
Abstract
Background
Our aim was to review our management of inverted papilloma (IP), perform a recurrence analysis, and review the literature.
Methods
A retrospective analysis of 247 patients treated for an IP. Patients were grouped according to surgical approach, tumor presentation (primary, residual and recurrence) and Krouse-stage.
Results
Recurrence was observed in 20.3%, 28.6% and 35.1% (p = 0.017) of the patients who underwent endoscopic, external and combined surgery, respectively. Recurrences occurred more often in residual than primary IP (36.9% vs. 22.3%, p = 0.021). Primary endoscopic surgery had a recurrence rate of 12.5%, which was comparable to the recent literature (11.2%, 161/1433).
Conclusions
The relatively high number of recurrences in this cohort is explained by the long follow-up and previous (incomplete) surgery in 61.5% of the cases. The inferior outcome of residual IP underscores the importance of having a low threshold for preoperative biopsy in unilateral and atypical sinonasal disease.
Background
Inverted papilloma (IP) is a benign tumor of the sinonasal cavities. It was first described by Ward more than 150 years ago as a follicular tumor involving the nasal bones [1]. It took until 1938 for Ringertz to recognize the characteristic endophytic growth pattern and introduce the term ‘inverting papilloma’ [2]. Since then many researchers have contributed to the extensive knowledge we now have on IP [3].
The incidence of IP ranges from 0.2 to 0.6 people diagnosed per 100,000 per year. The most frequently reported complaints are similar to those of sinonasal polyps: unilateral nasal obstruction and rhinorrhea. IP is most commonly diagnosed in the fifth and sixth decade of life and has a predilection for males with a ratio of 3:1 [4]. The exact etiology of IP is unclear, but there are indications that HPV infection plays a role in the progression of inverted papilloma and confers an increased risk for recurrence and malignant transformation [5, 6]. The frequency of IP in unsuspected sinonasal polyps is reported to be between 0.31 and 0.93% [7, 8].
The standard treatment has always been surgery aimed at complete removal of the tumor. Its association with malignancies in 5–15% is one of the distinct characteristics of IP that endorses surgical treatment [9]. Other important features include its aggressive growth, that causes adjacent bone to locally erode, and its tendency to recur. Over the last decades endoscopic surgery has become the gold standard for the treatment of IP with many studies showing significantly better treatment outcome in patients treated endoscopically [9].
The aim of this study was to analyze the developments in our management of IP over the last three decades, in particular with regard to the recurrence rates and outcomes of treatment. All surgical approaches were reviewed, with an emphasis on endoscopic surgery. Whether the presentation of the tumor (primary, residual or recurrent) before surgery in our clinic would affect the recurrence rate also had our interest. Finally, a literature review of IP cohort studies was performed to compare with our surgical outcomes and recurrence rates.
Methods
The Ethics Committee of the Erasmus Medical Center, a tertiary referral medical center, stated that ethical permission was not required for this retrospective study.
We included 323 IP patients, of which 247 were included in the recurrence analysis, between January 1983 and December 2012. All patients were obtained from PALGA, a Dutch nationwide network and registry of histo- and cytopathology. All cases received surgical treatment, had a preoperative histopathological proven diagnosis of IP, and complete clinical information. Clinical data was assessed using the electronic medical records (CSC-iSOFT, Virginia, USA) and paper charts.
The IP was classified as a primary when no prior surgery was performed and diagnosis was confirmed by a simple biopsy. Patients with previous surgery were divided into two groups: residual and recurrent IP. Residual IP were defined as those who underwent functional endoscopic surgery for reasons other than IP, which was deemed as inadequate tumor surgery. Inverted papilloma diagnosis is this group was unexpected at postoperative histopathological examination. Recurrent IP were defined as those who underwent adequate tumor surgery in a different, non-academic hospital with the preoperative suspicion or diagnosis of IP. These patients were referred to us for revision surgery after diagnosis of a recurrence.
Summary of Clavien-Dindo Classification of Surgical Complications

A literature search was performed of EMBASE (2005, jan – 2016, dec) using the key term ‘inverted papilloma’. All IP case series with a minimal follow-up of 12 months, reporting on recurrence rates per operative approach, and published in the English language were included.
Statistical analysis
When quantitative variables were normally distributed, the results were expressed as mean values and standard deviation (SD), otherwise median and inter quartile range (IQR). Differences between two groups were analyzed using the t-test or the Mann-Whitney U test. Qualitative data are reported as counts and frequencies, and differences between groups were analyzed using the chi-squared test or Fisher's exact test. Multivariate logistic regression was used to investigate the association of Krouse staging, surgical approach and presentation of tumor and the risk of recurrence [11]. Cox regression analysis was performed to evaluate the association between variables of the univariate analysis and recurrence free survival time. Statistical analysis was performed using SPSS version 21 (IBM Co., Armonk, NY, USA) and cut off point for significance was p < 0.05.
Results
The mean age at time of diagnosis was 55.8 years (SD 13.7). The study population consisted of 245 males and 78 females (3.1, 1). Nasal obstruction was the most frequent complaint (257 patients, 79.6%). Other complaints were rhinorrhea (73, 22.6%), headache (38, 11.8%), epiphora (21, 6.5%) and feeling of pressure in the face or forehead (17, 5.3%). Thirty patients (9.3%) had no complaints. Preoperative radiological imaging was performed with CT-scan in 201 cases (62.2%) and with MRI in 15 cases (4.6%). Both CT and MRI were used in 62 patients (19.2%). Forty-five patients (13.9%) underwent surgery without preoperative radiological imaging. The left and right side of the sinonasal cavity were equally involved (50.2% vs. 48.3%). Five patients (1.5%) had bilateral involvement.
In 121 of the cases (37.5%) the inverted papilloma was primary, in 115 cases (35.6%) residual, and in 87 cases (26.9%) recurrent. The tumors were classified as Krouse T1 to T4 in respectively 38 (11.8%), 148 (45.8%), 108 (33.4%) and 29 cases (9.0%). Twenty-eight IP were classified as T4 because of an associated malignancy and one because of extrasinonasal extension. Endoscopic surgery was performed in 107 patients (33.1%), a combined approach in 22 cases (6.8%) and an external procedure in 194 patients (60.1%).
Complications
The overall percentage of perioperative complications was 14.6% (47 cases). Most complications were Clavien-Dindo grade I (24, 51.1%), such as sensibility disorders, perioperatively managed cerebrospinal fluid leakage and excessive crustae. Ten patients (21.3%), including four wound infections, had grade II complications. Most Clavien-Dindo grade III complications (10, 21.3%) were complaints of epiphora after a classical Denker procedure that required a dacrocystorhinostomy. Two patients (4.3%, grade IV) developed meningitis post-operatively and had to be admitted to the intensive care unit. One patient died post-operatively as a result of severe comorbidity (2.1%, grade V).
Malignancies
Thirty-one patients (9.6%) had an associated malignancy. The malignancy occurred synchronously in 28 cases (90.3%). They consisted of 25 squamous cell carcinomas (89.3%), two verrucous carcinomas (7.2%), and one undifferentiated carcinoma (3.6%). Three other cases squamous cell carcinomas developed metachronously (9.7%).
Four patients (12.9%) had a carcinoma in situ. Nine patients had tumor with T stage I (29.0%) three with II (9.7%), three with III (9.7%) and 12 with IV (38.7%). Three patients (9.7%) had a regional lymph node metastasis and three patients (9.7%) a distant metastasis. Most patients (80.6%) with an associated malignancy were treated with an external approach. For patients with an associated malignancy, the 5-year overall survival was 80.6% and the 5-year disease specific survival 87.1%. Eight patients with an a associated malignancy (25.8%) developed a recurrent IP after initial treatment. The 5-year recurrence free survival rate was 77.4%. During follow-up 20 patients (64.5%) remained alive with no evidence of disease. One (3.2%) was alive with disease, eight (25.8%) died of disease, and two (6.5%) died of other cause.
Recurrence analysis
Multivariate analysis of recurrence rates according to surgical approach and presentation of the tumor
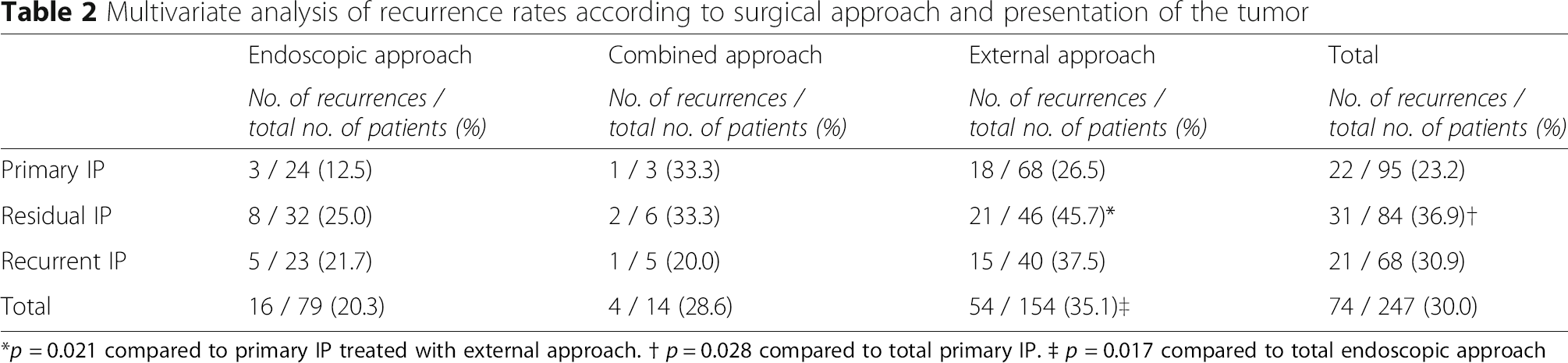
*p = 0.021 compared to primary IP treated with external approach. † p = 0.028 compared to total primary IP. ‡ p = 0.017 compared to total endoscopic approach
Type of surgery
Distribution of Krouse stage per surgical approach

Presentation of tumor
The risk of recurrence was significantly higher in the residual IP group than primary IP (31 [36.9%] vs 22 [23.2%], p = 0.021 OR 95% CI 2.2 [1.1–4.3]). Recurrence occurred in 21 cases (30.9%) in the recurrent IP group.
Krouse stage
Krouse stage did not influence the overall recurrence rate significantly. Patients with Krouse stage T1-T4 IP developed recurrences in respectively 7 (22.6%), 36 (30.5%), 25 (28.9%), and 6 (42.9%) cases.
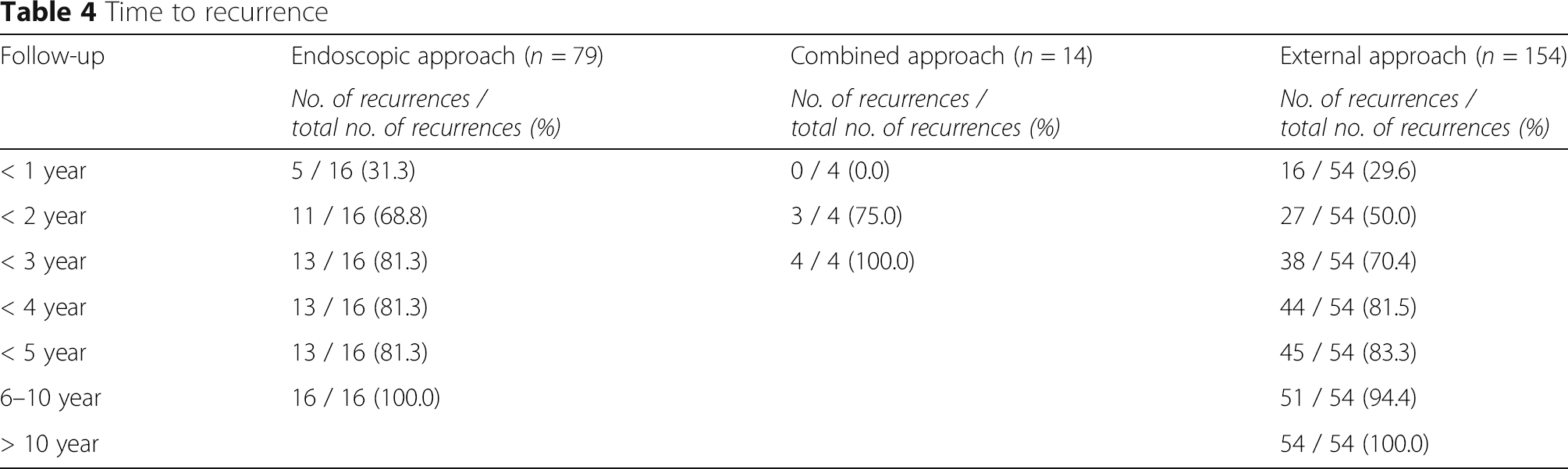
Time to recurrence
Time to recurrence
Number of recurrences
Thirty-seven (50%) of all 74 cases with a recurrence after initial surgery in our hospital developed a second recurrence after revision surgery. This occurred more often in the group of patients that underwent external surgery than the endoscopic group (5/16 [31.3%] vs. 32/54 [59.3%], p = 0.049). Eighteen patients (24.3%) developed a third recurrence, while six patients (8.1%) developed even more than three recurrences during follow-up.
Literature review
Review of inverted papilloma cohort studies per surgical approach with a minimal follow-up of 12 months (2005–2016)

Discussion
We have, to our knowledge, presented the largest ever single-center cohort of inverted papilloma patients. Our reported recurrence rates were higher for residual and recurrent IP than primary IP. We also confirmed superiority of endoscopic surgery over combined and external approaches. Finally, we've shown that many recurrences occur more than two years after initial treatment.
Thirty percent of all the patients in our recurrence analysis developed a recurrence (Table 2). This is relatively high compared to recent literature (Table 4). This could be explained by our heterogeneous cohort with a high number (62.3%) of external surgery. Also our rate is based on results covering a large time period with one third of the patients treated before the ‘endoscopic era’. These patients account for more than half of all recurrences. Based on our observation, most of the recurrences after an external approach, Denker in particular, occur in the frontal recess and ethmoidal roof. Tumor remnants at these areas can easily be missed or left out during such procedures due to lack of good visualization and magnification. Nowadays, we make it a point to inspect these areas using an endoscope and drill out as much bone as possible. Several literature reviews on IP recurrences have been published between 1981 and 2009 [9, 14, 35–37]. Their average recurrence rates after endoscopic surgery vary between 12.5% and 19.6%. This is higher than the 11.3% in our review of more recent studies, suggesting a global decrease in recurrence rates in endoscopic IP surgery.
Our recurrence in the endoscopic group (20.3%) was also higher than the average 11.2% (161/1433) in our review of the recent literature (Table 5). However, primary tumors treated by endoscopically had a similar recurrence rate of 12.5%. Therefore, we believe that the relatively high recurrence rate is due to our high number of residual and recurrent IP and to our long follow (median > six years). After splitting the complete endoscopic group in a 2003–2007 (the first years of endoscopic IP surgery in our clinic) and a 2008–2012 cohort, we also noted a non-significant learning curve is noticed with 31.8% and 15.4% recurrences (p = 0.12) respectively.
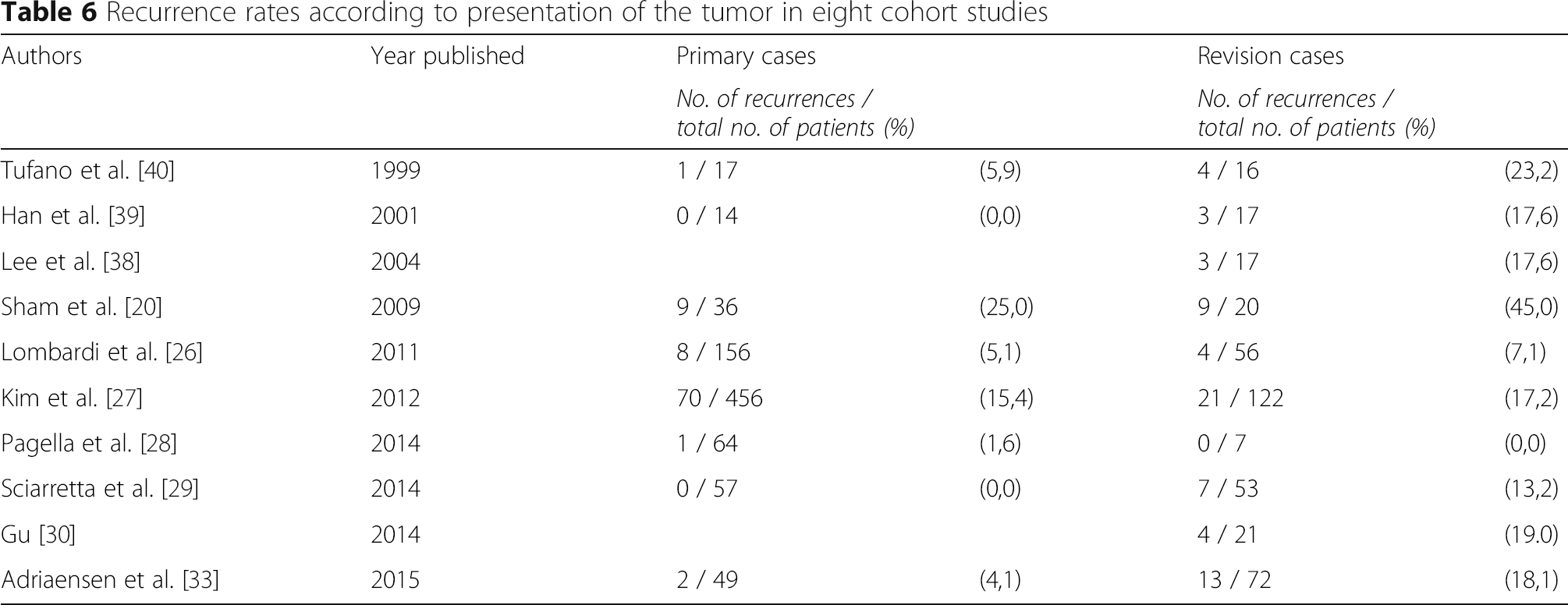
Recurrence rates according to presentation of the tumor in eight cohort studies
Many articles claim that the majority of recurrences after IP-surgery occur in the first two years [20, 43]. Sham et al. published a detailed data of time to recurrences of a group of 56 patients, which supported this statement [20]. This was however not the case in our larger cohort: only 55.4% of all recurrences occurred in the first two years (Table 4). This percentage was slightly higher (68.8%) in patient treated endoscopically. A follow-up of three years after endoscopic surgery and four years for all cases was needed to diagnose >80% of the recurrences. A multi-center study has also shown a significant difference in recurrence rate between patients with a follow-up longer and shorter than three years (26.1 vs. 8.5%) [27]. Therefore, our department supports suggestions by Suh and Adriaensen to perform a long or even life-time clinical follow-up [33, 43].
Conclusion
The recurrence rate of residual tumors is significantly higher than primary tumors. Therefore clinicians should have a low threshold for suspecting IP and when uncertain first take a biopsy. Furthermore, given the mean time to recurrence and the rate of late recurrences a long follow-up is required in both the clinic and research.
Footnotes
Acknowledgements
Authors’ contributions
OB, DM and JH contributed to study conception. All authors contributed to the study design. OB and FvZ performed the data collection. OB, FvZ, DM and JH or supervised data analysis. All authors interpreted the data. OB and DM wrote sections of the initial manuscript. OB designed figures and tables. All authors critically reviewed iterations of the manuscript and approved the final draft for submission.
Competing interests
All authors declare that they have no conflicts of interest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The Ethics Committee of the Erasmus Medical Center, a tertiary referral medical center, stated that ethical permission was not required for this retrospective study.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.