
Abstract
Objective:
The aim of these analyses was to determine the potential development of increased carotid intima-media thickness (cIMT) and spectral Doppler velocity in a cohort of children who were eligible for federal nutrition support services.
Materials and Methods:
A secondary data analysis was conducted based on data collected during a larger randomized clinical trial. Data were pulled on 108 children, ages 8 to 11 years, who had both cIMT measures, as well as spectral Doppler data, at the level of measured intimae. Additional data such as vessel geometry, body mass index (BMI), and blood pressure (BP) were added to the analysis to provide additional descriptive data.
Results:
The posterior cIMT data provided the best visualization and measurements to assess the presence of early risk for atherosclerosis. In this cohort of 8- to 11-year-olds, the median spectral Doppler values did not exceed the published values for these ages, nor did their systolic blood pressure. In this group, 77 (71%) were classified as having a healthy BMI. However, the posterior cIMT data were compared to published measures of pediatric cIMT values and 60 children (55%) exceeded the expected mean thickness of 0.38 mm + 0.04 on the right and 58 (53%) on the left.
Conclusion:
The use of spectral Doppler to assess the risk of developing atherosclerosis may not be the best diagnostic tool, based on this cohort. The measurement of cIMT has the most promise to proper classify healthy appearing 8- to 11-year-olds, for early signs of diminished cardiovascular health.
Keywords
Many global health initiatives have been identified for children and chief among them is cardiovascular health (CVH). As an example, Healthy People 2030 has goals to reduce cardiovascular disease in adults and reduce obesity in children, especially for children with social determinents.1,2 These goals are inextricably tied together, as it is important to address early risk factors that contribute longitudinally to the development of cardiovascular disease. One suggested method to promote CVH is including it as part of an annual general wellness check. As part of the general wellness check, providing messaging aimed at both parents and children concerning atherosclerotic risk factors is made easier by emphasizing how to improve CVH. 3 Having medical providers engaging with parents and children about CVH and ways to improve their risks, allows for conversations to be less focused on obesity and more inclusive of factors such as sleep, diet, physical activity, and smoking/vaping.3,4 Moving medical providers to have more inclusive discussions that will improve CVH early in childhood and continuing as an adult is a holistic strategy, but diagnostic testing is important to measure success. After the ages of 9 to 11 years, universal screening for fasting glucose and cholesterol has been rapidly adopted and recommended as a part of the American Academy of Pediatrics’ Bright Future Guidelines. 5 What is lagging is the type of diagnostic testing that would assess early development of plaque and risk for vascular compromise. While several blood tests exist, the use of sonography, a non-invasive and non-ionizing diagnostic examination, could be an important factor in assessing a child’s CVH. Trihan et al. 6 worked to record Doppler measurements for pediatric patients based on age, height, and weight. However, these measurements were not tied to clinical outcomes. Empirical evidence for the use of Doppler is lacking given that many providers feel that pediatric patients are unable to tolerate prolonged diagnostic examinations. An additional method for assessing early atherosclerotic disease is measuring the carotid artery intima-media thickness (cIMT). Rarely are diagnostic assessments completed on children however, a study of type-1 diabetic children captured cIMT measurements, which were compared to normal controls. The results of that study demonstrated that when comparing 52 diabetic patients to 47 controls, the cIMT measurements were increased among those diabetics, but with lower Doppler velocities. 7 Interestingly, in a large study conducted with 11- to 13-year-old children who had obesity, they found that female children demonstrated a significant association between measured cIMT and obesity. 8 However, the males did not show the same statistical significance.
Based on some of the available published evidence, the use of spectral Doppler to measure carotid velocity and cIMT is worth exploring as a screening technique for children, to assess CVH. Despite some of these early studies, there is a paucity of data measuring cIMT, Doppler, and clinical outcomes in school age children, including in those from historically underserved households. The objective of this study was to assess children who resided in low-income neighborhoods qualifying for federally funded nutrition support programs and to determine the early presence of atherosclerosis and determine the associations with Doppler and CVH outcomes. Therefore, the research question was:
Materials and Methods
Study Design and Participants
For the purposes of this study, a convenience sample of participants was prospectively examined, as part of a 5-year randomized control trial (RCT #NCT05367674). Participants for the main RCT were recruited from the local intercity public school system and had to be eligible to participate in federally funded nutrition programs. This study was approved by The Ohio State University’s Internal Review Board (Biomedical IRB #2017B0110) and required a parent/guardian’s written consent and their child’s assent to participate in the study. Children were ineligible if they were unable to participate in physical activities, did not speak English, were diagnosed with metabolic, digestive illnesses, or diagnosed with mental, and/or physical disabilities that would impair their participation in the study. The consented cohort included 192 children aged 8 to 11 years. Participants from two years of this study were included in this sub-analysis if the children had gray-scale sonography, cIMT measures, and spectral Doppler completed.
Sonography Protocol
All exams were performed with the same ultrasound equipment system by two trained vascular sonographers. Imaging and analysis were executed using a GE Logiq i laptop ultrasound system (GE Healthcare, Inc. Milwaukee, Wisconsin), which has been optimized for high resolution. The equipment chosen was highly portable and provided easy accessibility in small spaces and exam rooms. The type of equipment being used also reflected what may be available to physicians and outpatient sites in a genuine clinical setting. A high-frequency linear (7-12 MHz) transducer was used. Participants were asked to lay in the supine position with their head slightly hyperextended and rotated 45° away from the artery side being examined (See Figure 1). 9 Because a cIMT measurement software did not exist on the equipment, all measurements were made post-examination. To ensure harmonization between participants, the measurement protocol was adapted from an updated document from the Mannheim IMT consensus. 10 This update seeks to address the importance of standardized cIMT measurements: “Further advancement for the field of IMT requires standardized methods, enabling homogenous data collection and analysis. This may help to improve the power of such studies and to facilitate the merging of large databases for meta-analyses.” 10 The transducer was placed directly on participants’ lateral neck with minimal pressure, to ensure no compression of the vessel. Images of the common carotid artery (CCA) to the bifurcation were imaged, as well as the proximal portion of the external carotid artery (ECA) and internal carotid artery (ICA). Imaging was repeated on both the right and left carotid artery. Measurements of the cIMT were made of the anterior and posterior carotid intimae (See Figure 2). The posterior measurements were prioritized, as it offered the best image quality. Prioritizing the posterior cIMT is also stressed in the Mannheim IMT consensus, noting that the anterior wall measures offer less reliability. 10 A process of interobserver checks were made on all cIMT measurements, to provide added confidence in the data. In addition, bilateral spectral Doppler waveforms were taken in the same location as the cIMT measurement, approximately 1.5 cm from the bulb of the carotid artery (See Figure 3). The spectral Doppler tracing was obtained with angle correction that was ≤60° and parallel to flow. All spectral tracings were closely supervised by the principal investigator (PI), and a peer-review process was also used to select the waveform for data analysis (See Figure 4). The cIMT measures were made on a computer with Image J software. The peak systolic and end diastolic endpoints were found using the auto trace function but often the end diastolic endpoint had to be manually adjusted for a proper data endpoint.
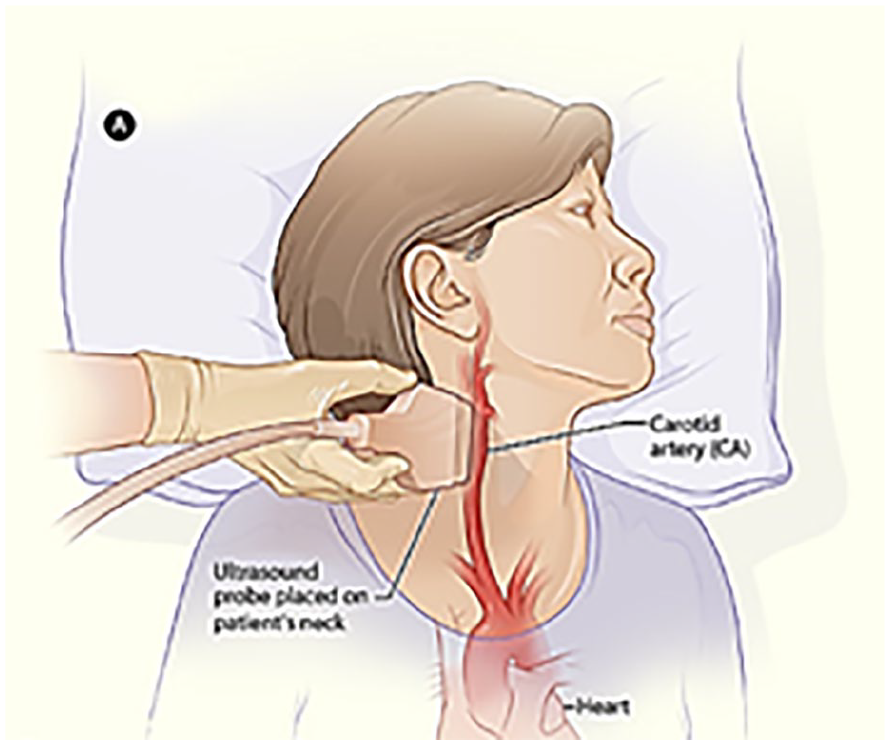
An illustration of the participant’s positioning to examine the carotid arteries.
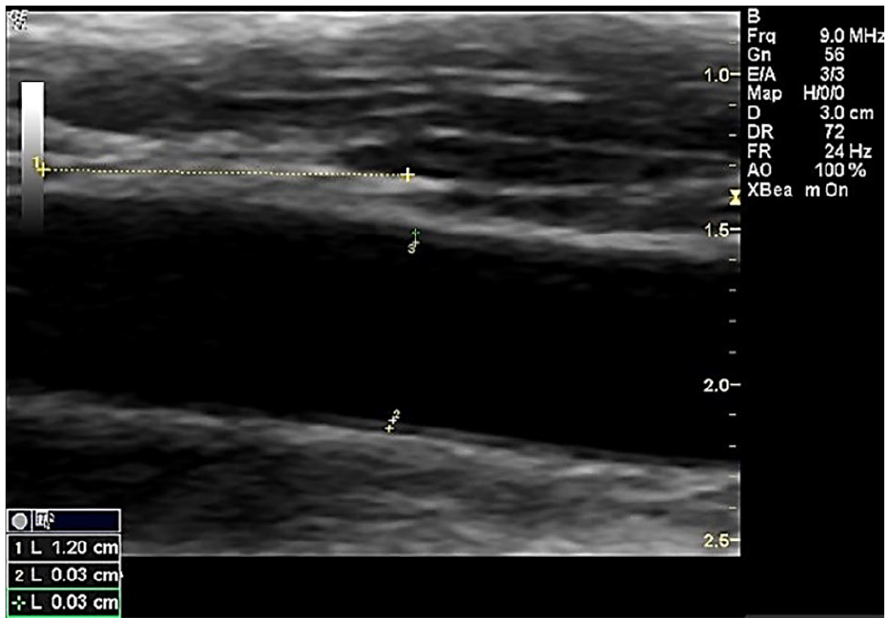
A sonographic image that demonstrates the cIMT measurement. cIMT is the abbreviation for carotid intimal media thickness. Cursors are placed longitudinally to indicate the segment distal to the carotid bulb.
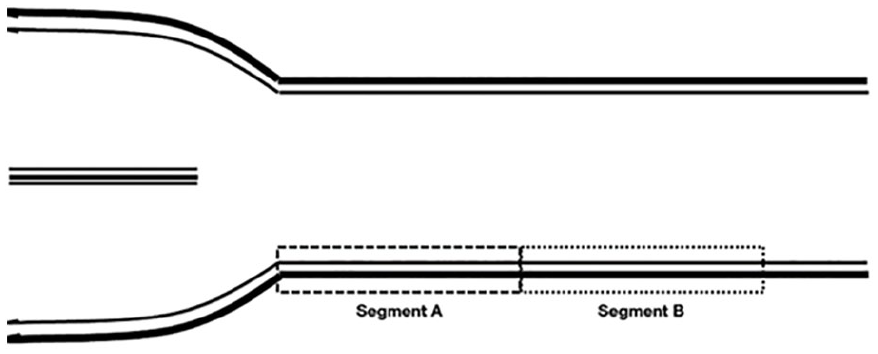
A diagram of the common carotid artery segments to allow for repeated measurements of velocity. All study measurements were made in segment A, which is usually 1.5 cm from the carotid bulb.
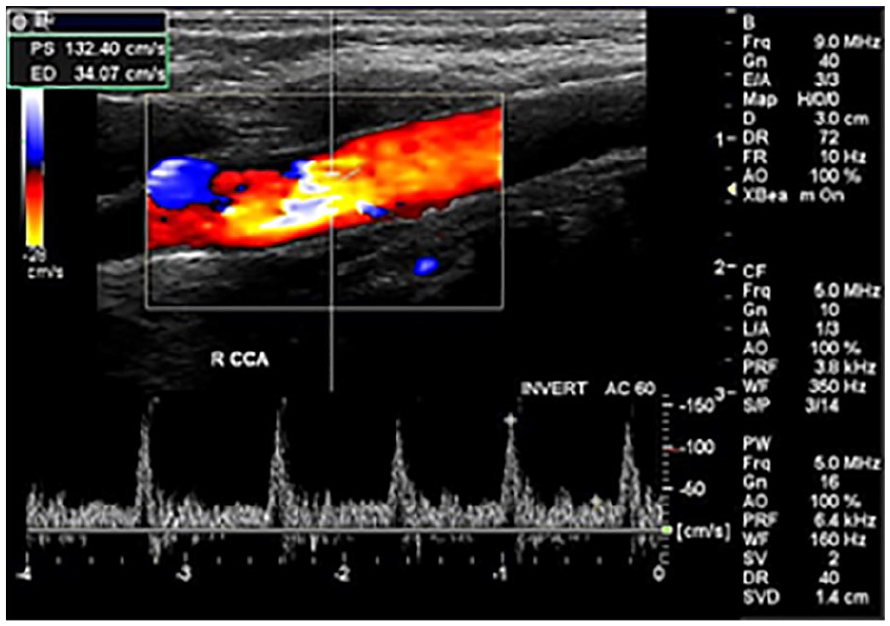
Triplex Doppler examination of a pediatric participant, who demonstrated high velocity flow in segment A, proximal to the distal common carotid artery. Spectral waveforms were attempted to quantify the velocity, which was not routinely noted in this cohort with color or spectral Doppler.
Vessel geometry was important to allow for comparison across the age categories and sex. 11 The length of the carotid was measured from the bulb to subclavian or aortic arch, and the vessel area was derived using vessel diameter.
Demographic and Cardiovascular Health Measures
Patient characteristics including height and weight measures were collected by trained medical staff and were used to calculate the child’s body mass index (BMI) percentile, based on the US Center for Disease Control’s (CDC) growth charts for children. 12 In addition, each participant had their blood pressure measured using an automated blood pressure cuff following standardized research protocols.
All children were seated with a both feet on the ground, the arm relaxed, and at heart level. All measures were taken from the right arm unless significant clinical reasoning prevented pressure to be taken on this arm. 13 In these cases, blood pressures were taken from the left arm and proper documentation was made.
Data Analysis
This study was a secondary data analysis of the main RCT. The process for curating the participant data was conducted using the process outlined in Figure 5. As such, it was not powered to detect statistically significant differences. Descriptive statistics (frequency and percent for categorical variables and medians, inter-quartile range, minimum and maximum for continuous variables) were used to summarize subject demographics and CVH characteristics, by age. The CCA peak systolic velocity (PSV), end diastolic velocity (EDV), CCA length, and CCA vessel area were summarized by cIMT measures of the carotid artery, left and right separately. Descriptive data were compared to the published works that provided norms for vessel geometry, cIMT, and spectral Doppler velocities, in this age group.6,14,15 All data analysis were conducted using SAS Statistical Software (Cary, North Carolina). The p-value of .05 was chosen a priori for statistical significance.
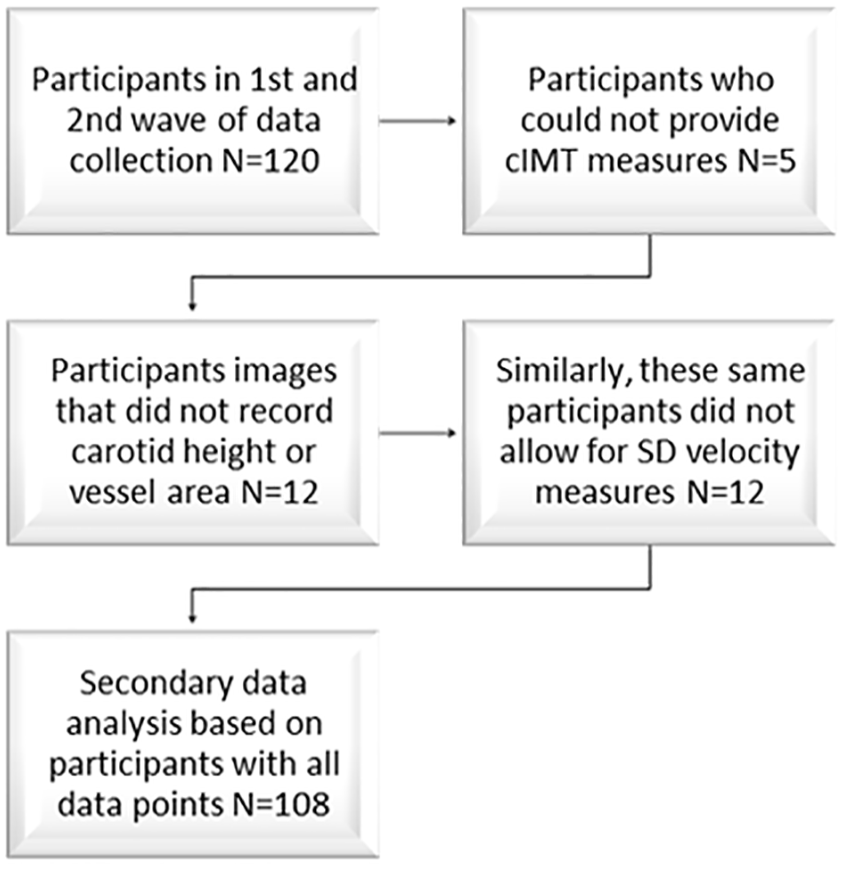
CONSORT diagram that outlines the participants who were consented but had all the data points necessary to conduct the secondary data analysis.
Results
A total of 120 participants (out of the cohort of 192) were examined for cIMT; however, based on missing data for this sub-analysis, only 108 children had all the data necessary to run the full analysis (See Figure 5). The final cohort was comprised of 46 males (39%) and 71 females (61%). The median age of this cohort was 9 years of age, and the median BMI percentile was 79 (min 3.0, max 99.6). For those participants who provided cIMT measures, the median right CCA anterior cIMT was 0.40 mm (min 0.20; max 0.70). The cIMT measures for the right CCA posterior vessel wall was 0.50 mm (min 0.30; max 0.70). The left mean CCA anterior cIMT was 0.40 mm (min 0.30; max 0.70). The cIMT measures for the left CCA posterior vessel wall were 0.50 mm (min 0.30; max 0.70). To properly normalize the data for analyses, the vessel length and area were taken from those participants who contributed all the data points. The median vessel length of the left CCA was 5.9 mm (min 5.0; max 7.2). The median vessel length of the right CCA was 6.0 mm (min 4.5; max 7.4). The median left CCA area of the vessel, where the cIMT measures were taken, was 2.7 mm2 (min 2.0; max 4.1). The median vessel area of the right CCA was 2.8 mm2 (min 1.6; max 4.3). The spectral Doppler tracings and the data points of PSV and EDV were taken at the same place that the respective cIMT measures were made. The median PSV taken in the left CCA was 113.04 cm/s (min 59.62; max 181.37). The median EDV taken in the left CCA was 34.07 cm/s (min 18.04; max 54.39). The median PSV taken in the right CCA was 109.94 (min 62.91; max 175.95). The median EDV taken in the right CCA was 32.52 cm/sc (min 9.29; max 49.94). The left and right carotid arteries were analyzed separately due to their anatomical positions on the aortic arch and how other studies have handled this type of data. 11 It was important to review the distribution of the data by age and BMI categories 16 to make sure that all the data could be combined and fairly represented the cohort. The descriptive data are provided in Table 1. In addition, the demarked areas of segments A and B (See Figure 5) were important visual landmarks to ensure that spectral Doppler tracings were taken only in segment A. 11 In conjunction with this measurement, it was critical to make all measurements during systole, which was done using the cine function and scrolling to find the widest diameter, in conjunction with that phase of the cardiac cycle.
A Data Summary is Provided Based on the Ages of the Participants and Their Respective Body Mass Index Category, Right and Left Common Carotid Arteries (RCCA and LCCA), Vessel Height, and Vessel Diameters.
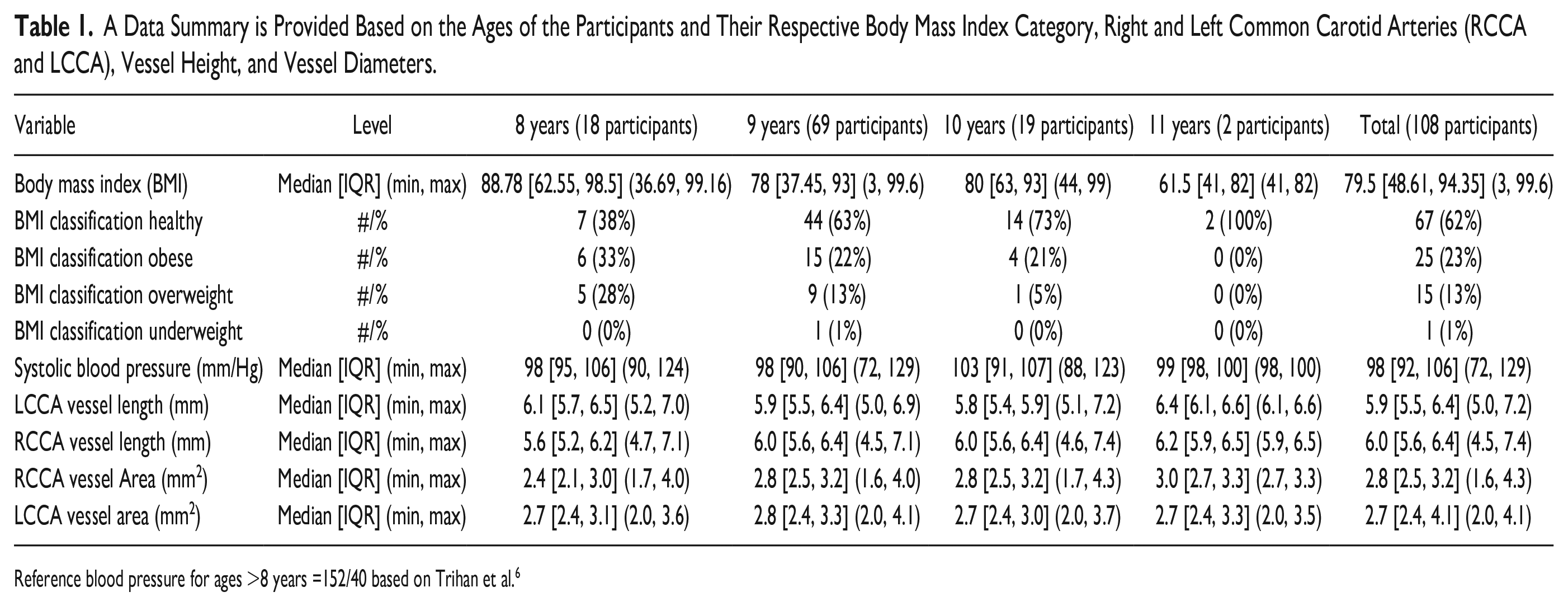
Reference blood pressure for ages >8 years =152/40 based on Trihan et al. 6
In addition, cIMT was summarized by age and the level of thickness (See Tables 2 and 3). As mentioned, the posterior cIMT was prioritized, as it was less prone to hand pressure and artifacts that could have diminished the anterior cIMT measurements. To further analyze the descriptive data, the posterior cIMT thickness levels were compared to vessel height, area, spectral Doppler velocities, PSV, and EDV, within both the left and right CCA (See Tables 2 and 3).
The Data Provided Summarizes the Data Collected on the Right Carotid Artery, Within the Study Cohort (N = 108).
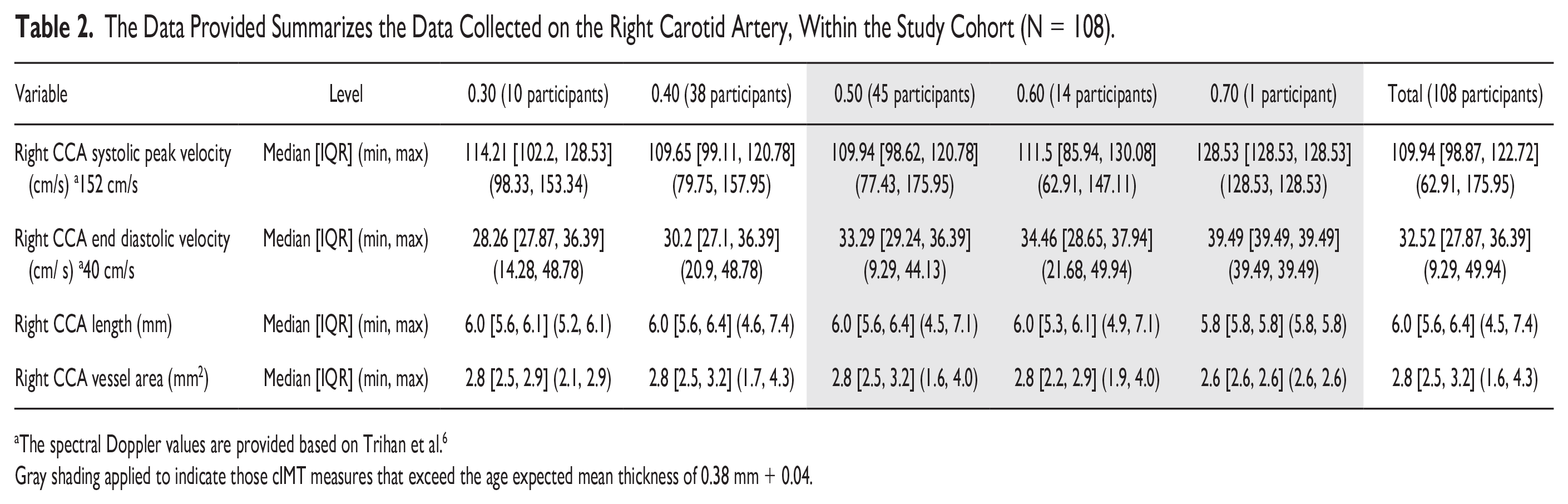
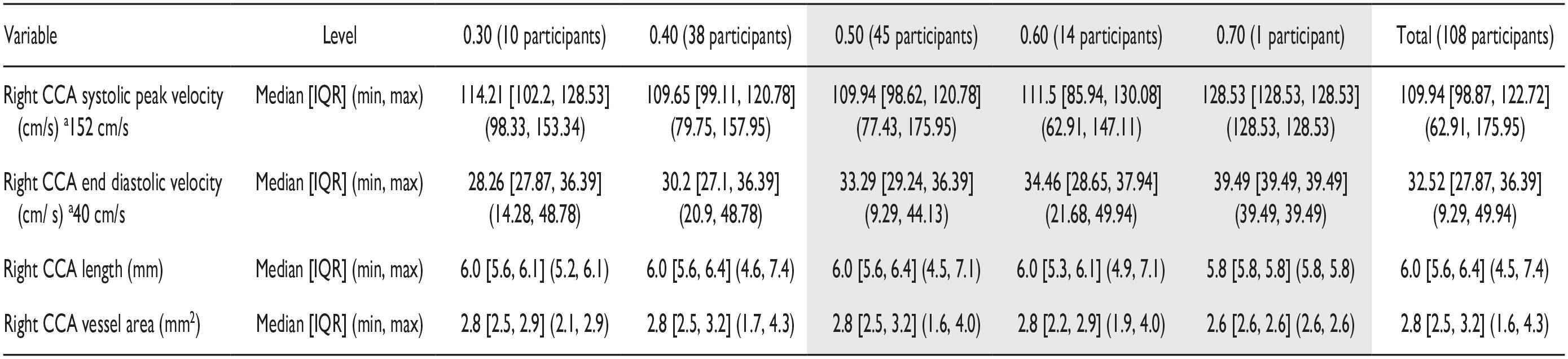
The spectral Doppler values are provided based on Trihan et al. 6
Gray shading applied to indicate those cIMT measures that exceed the age expected mean thickness of 0.38 mm + 0.04.
The Data Provided Summarizes the Data Collected on the Left Carotid Artery, Within the Study Cohort (N = 108).
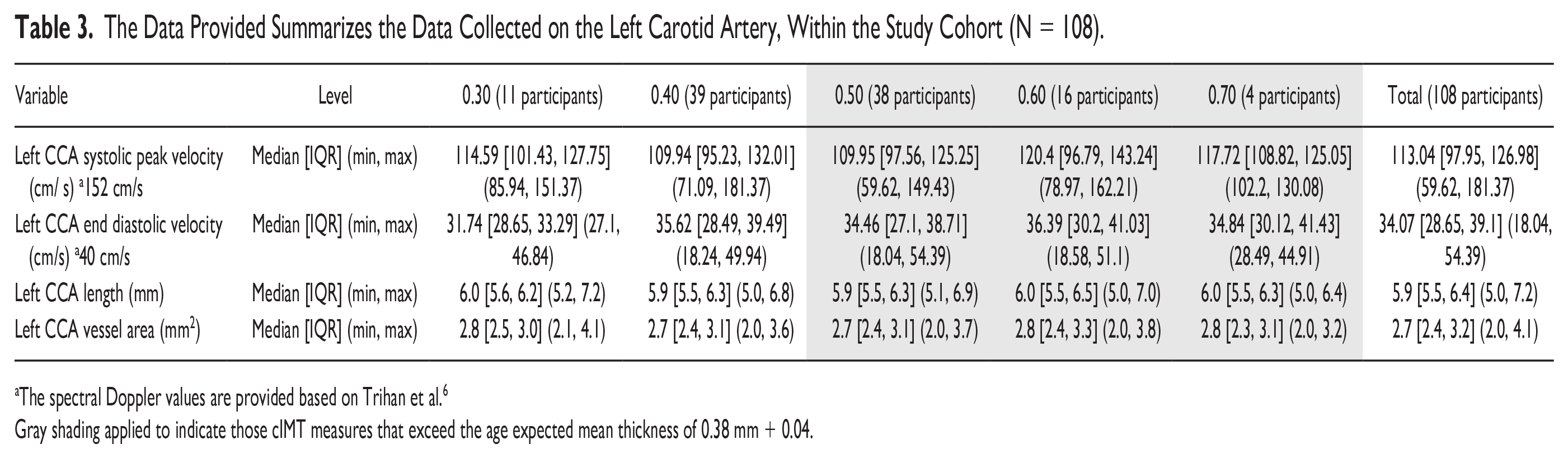

The spectral Doppler values are provided based on Trihan et al. 6
Gray shading applied to indicate those cIMT measures that exceed the age expected mean thickness of 0.38 mm + 0.04.
It was imperative to apply the guidelines provided by Jourdan et al., 14 as they identified cIMT measurements in healthy children, between the ages of 10 to 13.9 years as 0.38 mm ± 0.04, regardless of gender. In addition, the evidence published by Semmler et al. 14 and Jourdan et al. 15 would suggest that CCA diameter measurements in their cohorts as 4.99 mm ± 0.46 (males); 4.94 mm ± 0.42 (females) and a mean diameter of 5.45 ± 0.46. These reported parameters were applied to determine further data analysis.
Another important factor was to look at vessel length and area to make sure that the vessel geometry was comparable across the group and to ensure a proper comparison of the Doppler velocities. Reviewing these data was done using box plots and checking the normal distribution of the data (See Appendices A and B) QR CODE. This data was reviewed, in context, specifically in relation to the spectral Doppler analysis published by Trihan et al. In their work, they listed the PSV in the CCA of 3- to 9-year-olds as 152 cm/s + 29; EDV of 40 cm/s + 7; and PSV 142 cm/ s + 33 for 10- to 18-year-olds and EDV of 34 cm/s + 7.6. 6
In this healthy cohort of 8- to 11-year-olds, the median spectral Doppler PSV and EDV values did not exceed the published values for these ages nor did their systolic blood pressure. Of note was the fact that the posterior cIMT measurements exceeded 0.38 mm + 0.04 in 53% of the participants. In addition, based on BMI, only 36% of this cohort were classified as being either overweight or obese.
Discussion
The purpose of this sub-analysis was to determine the evidence of early signs of atherosclerosis and potentially impaired CVH, in a group of children residing in low-income neighborhoods and part of a cohort of a larger dietary intervention. The opportunity to collect spectral Doppler and cIMT data on these participants allowed for examining spectral Doppler, cIMT, and any evidence of pre-atherosclerotic disease, in pediatric carotid arteries. Surprisingly, in this study cohort, 62% were considered at a healthy weight; however, 37% had a BMI percentile classification of being either overweight or obese. These descriptive data may suggest that many of these children were successful in selecting supplemental food choices that are contributing to health and the fulfilling the program goals. 17 However, it is of equal concern that a percentage of this cohort was categorized as being overweight and/or obese at an early age (e.g., 8-9 years old). This study found that the median measurement of cIMT for this cohort was 0.50 mm. 6 This exceeds the previously published cIMT in a larger cohort of children, which was 0.38 mm ± 0.04. While standard measurements for children do not exist at this time, this is elevated and suggests that 33% of children demonstrated early evidence of thickening of the posterior cIMT and borderline anterior cIMT thickness. This allows for comparison with other cohort studies that have been conducted on the development of early development of atherosclerotic disease. One such study was work conducted by Meyer et al., which investigated cIMT thickness and flow-mediated vasodilation in 32 obese children compared to 20 normal controls. One limitation of that study was the age range of the obese participants was skewed to older children (9-16 years; median age 13.7; ± 2.11). 18 In their case-control study, obese participants had a mean cIMT (measured at the carotid bulb) of 0.53 mm ± 0.09; however, it was unclear whether these were anterior or posterior cIMT measures. 18 The control group of children had a mean cIMT (measured at the bulb) of 0.43 mm + 0.06, also unspecified as to anterior or posterior wall thickness. 18 Unfortunately, their results did not specify right versus left carotid artery measurements. Compared to this study, there were 60 participants (55%) who had cIMT measurements, bilaterally, and they were at or above the Meyer et al., obese and control cohort’s cIMT measurements. This is concerning as this study’s children are younger and had no signs of hypertension. The Meyer et al.’s study measured flow velocity within the radial artery, so this did not allow for a comparison of arterial flow to the present cohort. A more recent study case-control study of obese children (n = 71) by Jin et al. reported measured carotid artery stiffness with specialized software finding no statistical difference between right and left carotids, yet, the stiffness was statistically significantly higher in the obese group. 19 However, the ages were unspecified in these children other than consent was obtained for those participants who were older than 12 years. 19 Likely, this was an older cohort by comparison to this study based on the unpublished age ranges. In comparison, this study’s younger (8-9 years old) cohort presented with a higher-than-normal BMI in 8-year-olds (61%) and 9-year-olds (34%). However, their systolic blood pressure was 98 mmHg making this early prevalence of increased BMI not as clinically evident to be affecting CVH. In the present cohort, the fact that 62% were deemed, by BMI classification, to be of a healthy weight, but had bilateral cIMT posterior wall thickness greater than 0.5 mm was very surprising (e.g., 53% LCCA to 55% RCCA of the cohort). Given that the present cohort had this predilection to an increased bilateral cIMT posterior wall thickness, the participants flow velocities were below the Trihan et al.’s 6 values of 152/40 for those participants who were 8 years or older. In the present group, this may indicate that an increased bilateral cIMT posterior wall thickness had little influence on the carotid flow velocities. Regarding the research question, this cohort’s data would suggest that spectral Doppler did not demonstrate this early risk of developing atherosclerosis. This phenomenon was also seen in the Jin et al.’s 17 cohort, as their obese participants had bilateral mean Doppler pulse wave measurement that were not significantly correlated with obesity or cIMT stiffness. The concern would be that medical providers might rely solely on BMI, blood pressure, or spectral Doppler to determine which children are a risk for early development of atherosclerotic disease. In this cohort, it is possible that the cIMT is soft and pliable such that it is pushed back and does not yet inhibit the forward flow of blood through the vessel. This descriptive analysis of data suggests that further research is needed on the role that cIMT wall thickness plays in evaluating the CVH of pediatric patients.
Limitations
The major limitation to this study is the pre-experimental research design, which has threats to internal and external validity. The fact that this was a secondary data analysis of participants enrolled in an RCT made this work statistically underpowered and the sub groupings of participants resulted in an ability to conduct meaningful inferential statistics. There were also issues of not being able to get measurements on all of participants in this cohort. It also would have been advantageous to have had cIMT software to avoid making manually measurements. It is also important to note that newer forms of vascular flow detection (i.e., B-flow imaging and Power Doppler), as well as ultrasound contrast media could yield different results.
Conclusion
This study showed that cIMT and Doppler measures can be taken in children and that in our cohort, cIMT measures were elevated, without changes in Doppler velocity. As the CVH of children has become increasingly important, non-invasive and non-ionizing diagnostic tools are needed to assess the risk for diminished CVH. Given the prevalent use of cIMT and carotid sonography, these techniques could be applied to children. This secondary analysis suggests that for this cohort of 8- to 11-year-olds, cIMT was a better indicator of early atherosclerotic disease, despite the other normal screening values of spectral Doppler, BMI, and blood pressure. The use of cIMT continues to hold diagnostic promise and needs added evidence with children to advocate its use as a proper diagnostic assessment technique.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793241275584 – Supplemental material for Exploring the Potential to Identify Early Development Pre-Atherosclerotic Disease in Pediatric Carotid Arteries
Supplemental material, sj-docx-1-jdm-10.1177_87564793241275584 for Exploring the Potential to Identify Early Development Pre-Atherosclerotic Disease in Pediatric Carotid Arteries by Kevin D. Evans, Julie A. Stephens, Peter Bradbury, Isaiah W. Bloom, Nicole Stigall-Weikle, Amrik Singh Khalsa and Colleen Spees in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793241275584 – Supplemental material for Exploring the Potential to Identify Early Development Pre-Atherosclerotic Disease in Pediatric Carotid Arteries
Supplemental material, sj-docx-2-jdm-10.1177_87564793241275584 for Exploring the Potential to Identify Early Development Pre-Atherosclerotic Disease in Pediatric Carotid Arteries by Kevin D. Evans, Julie A. Stephens, Peter Bradbury, Isaiah W. Bloom, Nicole Stigall-Weikle, Amrik Singh Khalsa and Colleen Spees in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
This research team thank all their graduate students who took part in the diagnostic assessment of children reporting for this study.
Ethics Approval
Ethical approval for this study was obtained from The Ohio State University’s Internal Review Board (Biomedical IRB #2017B0110).
Informed Consent
Written informed consent was obtained from legally authorized representatives before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of a larger study that was funded by The United States Department of Agriculture #2017-68001-26353. This publication was supported, in part, by the National Center for Advancing Translational Sciences of the National Institutes of Health under grant no. UM1TR004548. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Peer Reviewer Guarantee Statement
The Editor / Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor / Associate Editor had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.