
Abstract
An appendiceal mucocele (AM) is a rare right lower quadrant gastrointestinal pathology, frequently misdiagnosed during a diagnostic evaluation. An AM refers to a mucin-filled appendix caused by a complex interplay of pathophysiologic processes, most commonly obstruction of the appendiceal lumen. This case series presents three patient cases that used a diagnostic multimodality imaging approach to diagnose AM, to insure appropriate clinical management. The unique imaging characteristics of sonography, magnetic resonance imaging (MRI), and computed tomography (CT) utilized for the diagnosis of AM are discussed briefly, as part of this case series report.
The Austrian physician and pathologist, Carl von Rokitansky, first described an appendiceal mucocele (AM) in 1842. 1 An AM refers to the distension of the appendix due to obstruction of the lumen, which could have a neoplastic or non-neoplastic etiology. 2 Although the term AM is more prevalent in the literature, some current studies have reported that a “neoplastic appendiceal mucinous lesion” is more appropriate. 3 The incidence of AM is relatively controversial, and there is no consensus among experts. Most of the literature places the incidence of AM in the range of 0.07% and 0.7% occurrence, in appendectomy specimens.4 –6 The prevalence of AM has been shown to be higher in females.7,8 Appendiceal mucoceles can be asymptomatic or present with appendicitis-like clinical symptomatology and are often encountered in clinical practice, as an imaging incidental finding.8 –10 Appropriate diagnosis of this pathology is essential, as it can progress to rupture and spillage of the appendiceal contents, in the peritoneal cavity, which can lead to a pseudomyxoma peritonei (PP).11,12 Pseudomyxoma peritonei (PP) is a severe complication of AM because disseminating epithelial components of the appendiceal content can produce mucin in the abdominal cavity, thereby causing mucinous ascites or loculated mucinous collections.13,14 Therefore, diagnostic imaging is vital in diagnosing AM, as soon as possible to prevent complications.
Computed tomography (CT), magnetic resonance imaging (MRI), and sonography are the three well-known diagnostic imaging techniques for diagnosing AM, utilizing non-invasive means. One typical imaging detail for diagnosing AM, across all three imaging modalities, is to ensure that the suspected mass arises from the cecum and separate from the right ovary. 15 Each imaging modality has distinct characteristics distinguishing AM from more common right lower quadrant (RLQ) pathologies, especially in females. 15 It refers to the echogenic layering of debris within the lumen of the appendix, which is quite specific for AM. 7 A histopathologic examination is considered a diagnostic gold standard and essential for a definitive diagnosis. 2
This case series highlights the careful evaluation of pelvic masses, especially delineating their origin, as well as maintaining the characteristics of each diagnostic imaging modality, as part of the clinical decision-making process. The radiologists interpreting the sonography, CT, and MRI examinations, as part of this case series, were all experienced in their respective diagnostic imaging technique.
Case Series
Patient Case 1
A 61-year-old post-menopausal female reported to the sonography department for surveillance of a right adnexal cystic structure. A prior sonogram and pelvic MRI defined a right adnexal cystic structure, originating from the right ovary. The patient was not symptomatic and did not describe any pain or tenderness, in the RLQ. The sonographer noted a complicated cystic structure in the right adnexal region and annotated it as arising from the right ovary, similar to the previous sonographic report from the outside hospital. Numerous echoes were visualized in a lamellar pattern, without any color flow, and the mass was measured in all orthogonal imaging planes (See Figures 1–3) The sonographer also obtained the cine loop of this adnexal structure (See Supplemental Material QR code-Video 1). A discrete right ovary was not demonstrated during the current sonographic examination. Based on the sonographic features, the radiologist was not convinced that this structure was part of the ovary and suspected an AM, based on the “onion skin-like” image and lamellar echoes. A subsequent CT examination was scheduled for this patient in a week, and the CT demonstrated the cystic mass originating from the base of the cecum. A contrast-enhanced CT identified attenuation levels, associated with the cystic structure, ranging from 17 to 26 Hounsfield units. This suggested proteinaceous/mucinous material, consistent with a large appendiceal mucocele, which measured 4.3 × 7.7 cm in maximum dimension (See Figures 4 and 5).
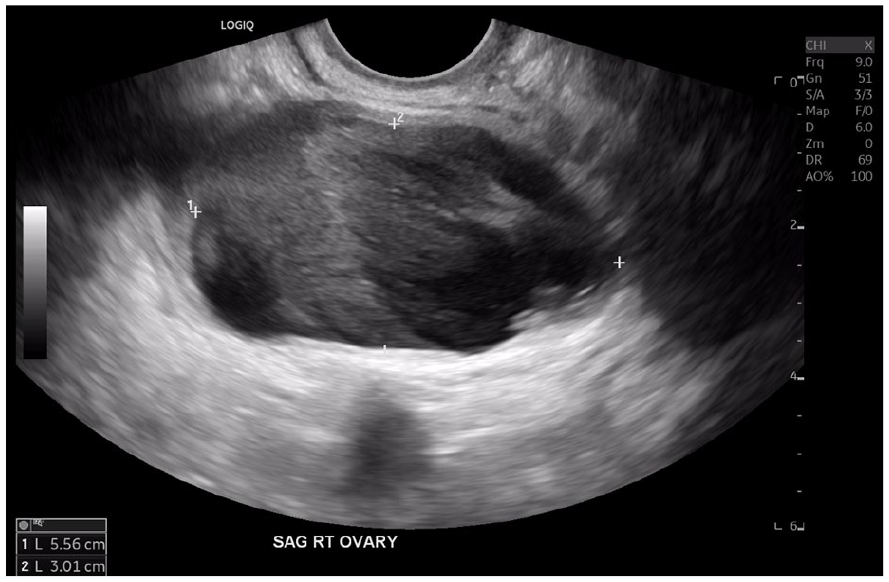
A sagittal sonographic image of the right adnexa showing complicated cystic structure with echoes set in a layered pattern. The mass was thought to be ovarian in origin.
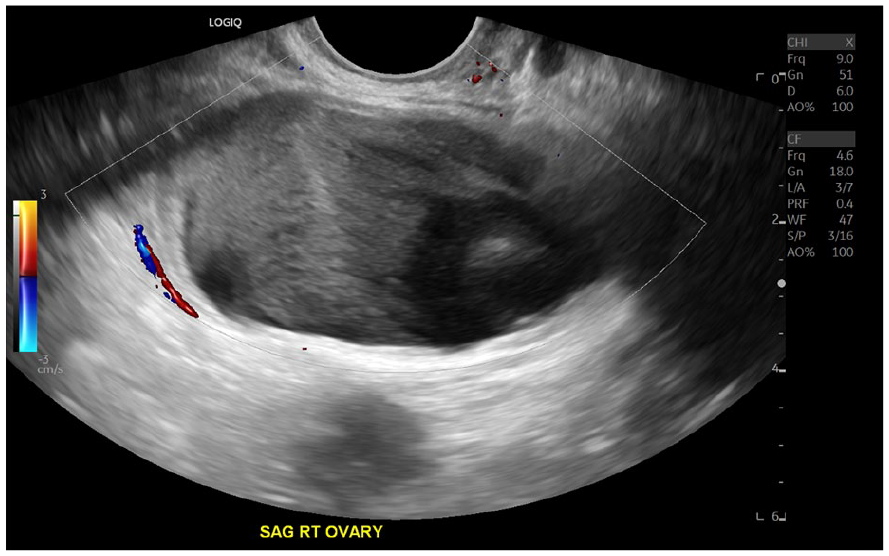
A sagittal sonographic image of the complicated cystic structure showing no peripheral or internal color flow.
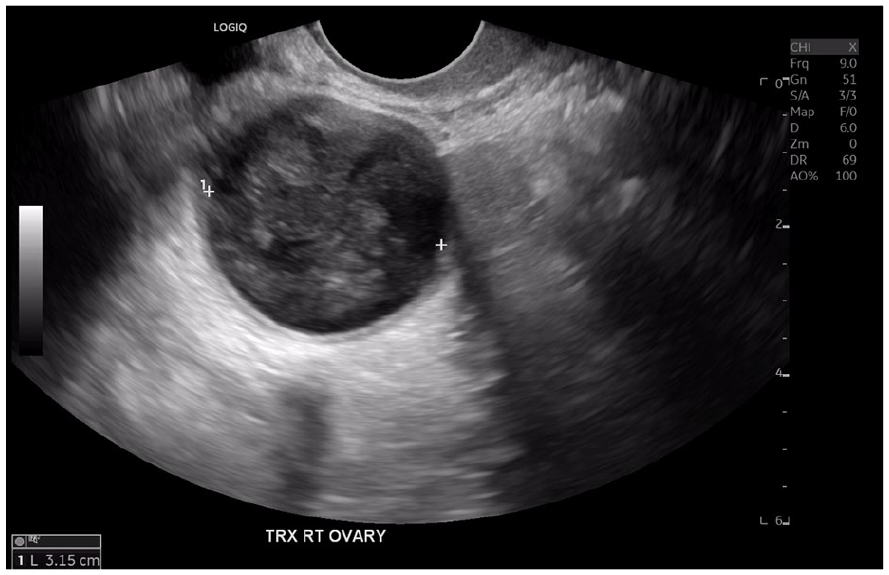
A short axis sonographic view of the right adnexal complicated cystic structure.
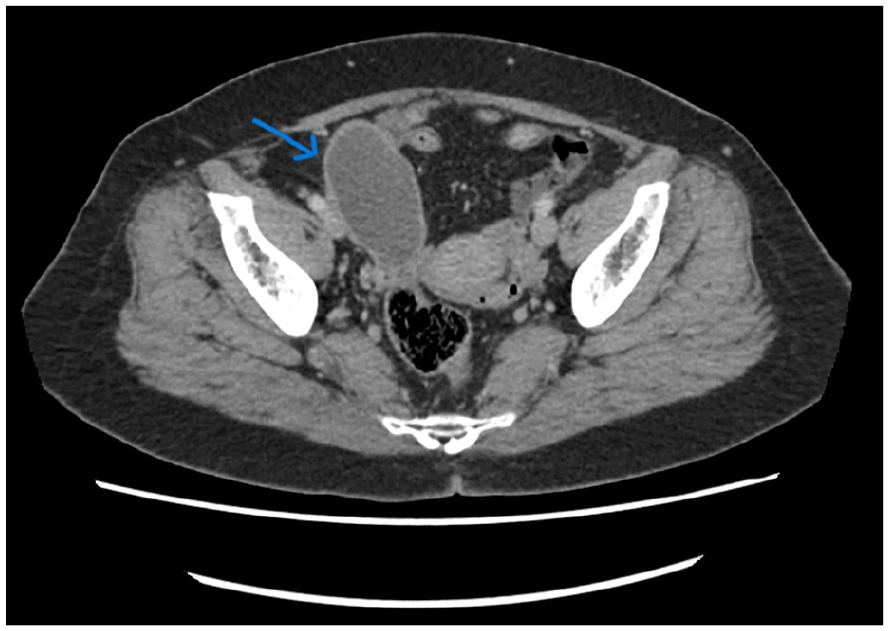
Transverse section of the right adnexal region illustrating the mildly thick walled cystic structure appearing to originate from the base of the cecum (blue arrow). The mass measured 4.3 × 7.7 cm in maximal dimension.
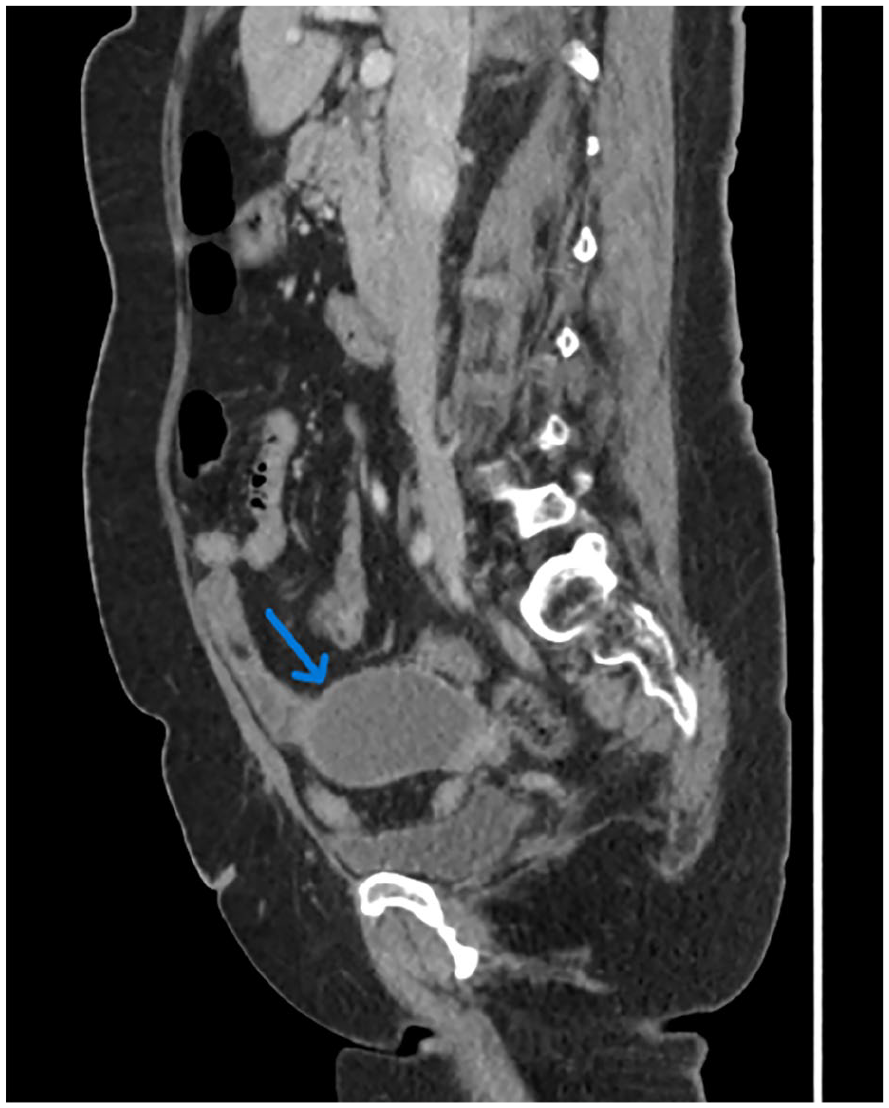
A contrast computed tomographic sagittal image shows the complicated cystic structure in the right adnexal region and demonstrating the origin of the mass posteriorly from the base of the cecum (See blue arrow).
Patient Case 2
A 43-year-old female was referred for a sonogram, for an intrauterine contraceptive device (IUD), localization to the pelvis. The patient was previously diagnosed with a 10-cm right adnexal hydrosalpinx, based on her prior MRI and multiple sonograms. The sonographer measured the cystic structure, during the current sonogram at 7.7 × 4.1 × 3.4 cm, in maximum dimensions (See Figures 6 and 7). The radiologist observed a “whorly/onion peel” appearance and suspected the cystic structure to be a mucocele rather than a hydrosalpinx, as previously reported on previous studies. A CT was recommended to confirm the sonographic suspicion of an AM. The contrast CT revealed the cystic structure to be intimately associated with the tip of the appendix. A subtle mural calcification was also suggestive of an AM (See Supplemental Material QR code-Video 2). The radiologist, interpreting the CT examination, recommended a surgical consult for this patient. Surgery was performed on this patient, and the tumor was successfully resected. The one-year repeated CT examination provided no evidence of tumor recurrence.
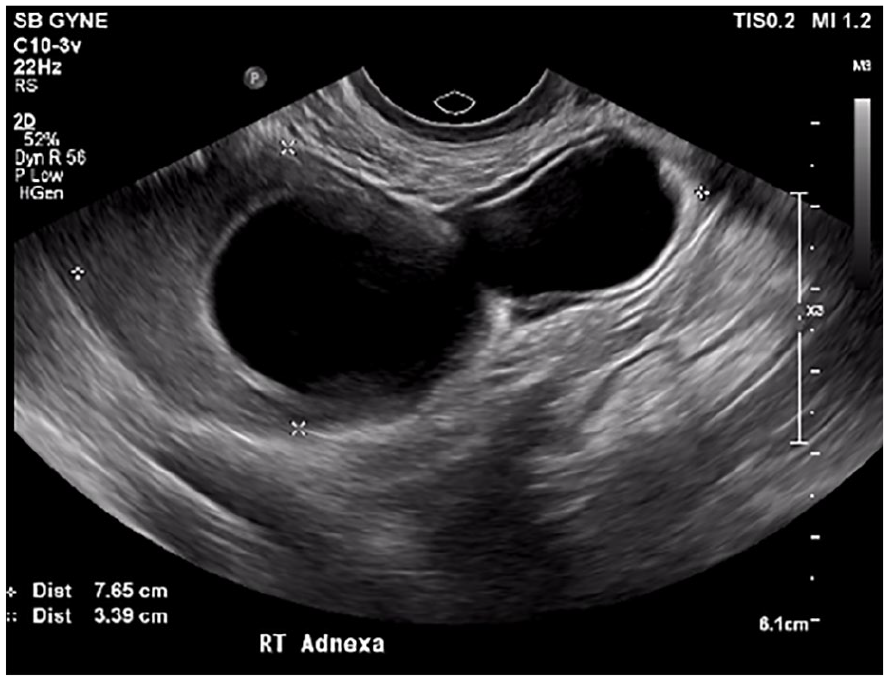
A sagittal sonographic view of the complicated cystic structure in the right adnexal region measuring 7.7 cm in maximal dimension.
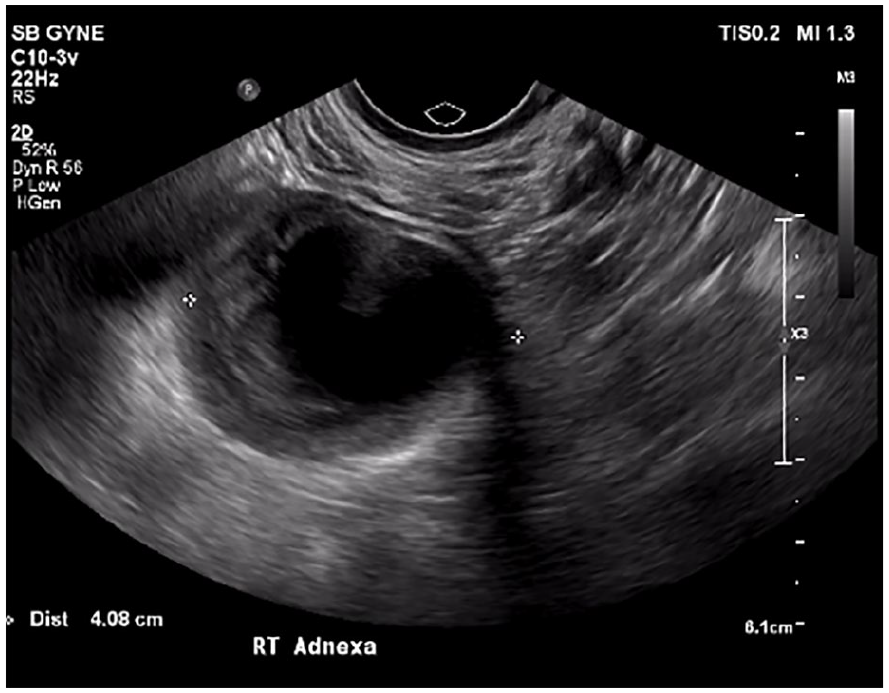
Sonographic short axis view illustrates the complicated cystic structure in the right adnexa measuring 4.1 cm in maximum dimension.
Patient Case 3
A 26-year-old female came to the sonography department for a repeated examination to recheck an ovarian cyst, visualized during a first-trimester obstetric sonogram. The prior two sonographic examinations, during the first and second trimester, documented a tubular cystic structure in the right adnexa. The radiologists, in two different hospitals, interpreted these as a right hydrosalpinx.
The patient was referred for surveillance of this cystic structure, post-partum, in two months. The sonographer assessed a non-tender, blind-ending loop, with complicated cystic components, within and separate from the ovary. This was noted with gentle pressure using a transvaginal transducer (See Figures 8–10 and Supplemental Material QR code-Video 3). The radiologist was suspicious of this lesion being a complicated AM and became skeptical about the previous sonographic diagnosis made during the patient’s pregnancy. The radiologist recommended a repeated MRI examination to elucidate the origin of the lesion. The T2-weighted MRI sequence revealed a hyperintense structure with peripheral enhancement and possible internal debris, adjacent to the right ovary. The mass appeared to originate from the base of the cecum (See Figure 11 and Supplemental Material QR code-Video 4).
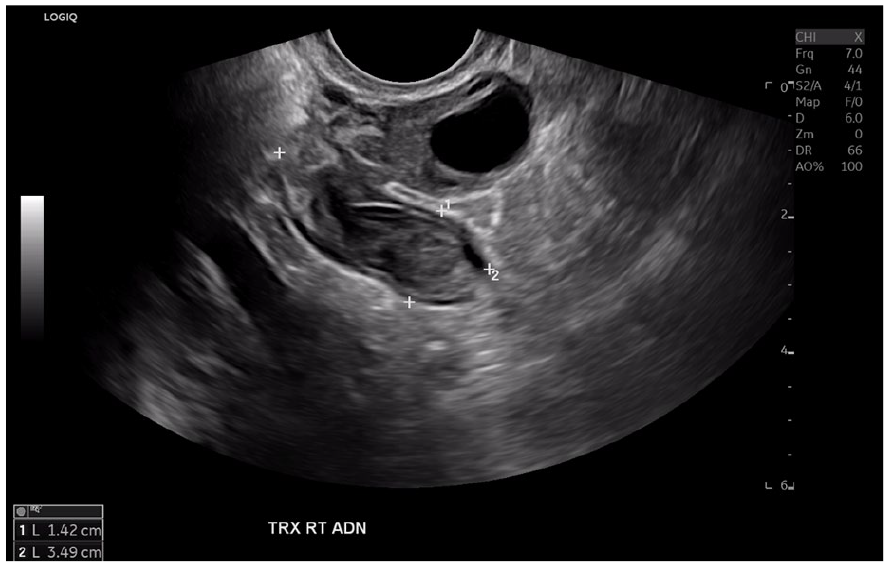
Sonographic transverse view of the right adnexa showing the solid structure measuring 3.5 cm in dimension.
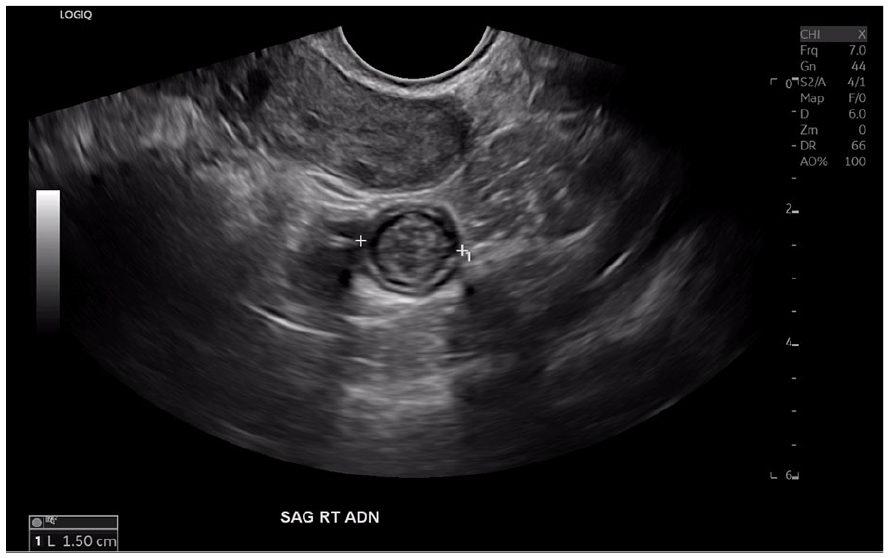
Sonographic sagittal view of the right adnexa illustrating the short axis of the mass measuring 1.5 cm in maximum dimension.
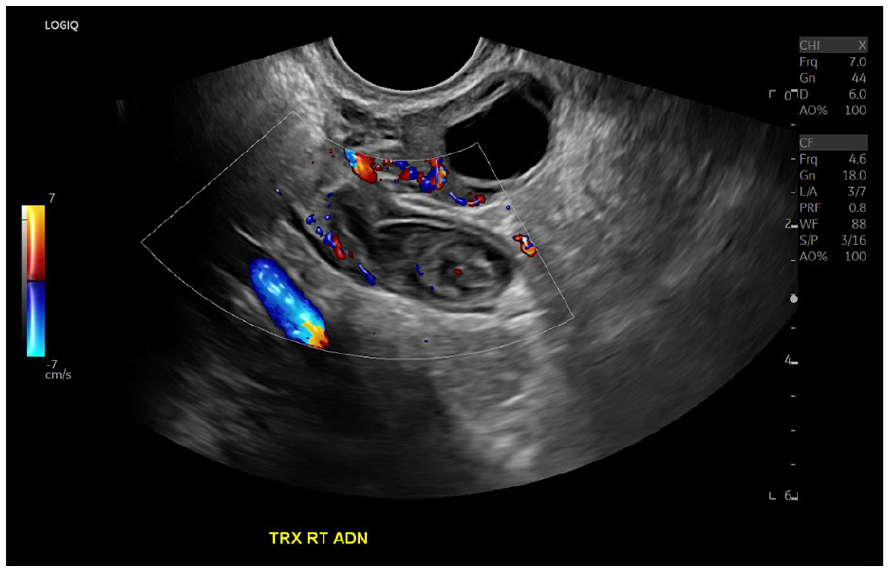
No significant internal or peripheral flow is appreciated, with Doppler, in this sagittal view of a solid structure in the right adnexa.

A magnetic resonance imaging (MRI) T2-sequenced sagittal image demonstrated the right ovary (green arrow), tubular cystic structure (blue arrow), and cecum (red arrow), which are seen distinct in this image. The tubular cystic structure (See blue arrow) is believed to be appendiceal mucocele and appears to be arising from the base of the cecum (See red arrow) and is separate from the ovary (See green arrow). No periappendiceal stranding was appreciated on MRI.
Discussion
The three case reports provided demonstrated the challenges of diagnosing an AM, if the relationship to the cecum is not demonstrated, as part of the imaging technique chosen. Some experts have suggested sonography, as the primary imaging technique for diagnosing AM, while others consider CT superior for diagnosing, staging, and surveillance of appendiceal tumors.6,14,16 It is usually the easiest to determine if a cyst, in the RLQ, originates from the cecum with a CT examination, which can be challenging on MRI and sonography, due to artifacts from air and bowel peristalsis. This case series would suggest that sonography works well as the primary imaging technique for AM, owing to its cost-effectiveness, portability, lack of radiation, and the characteristic sonographic sign. The “onion peel sign” or “the onion skin sign” has also been reported to be pathognomonic for an AM. 15 –17 It refers to the echogenic layering of debris within the lumen of the appendix and is quite specific for AM. 7 Acute appendicitis is the most common differential diagnosis that must be excluded from AM in symptomatic patients, since acute appendicitis and AM can coexist. 15 One retrospective cohort study reported specific CT imaging features for AM with coexisting acute appendicitis (e.g., cystic dilatation of the appendix, mural calcification, and a luminal diameter greater than 13 mm). 18 Many experts have considered the appendicular outer to outer diameter, greater than 15 mm, as convincing evidence for AM, which can be compared 6 mm or greater, for an acute appendicitis. 16 Other well-known differential diagnoses for cystic lesions in the RLQ, regardless of gender, are periappendiceal abscess, peritoneal inclusion cyst, lymphocele, enteric duplication cyst, mesenteric cyst, and Meckel diverticulum. In females, the only additional common differential diagnoses to consider, in the RLQ, are right hydrosalpinx, right tubo-ovarian abscess, ectopic pregnancy, and right ovarian cyst or neoplasm.15,19
A typical simple appendiceal AM can appear on CT, as a well-defined water density mass, in the right lower quadrant, or sometimes with an intramural curvilinear calcification. 16 A mural calcification strongly supports the diagnosis of an AM, in the RLQ. 20 However, CT is not sensitive and specific enough to differentiate between a benign and malignant AM. Some authors have suggested mucocele wall irregularity and soft tissue thickening, as criteria for malignancy. 21 On MRI, the AM demonstrates varying signal intensity due to differing luminal protein content. 15 Evaluating intraluminal air and calcifications, in AM, can be challenging with MRI. AM often appears hypo-intense on the T1-weighted MRI sequenced images and hyperintense on T2-weighted MRI sequenced images, although the signal characteristics can vary depending on the degree of protein and mucin, within the lumen. 16 Mural nodularity and irregular wall thickening of the appendiceal mucocele can be suggestive of malignancy, as seen on MRI and CT examinations. 15
The literature has highlighted four types of AMs, based on the cause of obstruction (e.g., retention cysts, epithelial hyperplasia, mucinous cystadenoma, and mucinous cystadenocarcinoma).22,23 This classification might be more useful in surgery, since the surgical approach chosen is based on the appropriate etiology. The World Health Organization (WHO) has classified an AM into serrated polyps, hyperplastic polyps, low-grade appendiceal mucinous neoplasms (LAMNs), high-grade appendiceal mucinous neoplasms (HAMs), and mucinous adenocarcinomas. 3 Identifying if an AM lesion may be malignant pre-operatively is vital for appropriate management. 17 The literature provides the use of both classifications, to determine the prognosis and management of the pathology. The WHO classification is more dependent on the histopathologic examination. Imaging alone cannot reliably categorize the types of AM. In the current case series, the pathology reports were unavailable, for all three specimens, due to technical reasons. Hence, the diagnosis of AM in the current patient cases was based on a diagnostic multimodality imaging approach, prior to surgery. Regardless, the standard of care for AM is a complete appendectomy for tumors less than 2 cm and right hemicolectomy for tumors larger than 2 cm. 6 An alternative opinion is to recommend a right hemicolectomy for mucinous cystadenocarcinoma and appendectomy for hyperplastic lesions and cystadenomas, if the resected tissue margins are clear. 24 Some consider the prognosis of benign mucocele to be excellent, while a malignant mucocele/mucinous appendiceal neoplasm has a 5-year survival rate of only 20% to 25%. 21 Therefore, AM should not be missed sonographically on the preliminary imaging, as the prognosis can worsen if AM progresses to PP in the abdominal cavity. A contrast-enhanced CT examination might add further diagnostic value to the sonographic suspicion of AM and can add to the treatment and management plan of the patients. A systematic review, with or without a meta-analysis, comparing the diagnostic test accuracy of CT, sonography, and MRI for the non-invasive AM diagnosis would be a beneficial for higher-level diagnostic evidence.
Conclusion
An AM is a relatively rare disease that could be misdiagnosed, during a diagnostic evaluation, especially as ovarian pathology demonstrated with sonography or MRI. To provide an imaging diagnosis of AM, it is vital to find the origin of any suspicious cystic mass in the RLQ. The use of sonography, CT, and MRI are preliminary non-invasive diagnostic imaging techniques to detect an AM. Interpreting physicians need to be aware that AM may present clinical and on imaging studies as a possible appendicitis.
Footnotes
Acknowledgements
The authors acknowledge our families, colleagues, management, and radiologists at the prestigious St. Boniface Hospital (Winnipeg) and the University of Manitoba for providing the necessary support for publishing this rare pathologic case series, with Sage Publications Inc.
Ethics Approval
Ethics approval was obtained from the University of Manitoba with reference number: REB Registry Number: H2024:208 (HS26544).
Informed Consent
Informed patient consent was obtained from all three patients involved in this case series report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.