
Abstract
Appendicitis is a surgical emergency that can mimic many other abnormalities. Early diagnosis is critical to reduce the risk of perforation and potentially life-threatening complications. The use of sonography has proven to aid in accurately diagnosing an inflamed appendix without adversely affecting the rate of perforation. However, the accuracy of sonography is highly operator dependent. This case demonstrates the classic clinical presentation of appendicitis with the incorporation of sonographic findings to support the diagnosis.
Acute appendicitis is one of the most frequent causes of abdominal surgery. 1 The appendix becomes obstructed, altering the permeability of the walls, allowing bacteria to invade the lumen of the appendix.1,2 The risk of perforation and associated complications results in approximately 30% of people undergoing appendectomy who ultimately are found to have a normal appendix. 3 The diagnosis is often difficult to make because patients present with symptoms similar to many other abnormalities. The incorporation of diagnostic imaging in ambiguous cases has helped to accurately diagnosis acute appendicitis.3,4 Sonography, a rapid, noninvasive examination involving no patient preparation, is a prudent choice when evaluating for a possible surgical emergency. However, the accuracy of sonography is highly user dependent.3,4
Methods
To begin the examination, the patient should be positioned supine and instructed to identify the area of greatest pain to the sonographer. In classic appendicitis, this region in the right lower quadrant (RLQ) is referred to as McBurney’s point, the area midway between the umbilicus and the anterior iliac crest and where the appendix is typically located. 5 The sonographer should begin to evaluate this area with a high-frequency linear-array transducer looking for a blind-ending, noncompressible tubular structure. The amount of pressure applied while scanning should vary to determine normal compressible loops of bowel versus an inflamed appendix. Adequate pressure is achieved when the iliac vessels and psoas muscle are visualized. 6 The graded compression also provides a better scanning window by displacing bowel and overlying gas. To avoid false-negative examinations, the sonographer should evaluate the entire length of the appendix from the origin at the base of the cecum to its distal end.1–3,6 If the appendix is not visualized, the rest of the pelvis and abdomen should be interrogated for an atypical location of the appendix or an alternative source of the patient’s pain. 1
The sonographic appearance of an appendicitis is described as a blind-ending, noncompressible tubular structure that measures greater than 6 mm in diameter.1–4,6,7 The wall thickness alone will measure greater than 2 mm.1,2,7 An inflamed appendix is often referred to as a “target” sign because of the alternating hypoechoic and hyperechoic layers. In most cases of obstructive appendicitis, the center hypoechoic area represents fluid or pus, whereas the hyperechoic ring is mucosa. The outer hypoechoic layer is edematous appendiceal wall.1,4,6 A complex mass or free fluid in the pelvis may indicate that the appendix has already perforated and the concentric layers are no longer intact. Inflammation may also cause increased vascularity in the walls of the appendix and surrounding tissue 6 as well as increased echogenicity of the pericecal fat.1–3,7 Another characteristic occurring in approximately 50% of children with appendicitis is echogenic foci with posterior acoustic shadowing within the lumen of the bowel, known as appendicolith. 6
Case Report
A 10-year-old patient presented in the emergency room with severe RLQ pain and fever for one day. The patient stated that the pain initially started in the left lower quadrant/periumbilical area but eventually localized to the RLQ. On physical examination, the patient had RLQ rebound tenderness and guarding. The child also experienced one episode of vomiting and persistent nausea. A sonogram was ordered to evaluate for acute appendicitis.
The sonographic examination of the RLQ revealed a blind-ending, noncompressible tubular structure at the location of the patient’s pain (Figures 1 and 2). The appendix measured 1.2 cm in the anterior-posterior dimension, double the diameter of a normal appendix. The transverse image also demonstrated the alternating hyperechoic and hypoechoic layers of the “target” sign (Figure 3). The walls of the appendix appeared hyperemic with power Doppler imaging, with increased echogenicity of the periappendiceal fat, indicating inflammation (Figure 4). The sonographic findings of this examination were considered consistent with an acute appendicitis.
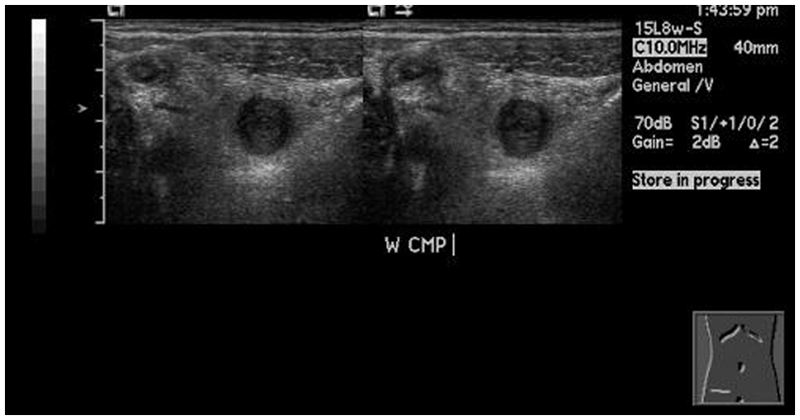
Dual image of transverse appendix demonstrating a noncompressible appendix using a linear-array transducer.
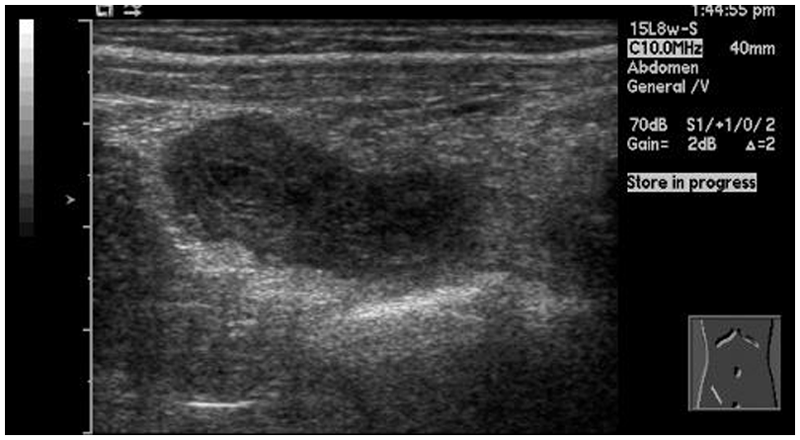
Longitudinal image of the distal end of the appendix demonstrating a blind-ending tubular structure.
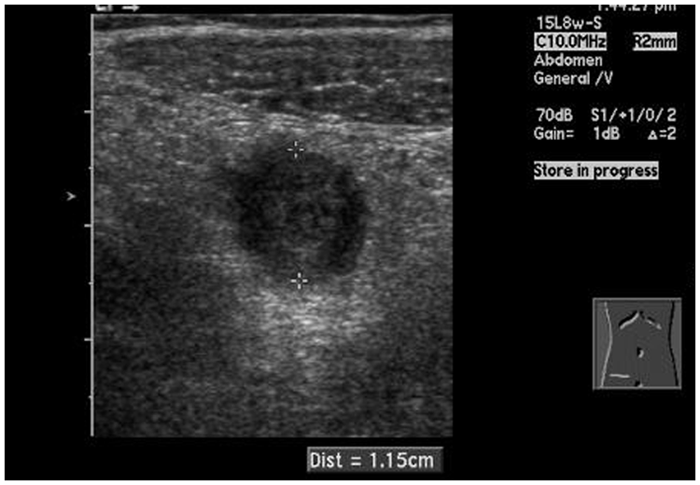
Transverse image of inflamed appendix measuring 1.2 cm in the anterior-posterior dimension.
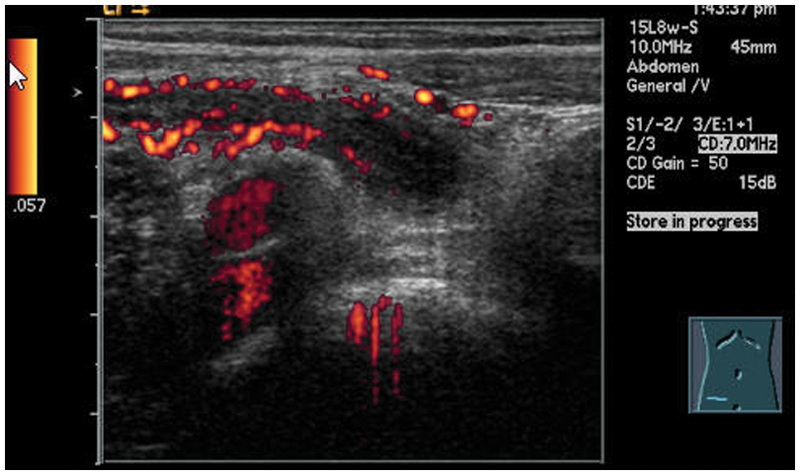
Longitudinal power Doppler image of an inflamed appendix with hyperemic walls anterior to iliac vessels.
The diagnosis of acute appendicitis was made based on the patient’s symptoms, physical examination, and sonographic findings. To reduce the risk of rupture, the patient underwent an emergency laparoscopic appendectomy. The surgical report confirmed the diagnosis of an acutely inflamed appendix with omentum adherence, without any signs of gross perforation. The patient tolerated the surgery well and was released from the hospital on postoperative day two with no reported complications.
Discussion
The appendix, a diverticulum arising from the inferior tip of the cecum, 2 serves no known significant physiologic function in humans. 4 Appendicitis is usually caused by obstruction of the appendiceal lumen. A number of different factors may cause the obstruction, including fecal material, foreign body, seeds, parasites, inflammation, or lymphatic hypertrophy. The obstruction does not allow secretions to drain from the walls of the appendix, resulting in distention and increased permeability of the lumen. Bacteria are then able to invade the wall of the appendix, causing pain and inflammation.1,2 Regardless of the cause of appendicitis, early surgical intervention is required to prevent the appendix from rupturing.
Appendicitis is the most common surgical abdominal emergency, affecting one in seven people in their lifetime. 3 The appendix may become obstructed at any age; however, it most commonly occurs between ages 10 and 30 years 8 and rarely before age 2 years.1,2,4,6,8 Males have a slightly higher lifetime risk of appendicitis than females, 8.6% and 6.7%, respectively. 2 Individuals experiencing RLQ pain, fever, nausea, vomiting, and loss of appetite should seek immediate medical attention to rule out appendicitis as there is a less than 1% mortality rate in nonperforated appendicitis. 2
The diagnosis of acute appendicitis is primarily based on the patient’s symptoms and physical examination. However, many gastrointestinal and gynecologic abnormalities mimic appendicitis, making the diagnosis difficult. The clinical decision to operate to avoid complications associated with a delayed or missed appendicitis results in 20% to 30% of people undergoing surgery who are found to have a normal appendix. 3
The incorporation of diagnostic imaging has aided in accurately diagnosing acute appendicitis without increasing the rate of perforation. 3 Sonography is an accurate, rapid, noninvasive, and inexpensive examination that can be performed in real time to provide significant additional information to the clinical workup with no exposure to harmful radiation. Sonography has a sensitivity of 88% and specificity of 96% when performed properly. 1 The major disadvantage of sonography is that the accuracy is highly dependent on the experience level of the sonographer.3,4 Other limitations of sonography include patient body habitus, overlying bowel gas, atypical location of the appendix, and an uncooperative patient.
An early diagnosis of acute appendicitis is especially important in children. The progression to a perforated appendicitis occurs within 6 to 12 hours in infants and young children 1 compared with 36 hours in adults. 2 The diagnosis in children is often more difficult due to their inability to articulate their symptoms, and their symptoms can mimic other common childhood illnesses. The rate of perforation is as high as 70% in preschool-age children compared with 30% in children and 21% in adults. 1 The morbidity rate and postsurgical complications increase after the appendix has ruptured. 4 Peritonitis or the formation of an abscess can result from bacteria from the appendix leaking into the peritoneum.1,4 It may be more difficult to identify a ruptured appendicitis on sonography because the lumen is no longer distended.4,6 Including sonography in the workup for acute appendicitis has proven to reduce the number of perforations and negative appendectomies. 3
Computed tomography (CT) is another imaging modality that is used to assess suspected appendicitis. The sensitivity and specificity of CT are slightly greater than sonography; however, CT is a more expensive test to perform, and there is the risk of long-term damage associated with radiation used in CT scans. 4 The accuracy of sonography performed by an experienced sonographer nearly parallels that of CT. 4 There has been research to support the decision to perform sonography first on patients with suspected appendicitis and then proceed to CT for patients with negative or equivocal results.4,6 This approach has increased the overall accuracy of diagnosing appendicitis. 4
Appendectomy is usually the standard treatment plan for appendicitis.8,9 Open appendectomy is more commonly performed because it is a faster, less expensive surgery; however, the popularity of laparoscopic appendectomy is increasing. With the laparoscopic approach, there are fewer wound infections, shorter hospital stays, and more favorable cosmetic outcome for the patient. When an appendix has perforated, the surgery will be delayed until the abscess can be properly drained. All patients undergoing an appendectomy are started on antibiotics to reduce postoperative wound infections. The prognosis of an appendectomy, regardless of the approach, is excellent. 9
Conclusion
Symptoms of appendicitis can mimic many other abnormalities. Early diagnosis is necessary to reduce the risk of perforation and potentially life-threatening complications. The addition of diagnostic imaging to the clinical workup has proven to aid in accurately diagnosing appendicitis. The number of negative appendectomies has been reduced without adversely affecting the rate of perforation. This case demonstrates a classic clinical presentation of an inflamed appendix with the incorporation of sonographic findings to support the diagnosis. The use of sonography rather than CT eliminated the patient’s exposure to potentially harmful radiation. Sonography is an extremely valuable tool in diagnosing appendicitis when performed by an experienced sonographer with the proper knowledge.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.