose an inter-professional approach that may increase rates of early diagnosis of OSMF and potentially malignant disorders/OSCC, with integrated management of both oral and systemic symptoms, improving long-term prognosis, reducing suffering and improving quality of life.
When a patient presents to a dentist, and a clinical diagnosis of OSMF is made, he/she should be referred to their primary care physician with a note of planned dental management. If any underlying systemic disease is diagnosed, the medical treatment plan should be communicated back to the dentist. If no systemic disease is diagnosed, a written medical clearance letter, including an assessment of risks of developing any systemic condition, and recommendations for review visits, should be included.
When a patient presents to a physician, if he/she is a user of areca nut, and especially if restricted mouth opening is present, he/she should be immediately referred to a dentist detailing any planned management of other disease. The dentist should report back to the physician with a treatment plan for OSMF, if present, or dental clearance letter with a suggested risk of developing OSMF or any other oral disease.
This, after all, should be routine in any integrated health care system.
Conclusion
Although studied intensively over many decades, one might say centuries, especially in South Asia, OSMF is hardly recognized and is poorly understood across the globe. The incidence is rising; there has been no significant improvement in management, nor reduction in its high malignant transformation rate.
Better integration of medical and dental services, especially in developing countries, may reduce patients’ suffering and improve their life quality. All health care professions must work together in public education and primary prevention.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
This manuscript arises out of discussions between the authors, both at international scientific meetings and in private. All have considerable experience of treating and researching Oral Submucous Fibrosis and similar disorders. The first draft was written by Naman Rao and revised with input from all other authors. All authors have approved the final version.
Funding
Not applicable.
Availability of data and materials
Not applicable.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.