
Abstract
Individually, inguinal hernias and acute appendicitis are common, but the combination of the two, acute appendicitis within an inguinal hernia or Amyand hernia (AH), is rare. The overwhelming majority of AH cases are in males and discovered during surgery. To date, only three case reports in the literature of this pathology have been diagnosed with sonography. This is a report of an AH diagnosed in a woman with sonography.
The finding of acute appendicitis within a hernia sac is a rare occurrence. 1 When the appendix is in an inguinal hernia, it is known as Amyand hernia (AH). Amyand hernias are named after Claudius Amyand, who first described his incision of an assumed groin abscess in 1736. 1 Instead of a simple abscess, he found a herniated appendix in the inguinal canal. The appendix was excised and the patient recovered. It is important to distinguish this from an appendix in a femoral hernia, called a DeGarengeot hernia, correspondingly named for the first physician to report the anomaly, Rene Jacque Croissant de Garengeot. 1
Inguinal hernias, and subsequently AH, are much more common in men than in women. 2 A review of the literature from 1969 to 1999 found only 60 case reports of acute appendicitis (AA) in an external hernia being diagnosed preoperatively. 3 Since then, a handful have been diagnosed with computed tomography (CT), but there are only three reports of AA within AH being diagnosed sonographically.4–6 This is a report of an AH in a woman in her early 70s diagnosed using sonography and confirmed with CT. This case is unique because of the rarity of the pathology and method of diagnosis. To the author’s knowledge, it is the first case report of an AH preoperatively diagnosed with sonography on a woman.
Case Report
A woman in her early 70s with a history of a right inguinal hernia repaired using the McVay technique six years prior presented with a painful, palpable, irreducible right groin lump. The McVay technique involves using sutures to repair the defect without the use of a prosthetic mesh. She reported that since the herniorrhaphy, she had an intermittent, reducible right groin lump but that over the preceding four days, the lump became painful. She reported malaise and increased flatus. A complete blood count showed her white blood cell count to be elevated at 10,700 cells/dL.
The patient was admitted for further evaluation of a possible right groin abscess or recurrent hernia. A sonogram was performed using a Phillips HDI5000 (Bothell, Washington) with a 5-MHz curvilinear transducer and a 7-MHz linear transducer. An incompressible, dead-ending, tubular structure with a bowel-like appearance was seen, measuring approximately 9 mm in diameter, surrounded by a small amount of apparent free fluid and echogenic fat (Figure 1). These features were inferiomedial to the inguinal ring. A diagnosis of acute appendicitis within a recurrent right inguinal hernia was made and confirmed by a subsequent CT scan (Figure 2).
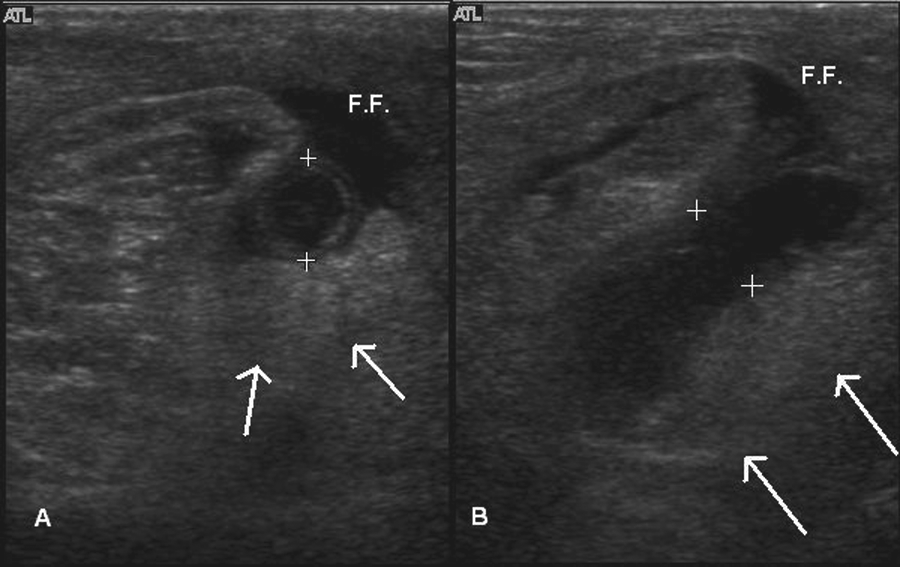
(A) Transverse and (B) longitudinal sonogram of the right groin showing the dilated appendix (calipers), echogenic fat (arrows), and peri-appendiceal free fluid (F.F.). Distance between calipers is 9 mm.
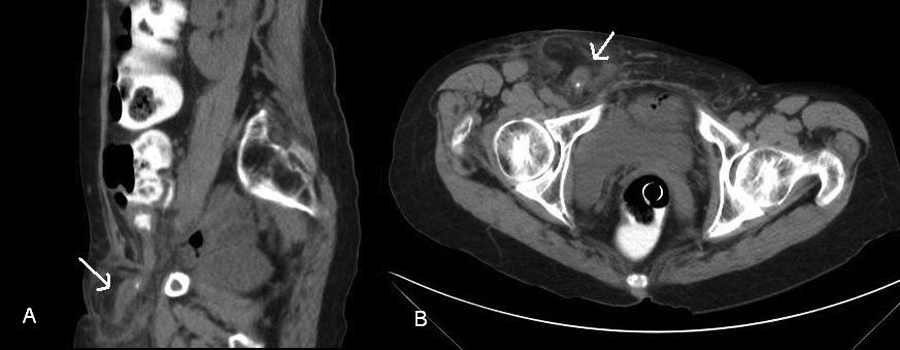
(A) Coronal and (B) transverse computed tomography images showing the appendix in the hernial sac (arrows).
The patient was taken urgently to the operating room. The appendix, as well as some peritoneal fat, was inflamed and incarcerated in a recurrent right inguinal hernia. The inflammation included the intra-abdominal portion of the appendix as well. The appendix was excised and the hernia repaired using the McVay technique. Postsurgical pathological examination of the excised appendix confirmed the surgeon’s initial impression of acute appendicitis.
The patient recovered well and was discharged on the third day. Follow-ups at 9 and 18 months found the patient to be doing well with no recurrence of the right inguinal hernia.
Discussion
Hernias
A hernia is the protrusion of an organ or tissue through an opening in its surrounding walls, especially in the abdominal region. Groin hernias can be of two basic subtypes: inguinal and femoral, with inguinal being further divided into direct and indirect. Shadbolt and colleagues 7 summarize groin hernias as (a) direct hernias that pass medial to the inferior epigastric vessels, (b) indirect hernias that pass lateral to the inferior epigastric vessels and follow the path of the inguinal canal inferiomedially, and (c) femoral hernias lie in the femoral canal, medial to the femoral vein.
Hernias are common, and hernia repair surgery, or herniorrhaphy, is the most common surgery performed in the United States. 2 A large review of cases in the United Kingdom found an overall lifetime risk of an inguinal hernia alone at 25% for men and 3% for women. 8 An extensive review of National Hospital Discharge Survey (NHDS) and National Survey of Ambulatory Surgery (NSAS) data found that hernias are much more common in men than in women, with 90% to 95% of all hernia operations being performed on men. 2 Acute appendicitis and hernias are both common conditions, with hernias occurring more often than AA. 9 The lifetime risk of AA is 8.6% for males and 6.7% for females. 9
An appendix appearing in an external hernia has been reportedly found in up to 1% of hernia cases. 10 Although patients with a herniated appendix are at an increased risk of developing acute appendicitis, it is nevertheless very rare for a patient to present with the combination of AA within a hernia. In a review of 8692 cases of AA, only 11 were found (0.13% or 13 per 10,000) to occur in external hernias. 1
Clinically, an AH usually presents similarly to an inguinal hernia or strangulated bowel.11,12 Patients often have a painful, reddened, edematous groin mass that may or may not be reducible. 12 Symptoms may also be similar to AA, with right lower quadrant or periumbilical pain and rebound tenderness. 6 Fever and white blood cell counts are nonspecific. 12
The exact mechanisms by which the appendix becomes incarcerated and then inflamed within the hernia are unclear. The normal location of the appendix is close to where inguinal and femoral hernias occur, but it is unknown whether the appendix becomes inflamed and subsequently incarcerated or whether the tight confines of the hernia cause strangulation and subsequently inflammation. Weber and colleagues 3 propose that a herniated appendix is at an increased risk of restricted blood flow because of the tight confines of the neck of the hernia. They further postulate that the partial strangulation leads to inflammation and edema, resulting in infection and necrosis.
Appendicitis within a hernia has implications for surgery, as it changes the operative approach. Instead of a simple herniorraphy, the surgeon must also perform an appendectomy. Although there is not a clear consensus, the literature tends toward favoring a hernia repair without prosthetics such as mesh because of the increased risk of infection.13,14
There are few studies regarding the prognosis of patients with AH and AA, with no clear consensus. Because the acute nature of appendicitis precludes proper bowel preparation, there is a resultant increase in infection when performing an appendectomy in addition to herniorrhaphy. The wound infection rate has been reportedly as high as 50%. 10 In one small study, mortality rates were 30% in elderly patients with perforated appendices 13 ; less complicated patients demonstrate no increase in mortality. 10 It has been reported that right lower quadrant peritonism and age older than 90 years are predictive of a poor outcome. 15
Imaging
By sonography, the appendix appears as a blind-ending, bowel-like, tubular structure and can be identified by a characteristic target-like appearance when viewed in transverse. Research has shown that an appendix measuring greater than 6 mm in the A-P dimension alone is suspicious for appendicitis with a 57% to 98% sensitivity.16,17 The presence of echogenic fat and focal tenderness over the appendix increases this sensitivity considerably. 16
Inguinal hernias appear as an extension of abdominal fat, bowel, or peritoneum in the inguinal canal. Although hernias in general are not often imaged before surgery, imaging can be useful to diagnose hernias. Diagnosis by sonography is reported to obtain sensitivities as high as 94% to 100%.18,19 The inguinal canal should be imaged with the patient supine, before and while the patient performs the Valsalva maneuver. If no hernia is visualized, images should be taken while the patient is standing. 20
An appendix within the inguinal canal will appear as a single tubular structure; a herniated loop of bowel will appear as two tubular structures and will not have a blind end. 6 Bowel may also show peristalsis.7,16,20 There may also be inflamed, echogenic fat and free fluid in the hernia in addition to the appendix. Differential diagnosis for groin masses with these sonographic characteristics includes strangulated or incarcerated hernia, DeGarengeot hernia, Richter hernia, inguinal abscess, inguinal adenitis, or an abnormally presenting neoplasm.
Although CT is often the preferred method of imaging groin masses and hernias, 7 sonography is useful because it is dynamic, real-time, and low cost and does not expose the patient to ionizing radiation. Because it is real-time, it can be used to diagnose sliding hernias that might otherwise be missed. 21 A sliding hernia contains a mobile combination of abdominal viscus and parietal peritoneum. 5 Sonography is not without its weaknesses. It is highly user dependent and has a small field of view relative to CT. Care should be taken to use proper machine settings. It has been reported that the use of spatial compounding was helpful in the diagnosis of acute appendicitis. 22
Conclusion
Inguinal hernias and acute appendicitis are common conditions. An appendix in an inguinal hernia, called an Amyand hernia, is rare, and acute appendicitis within an AH is very rare. It is exceedingly rare to diagnose AH preoperatively, but it is useful because the presence of acute appendicitis within the inguinal hernia changes the surgical risks and approach.
Computed tomography is more commonly used to diagnose hernias in general, but because sonography is operated in real-time, it can be used to see movement, such as a sliding hernia or peristalsis, that CT is unable to visualize.
Footnotes
Acknowledgements
The author’s colleague, Ralph Keith, RDMS, performed the sonographic examination in the patient described, and the author thanks him for his permission to publish the case study. Special thanks to Dr Sid Green, a senior radiologist at Salem Radiology Consultants, for taking the time to provide valuable input and assistance.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.