
Abstract
Objective:
Given the sophistication of ultrasonography, it is possible to explore and better comprehend the link between gestational age (GA), fetal weight (FW), and the diameter of the umbilical vein (UV). Therefore, the aim of this study was to determine whether a correlation exists between the Doppler indices, within the UV, compared with GA and FW, in a normal pregnancy.
Materials and Methods:
The design of this work was a cross-sectional analytical study. The sample size was calculated to include a sample size of 61, for statistical significance. A convenient sampling technique was used to collect the data. The inclusion criteria were to recruit pregnant women between the ages of 18 and 45 years, in the second and third trimester of pregnancy. In this cohort, the exclusion criteria were to be no co-existing maternal medical conditions chronic hypertension, gestational diabetes, cardiovascular problems, infections, hypercoagulability, and endocrine disorders.
Results:
A total of 61 pregnant women participated in this study, with a mean age of 25.21 ± 2.79 years. The mean GA was 32.4 ± 6.5 weeks. GA demonstrated a strong positive correlation with UV diameter (r = .772, p < .001), UV velocity (r = .687, p < .001), and UV volume (r = .732, p < .001). UV diameter showed a strong positive correlation with UV velocity (r = .593, p < .001) and an even stronger positive correlation with UV volume (r = .928, p < .001). UV velocity showed a strong positive correlation with UV volume (r = .754, p < .001). These findings may suggest that as GA increases, there are corresponding increases in UV diameter, velocity, and volume.
Conclusion:
In this cohort, the data collected demonstrated significant correlations between UV Doppler indices, GA, and FW, in normal pregnancies.
The growth of the fetus depends critically on the umbilical cord (UC) and vessels, which provide an important connection between the placenta and the growing fetus. Although the UC is most probably the only organ that dies when life begins, it is one of the most important parts of the feto-placental unit, playing a role in determining the way extra uterine life will begin. 1 Wharton’s jelly covers the two umbilical arteries (UAs) and one umbilical vein (UV) that make up the cord. The vein, which is greater in diameter than the arteries, is the only conduit through which the fetus receives oxygenated blood that is rich in nutrients from the placenta. 2 In a normal pregnancy, the average diameter of the UV varies from 2 mm at 14–15 weeks gestation to 7–8 mm at term. 3 Although the UC can be detected with sonography, as early as 6 weeks into pregnancy, it is typically easier to visualize by the eighth or ninth week.4,5 Classically, umbilical blood flow is determined using a combined two-dimensional (2D) real-time pulsed Doppler system. Grayscale imaging of the investigated segment of the cord vessel is typically done using a 3.5-MHz linear transducer. The desired imaging scan plane is directed parallel to the longitudinal axis of the UV, yielding visualization of a minimum length of 1 cm. 6 The use of Doppler to study fetal hemodynamics has largely focused on flow velocity waveform analysis. Few data have appeared on volume flow, and this may be due to the lack of precision of measurements, which may be due to the cross-sectional vessel size. For example, the increase in vessel size is responsible for most of the rise in umbilical venous volume flow. 7 The flow velocity profile of the UV, in the second and third trimester of pregnancy, is typically continuous and non-pulsatile. In the early first-trimester fetus, the UV flow pattern is normally pulsatile. The degree of plasticity that decreases with gestation is also due to a reduction in cardiac afterload, as well as a decrease in placental resistance. Pathological pulsation in the UV flow in the second and third trimester of pregnancy typically reflects a state of high placental vascular resistance. 8
During routine obstetric sonography, the size of the UV is typically not assessed or considered. 9 Usually, features outside of the UC receive more attention. Previous studies have shown that measuring the UV’s diameter can help with the early identification of particular congenital abnormalities, as it relates to the increased diameter. 10 In addition, it may help to provide early fetal detection of intrauterine growth restriction (IUGR). The blood flow velocity and ultimately the growing fetus’s blood supply are directly impacted by UV size. The finding of absent end diastolic flow in the UA is acknowledged as a sign of increased placental vascular resistance. It is also related to an increased risk of IUGR, imminent fetal asphyxia during labor, and high perinatal mortality. Increased diastolic flow velocities in the fetal middle cerebral artery have been described as a sign of redistribution of blood flow, in chronic hypoxemia. Normally, the blood flow velocities in umbilical and portal circulation are steady and without pulsations. 11 While the rate of rise is unknown, it is known that the linear diameters of the UV and the UC increase with advancing GA. 12
The rationale behind investigating the correlates to the UV was to understand its potential as a predictive marker for various fetal growth abnormalities, development issues, or other health complications. By establishing such correlations, medical professionals can potentially use this information for early detection, monitoring, and management of certain conditions in pregnant women and their fetuses. This type of research has yet to be conducted in Pakistan and would be impactful to explore this aspect. This highlights an important gap in scientific knowledge that could have significant implications for maternal and fetal health in that population.
Material and Methods
This research was designed as a cross-sectional analytical study and conducted at a university clinic, in Lahore, Pakistan. The study length lasted for 9 months. The calculated sample size was 61, based on the expected correlation between UV diameter and estimated fetal weight (FW), r = .57. 13 A convenient sampling technique was used to collect the data. The inclusion criteria were to recruit pregnant women between the ages 18 and 45 years, in their second and third trimester of pregnancy. It was also important that participants had no co-existing maternal medical conditions, chronic hypertension, gestational diabetes, cardiovascular problems, infections, hypercoagulability, and endocrine disorders. Additional exclusion criteria were any pregnant participants with any existing pathology (e.g., umbilical cord knot, cyst) related to the UV. In addition, a fetus afflicted with IUGR, deemed small for GA, a fetal congenital, or chromosomal anomalies were excluded from this study.
Procedure
Data were collected after the approval from the Research Ethical Committee, The University of Lahore (IRB # REC-UOL-518-09-2023). The rules and regulations set by the ethical committee of University of Lahore were followed while conducting the research and the rights of the research participants were respected. Written informed consent was taken from all the participants. All information and data collection were kept confidential. Participants’ identifiers were anonymized, throughout the study. The subjects were informed that there were no disadvantages or risks to them participating in the study. They were also informed that they were free to withdraw, at any time, during the study. The patient’s participation, in this research study, was totally voluntary. They were not penalized in any way, should they have decided not to participate or withdraw from the study.
Technique
The ultrasound equipment system used was a Xario XG (Canon Medical Systems, Tokyo, Japan) along with a convex transducer that had a transmit frequency of 2–5 MHz. The patient exam couch was prepared and positioned for patients to be supine, which was part of the scanning protocol. The sonographic examination was completed by including transverse, longitudinal, and oblique scanning plane images. After consenting participants, based on inclusion-exclusion criteria, GA was recorded and used as a basis for the fetal biparietal diameter (BPD), femur length (FL), and abdominal circumference (AC) measurements. Their measurement parameters were made from the grayscale sonographic images, made in the longitudinal and transverse scan planes (See Figure 1). Doppler of the UV was done to record UV velocity and blood flow volume. UC diameter and velocity measurements were made at the fetal intra-abdominal region and the Doppler angle was kept below 60° of insonation (See Figure 2).

A transverse fetal sonogram that was captured on a 27-year-old participant, in the third trimester of pregnancy. The umbilical vein diameter was measured at 7.8 mm (See the blue arrows).
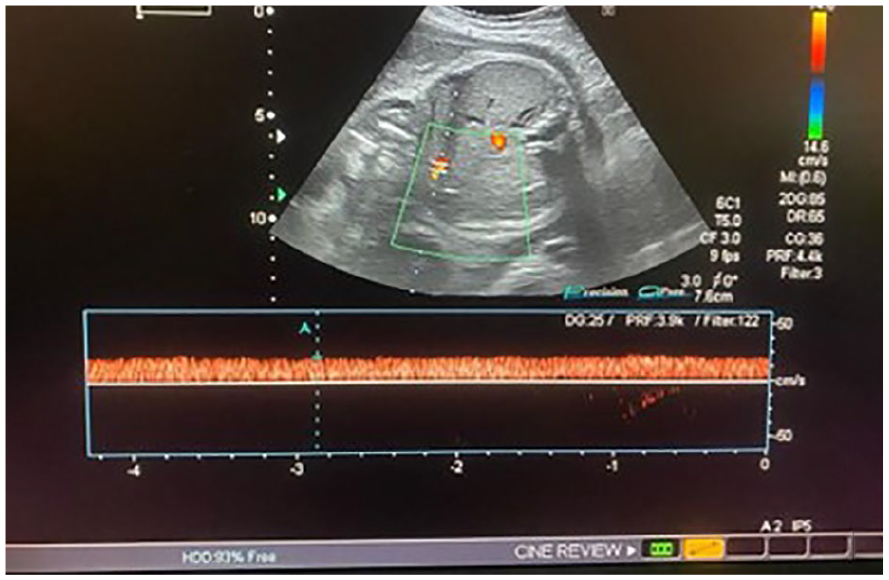
A duplex image demonstrates the spectral Doppler recording of the blood flow velocity. The waveform was recorded in the fetal umbilical vein, at 30 weeks gestation age.
Data Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) software version 25 (IBM Corp, Armonk, New York). The frequency, mean, and standard deviations (± SD) were calculated for quantitative variables (e.g., FW, GA, BPD, AC, FL, UV velocity, UV diameter, and blood flow volume). A Pearson correlation was used to determine the level of association between variables and the statistical significance was set at p < .05. Scatter plots were also generated as part of determining the strength of association.
Results
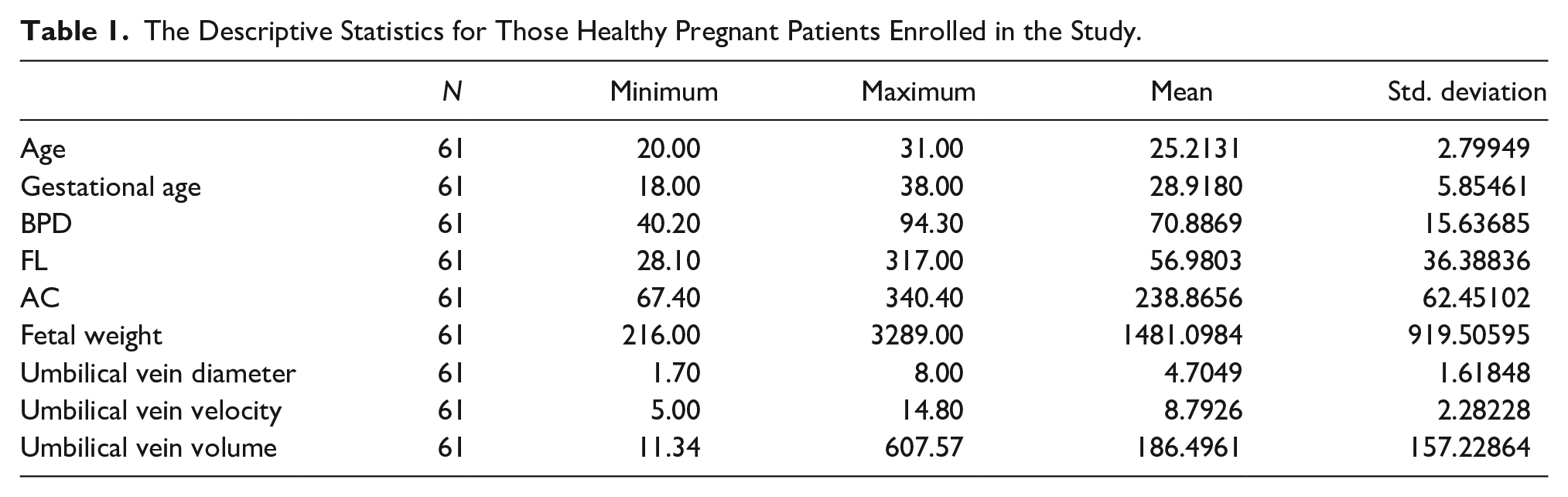
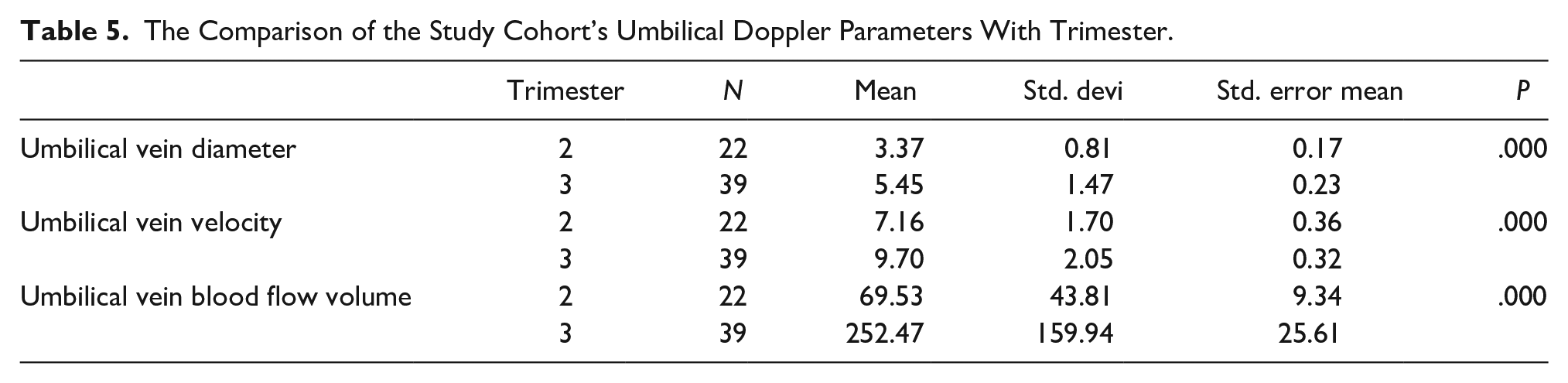
Based on the cohort of 61 participants, the mean age of the patients was 25.2 ± SD 2.79. The GA varied from 18.00 to 38.00 weeks, with a mean gestational age (GA) of 28.9 ± SD 5.8. The mean BPD was 70.88 ± SD 15.63. The mean FL was 56.98 ± SD 36.38. The AC varied from 67.40 to 340.40, with a mean AC of 238.86 ± SD 62.45. FW ranged from 216.00 to 3289.00 g, with a mean FW of 1481.09 ± SD 919.50 g. The diameter of the UV ranged from 1.70 to 8.00 mm, with a mean diameter of 4.70 ± SD 1.61 mm. The mean UV velocity was 8.79 ± SD 2.28, and the mean volume of the UV was 186.49 ± SD 157.22 mm (See Table 1). The GA showed a strong positive correlation with the UV diameter (r = .772, p < .001), UV velocity (r = .687, p < .001), and UV volume (r = .732, p < .001). The UV diameter demonstrated a strong positive correlation with UV velocity (r = .593, p < .001) and an even stronger positive correlation with UV volume (r = .928, p < .001). The UV velocity showed a strong positive correlation with UV volume (r = .754, p < .001). These findings may suggest that as GA increases, there are corresponding increases in UV diameter, velocity, and volume (See Table 2, Figures 3–5). FW indicated strong positive correlations with UV diameter (r = .756, p < .001), UV velocity (r = .673, p < .001), and UV volume (r = .738, p < .001). The UV diameter showed a strong positive correlation with both UV velocity (r = .593, p < .001) and UV volume (r = .928, p < .001). The UV velocity demonstrated a strong positive correlation with UV volume (r = .754, p < .001). These findings may suggest that FW is positively associated with UV parameters, indicating that as FW increases, there are corresponding increases in UV diameter, velocity, and volume (See Table 3, Figures 6–8). FW also showed a very strong positive correlation with BPD (r = .962, p < .001) and a strong positive correlation with AC (r = .816, p < .001). A moderate positive correlation was noted with FL (r = .536, p < .001). BPD indicated a very strong positive correlation with both FW (r = .962, p < .001) and AC (r = .854, p < .001). It also showed a moderate positive correlation with FL (r = .505, p < .001). FL also demonstrated a significant positive correlation with FW (r = .536, p < .001) and BPD (r = .505, p < .001), but an insignificant correlation with AC (r = .004, p = .977). These results may indicate that FW has very strong associations with BPD and AC and a moderate association with FL, while BPD and AC also had a very strong correlation between them (See Table 4). In the second trimester, the mean UV diameter was 3.37 ± SD 0.81, and the mean UV velocity was 7.16 ± SD 1.70 cm/s. In addition, the mean UV blood flow volume, in the second trimester, was 69.53 ± SD 43.81 mL/min comparatively, in the third trimester, these values increased significantly. The mean UV diameter rose to 5.45 ± SD 1.47, UV velocity increased to 9.70 ± SD 2.05 cm/s, and UV blood flow volume surged to 252.47 ± SD 159.94 mL/min. The p-values for all comparisons were statistically significant (p < .001), indicating a significant difference in this cohort’s UV parameters between trimesters (See Table 5, Figures 9–11).
The Descriptive Statistics for Those Healthy Pregnant Patients Enrolled in the Study.
The Strength of Association Between the Study Cohort’s Gestational Age Compared With Umbilical Doppler Parameters.
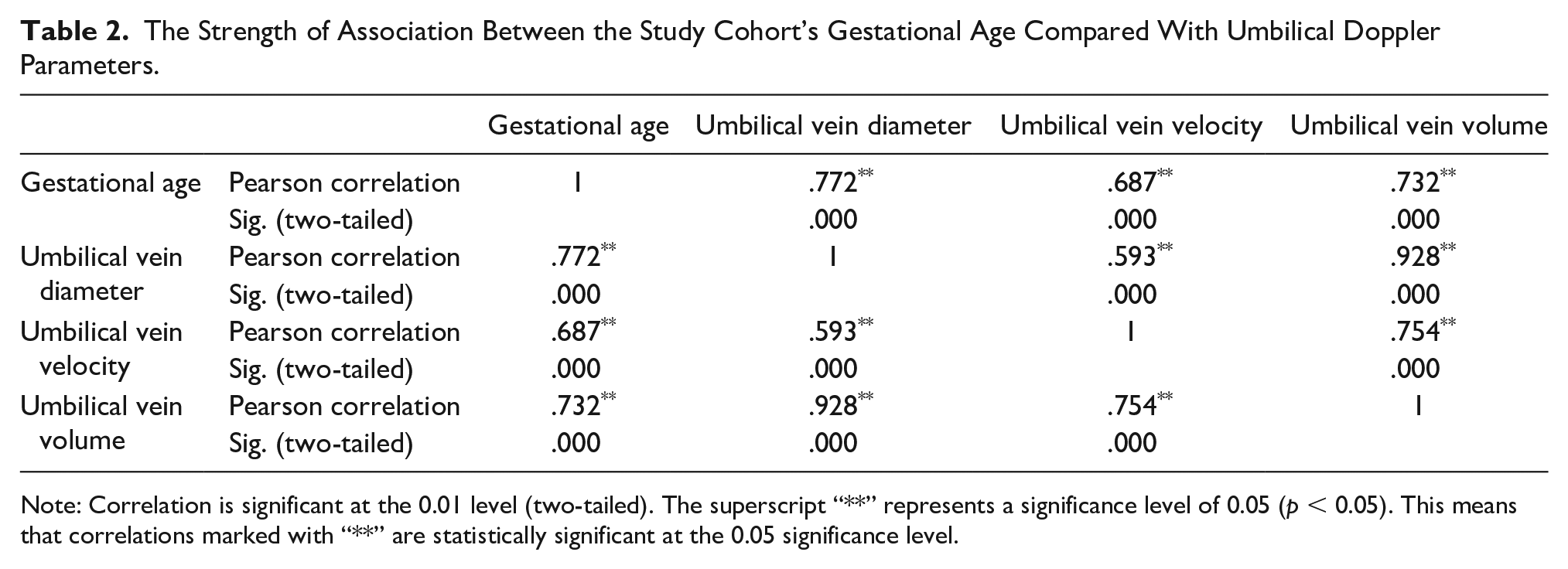
Note: Correlation is significant at the 0.01 level (two-tailed). The superscript “**” represents a significance level of 0.05 (p < 0.05). This means that correlations marked with “**” are statistically significant at the 0.05 significance level.
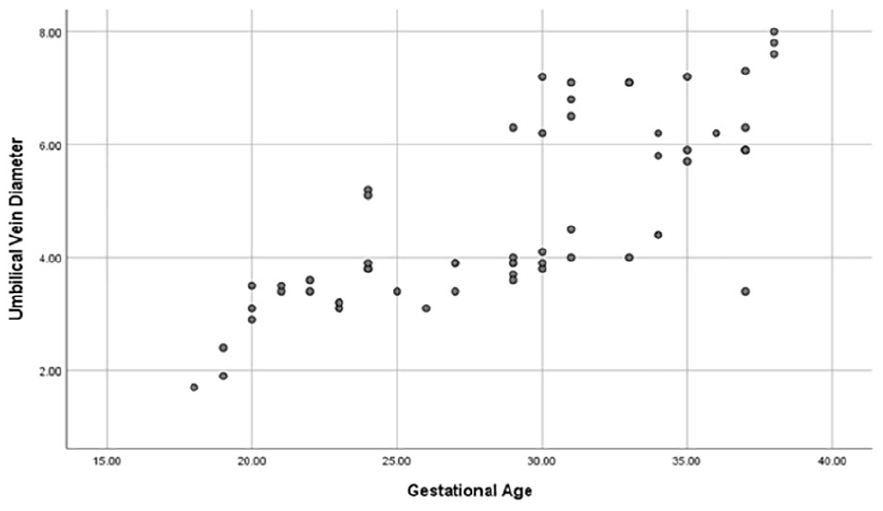
A scatter-plot diagram plotting gestational age and umbilical vein diameter data.
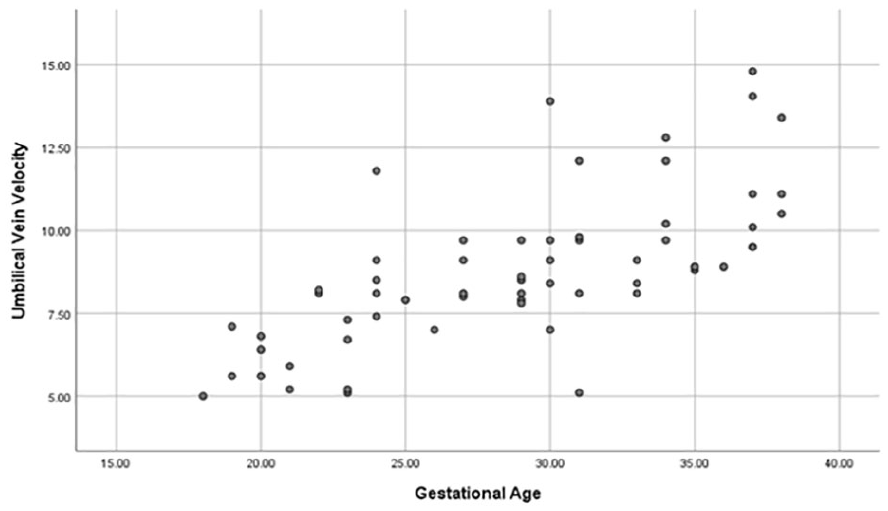
A scatter-plot diagram plotting gestational age and umbilical vein velocity data.
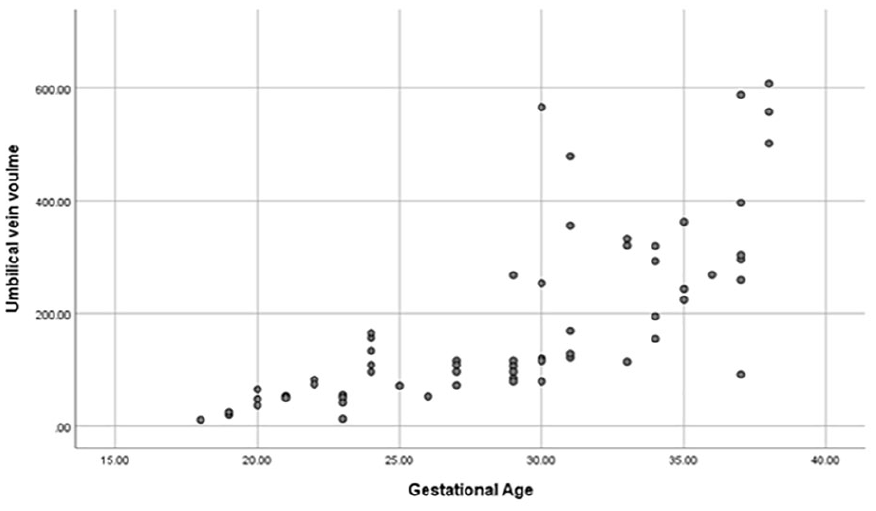
A scatter-plot diagram plotting gestational age and umbilical vein volume data.
The Strength of Association Between the Study Cohort’s Fetal Weight With Umbilical Doppler Parameters.
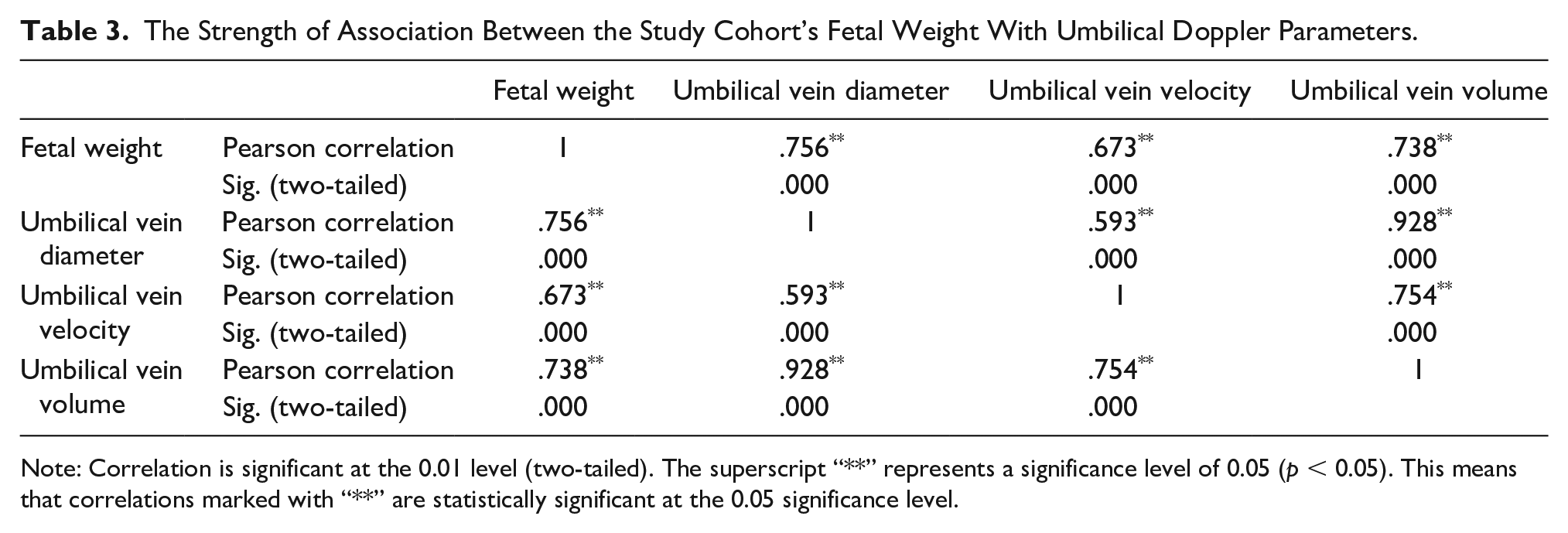
Note: Correlation is significant at the 0.01 level (two-tailed). The superscript “**” represents a significance level of 0.05 (p < 0.05). This means that correlations marked with “**” are statistically significant at the 0.05 significance level.
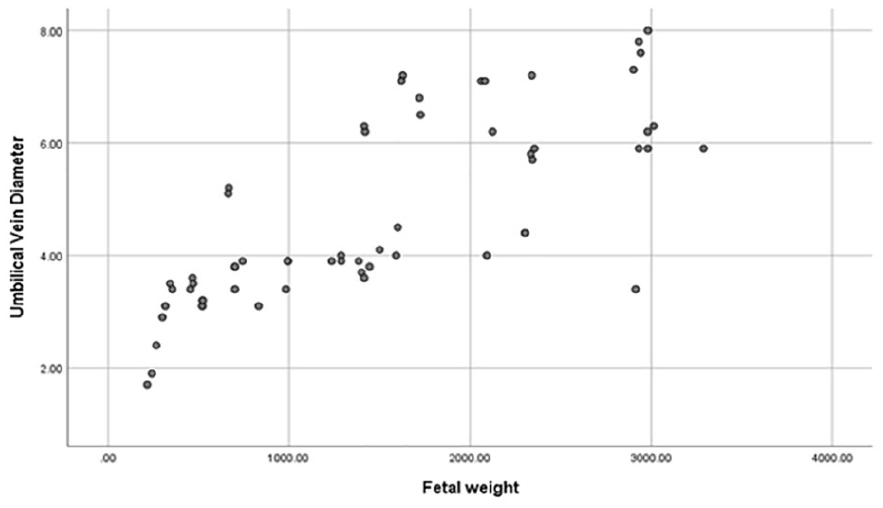
A scatter-plot diagram plotting fetal weight and umbilical vein diameter data.
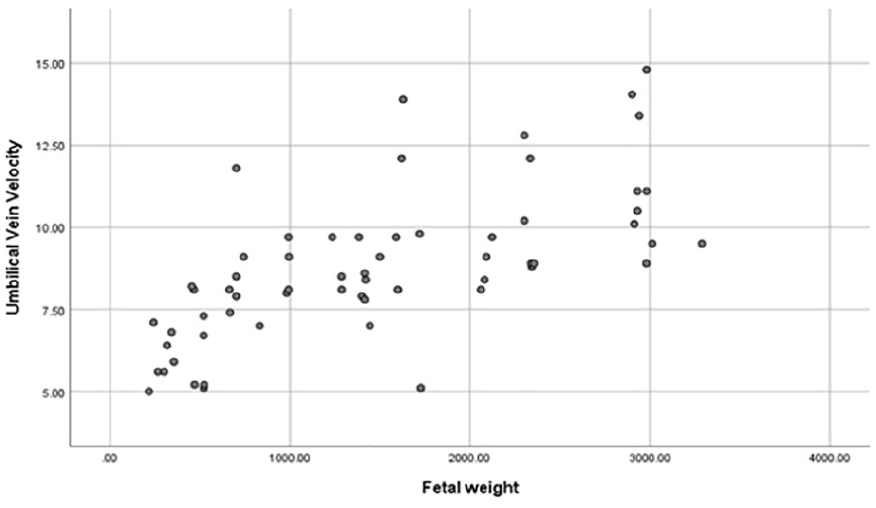
A scatter-plot diagram plotting fetal weight and umbilical vein velocity data.
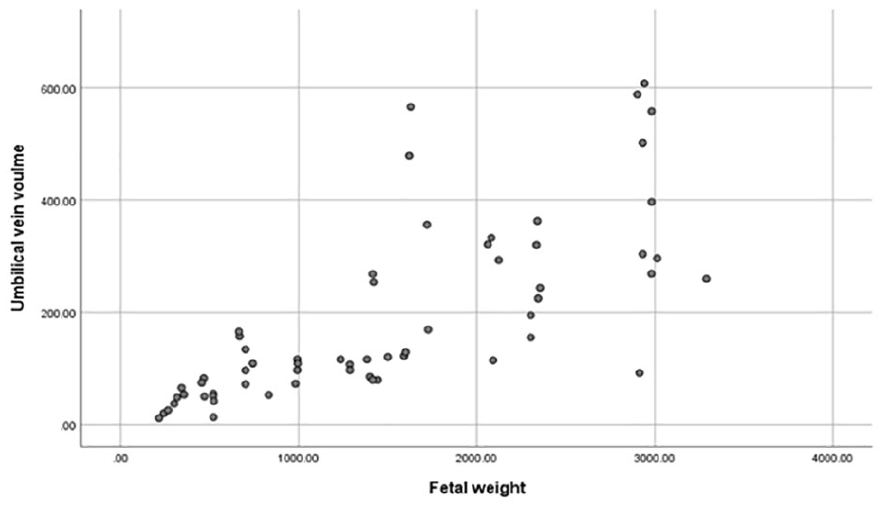
A scatter-plot diagram plotting fetal weight and umbilical vein volume data.
The Strength of Association Between the Study Cohort’s Fetal Weight With BPD, FL, and AC.
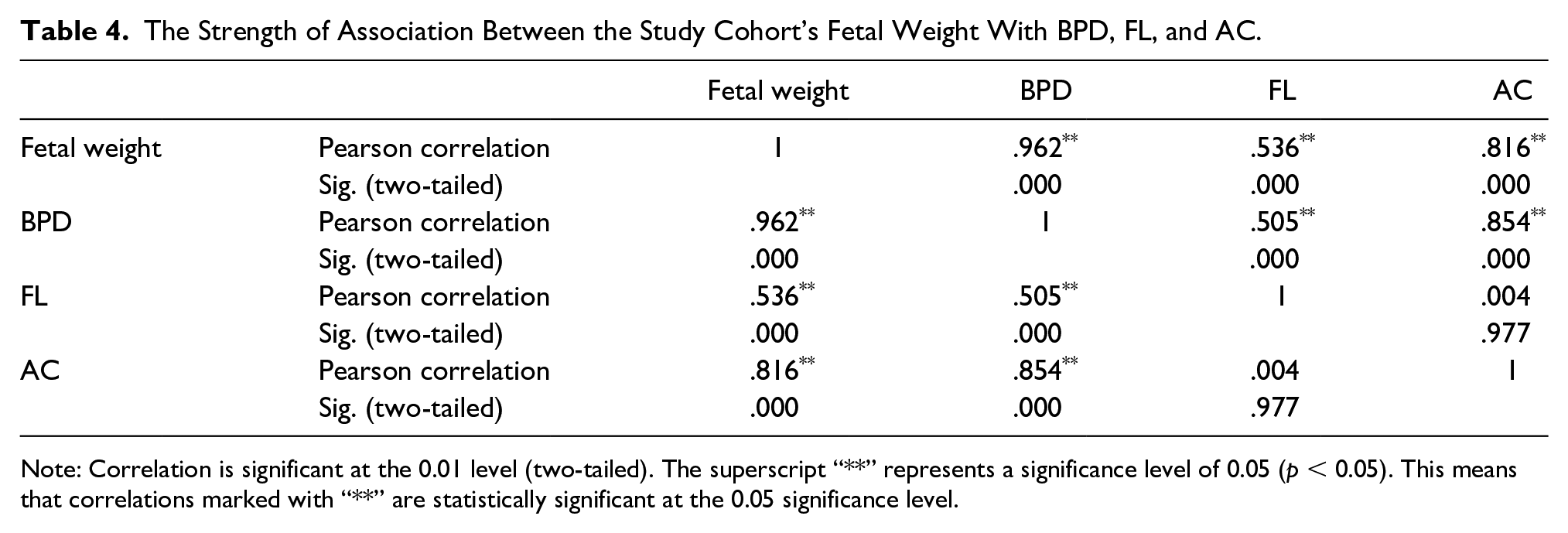
Note: Correlation is significant at the 0.01 level (two-tailed). The superscript “**” represents a significance level of 0.05 (p < 0.05). This means that correlations marked with “**” are statistically significant at the 0.05 significance level.
The Comparison of the Study Cohort’s Umbilical Doppler Parameters With Trimester.
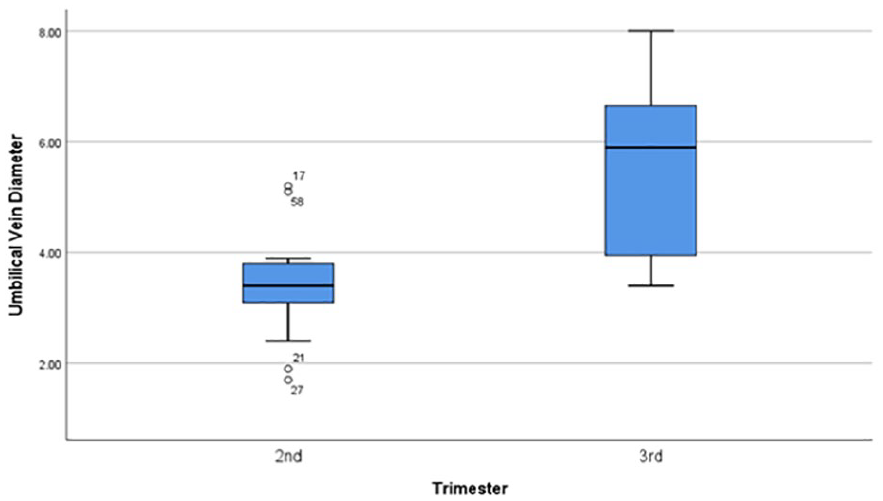
A box-plot diagram to demonstrate the mean comparison of umbilical vein diameter in the second and third trimester of pregnancy.
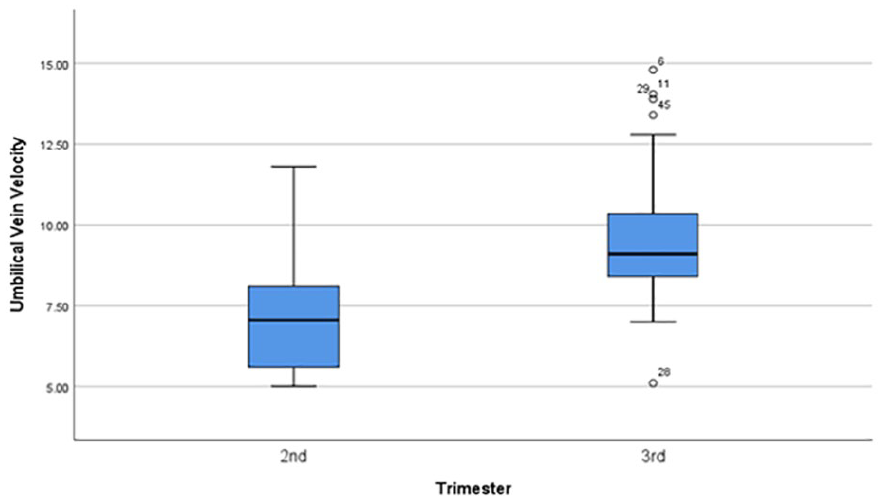
A box-plot diagram to demonstrate the mean comparison of umbilical vein velocity in the second and third trimester of pregnancy.
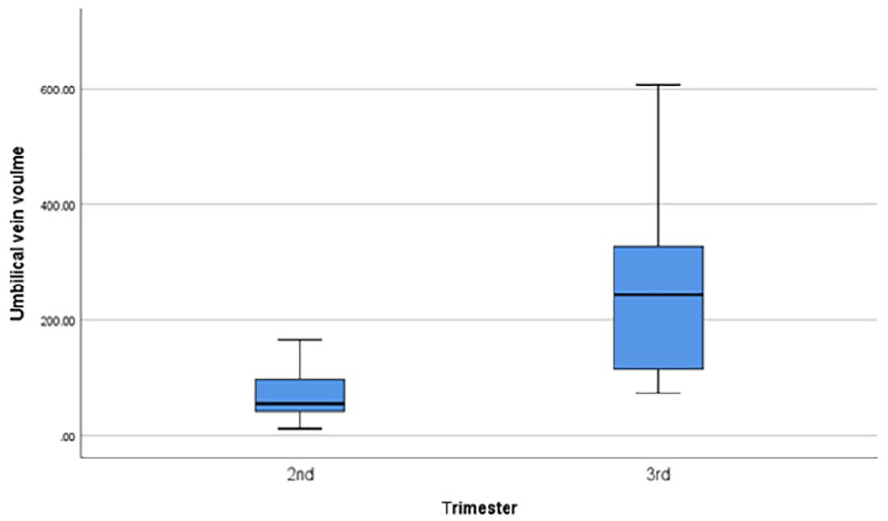
A box-plot diagram to demonstrate the mean comparison of umbilical vein volume in the second and third trimester of pregnancy.
Discussion
The current study showed the correlations observed between GA, FW, and UV parameters, which provided valuable insights into the dynamic changes that may occur in fetal circulation, during pregnancy. The strong positive correlations between this cohort’s GA and UV diameter, velocity, and volume may suggest a progressive increase in these parameters, as pregnancy progresses. This indicates a natural adaptation of the fetal circulatory system to meet the growing metabolic needs of the developing fetus. Similarly, the strong positive correlations between FW and UV parameters imply that fetal growth may be closely linked to UV hemodynamics. As the fetus gains weight, there is a corresponding increase in UV diameter, velocity, and volume, reflecting enhanced blood flow to support the growing fetus.
A study conducted in 2022, reported a mean UV diameter at 20 and 40 weeks’ gestation, which was 0.51 ± SD 0.03 and 0.91 ± SD 0.03 cm, respectively, showing a gradual increase in mean UV diameter as GA increased. 13 The mean UV diameter also increased gradually, in that study cohort, along with the estimated FW. There was a very strong, positive, and significant relationship between UV diameter and GA (r = .63, p = .001) and between UV diameter and estimated FW (r = .57, p = .001). 13 This is in comparison to the current study cohort that demonstrated FW had a strong positive correlation with UV diameter (r = .756, p < .001). Köşüş et al 14 observed similar findings of a significant correlation between UV diameter and estimated FW. In that study, they demonstrated that up to 34 weeks of gestation, UV diameter increased linearly before the data plateaued. They concluded that UV diameter might be helpful for predicting estimated FW under 34 weeks, based on their findings. 14 Conversely, Tutus et al 15 found that UV diameter and estimated FW had an inverse association, but they were unable to provide a pathophysiological explanation for their findings. A study by Spurway et al 16 reported that the diameter of the UV increased from 4.1 mm at 20 weeks to 8.3 mm at 38 weeks gestation. Their results showed that all three parameters of the UV were increased with GA, and their results are like the current study results. Another study found that UV flow increased with GA. 17 A study by Polin et al 18 provided data that indicated both UV diameter and the mean velocity increased during gestation.
Umbilical venous flow volume (UVFV) measured using sonography can be used to assess placental circulation in a fetus. A study by Ozawa revealed that with increasing gestational weeks, UVFV increased, while UVFV per estimated FW decreased slightly. 19
Because placental blood flow and systemic circulation changes in cases of IUGR, it was observed that UVFV was diminished in those conditions.20,21 Under these conditions, UVFV decreases, indicating changes in the placental circulation. According to Naro et al, 21 there was a decrease in UVFV in fetuses with IUGR compared with those with normal pregnancies; however, there was no significant difference in the pulsatility index of UA flow, between these groups.
The findings of the current study highlighted the importance of monitoring UV parameters, during pregnancy, as indicators of fetal well-being and development. Understanding the relationships between GA, FW, and UV parameters can aid in the assessment of fetal growth and guide clinical management decisions to optimize maternal and fetal outcomes. The potential impact of the current study could be important for patients with maternal hypertension. It is well described that according to Poiseuille’s law, the biggest effect on flow is diameter, as the radius is the fourth power in that equation. It is also well known that the flow volume in fetal circulation goes from approximately 50–500 mL, in the third trimester. Future research should include patients with pregnancy-induced hypertension to see the difference in diameter in the UV.
Limitations
This study has specific limitations due to the research design and threats to internal and external validity. The research was statistically powered but given the convenient sampling makes these study results specific to this cohort of patients. This work cannot be generalized beyond this cohort of patients.
Conclusion
The current study of this cohort of patients found strong, positive, and significant correlations between UV Doppler indices, GA, and FW. These research findings highlight the dynamic nature of fetal circulation and its adaptation to meet the growing metabolic demands of the developing fetus. Monitoring UV parameters may offer valuable insights into fetal well-being and growth, aiding in the assessment of fetal health and guiding clinical management decisions, during pregnancy.
Footnotes
Author’s Note
Khaled Jallad is also affiliated to Radiography & Medical Imaging, Fatima College of Health Sciences, United Arab Emirates.
Ethics Approval
Ethical approval for this study was obtained from the Research Ethical Committee, The University of Lahore (IRB # REC-UOL-518-09-2023).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.