
Abstract
Eccrine spiradenoma is a well-recognized benign tumor arising from the intradermal straight portion of the eccrine or merocrine sweat glands. It is usually a small, solitary lesion in the cutis and the subcutaneous tissues. As with other lesions in the cutis and the subcutaneous tissue, few cases describing the sonographic findings of eccrine spiradenoma have been reported. This case study demonstrates these sonography findings in a case of eccrine spiradenoma distributed in the right thigh.
Eccrine spiradenoma is a benign tumor of the sweat gland that was first described by Kersting and Helwing in 1956.1–3 Eccrine spiradenoma is characteristically located in the superficial and deep dermis and occasionally is located in the subcutaneous tissue. The tumor, which is usually covered by normal or blue epidermis, typically occurs in patients aged 20 to 40 years.2,4 It has a predilection for developing in the upper thorax but has also been described as a tumor occurring elsewhere in the body. 4 We report the ultrasonographic (US) findings in a case of eccrine spiradenoma in the right thigh.
Case Report
A female patient in her late 30s was admitted to our clinic for sonographic examination of a nodule on her right thigh that had been present for the past five years. During this time, the nodule had slowly increased in size. The patient reported no other similar lesions anywhere on her body, and her family history revealed no similar lesions. There was no history of pain, bleeding, or trauma. On physical examination, there was a small elevated subcutaneous lesion noted on the posterior part of the right thigh. Sonographic imaging was done using a linear array transducer with a 5- to 12-MHz multifrequency capability (Siemens Sonoline Antares; Siemens Healthcare, Erlangen, Germany). Sonographic examination showed a complex nodule with solid and cystic components (Figure 1A) located in the subcutaneous area with moderate vascularity (Figure 1B). It measured 3 × 2 cm and was well circumscribed and insensitive to pressure. The patient had a complete excision of the nodule, and pathologic examination showed benign eccrine spiradenoma. Microscopically, the nodule, which was located in the dermis and extended into the subcutaneous fat, was surrounded by a fibrous capsule. No mitotic activity was observed within the tumor. Multiple areas of tumor necrosis, cystic degeneration, and old hemorrhage were present (Figure 2). Neither vascular invasion nor perineural invasion was identified. The patient was discharged from the hospital and at three months follow-up showed no evidence of recurrence or complaint.
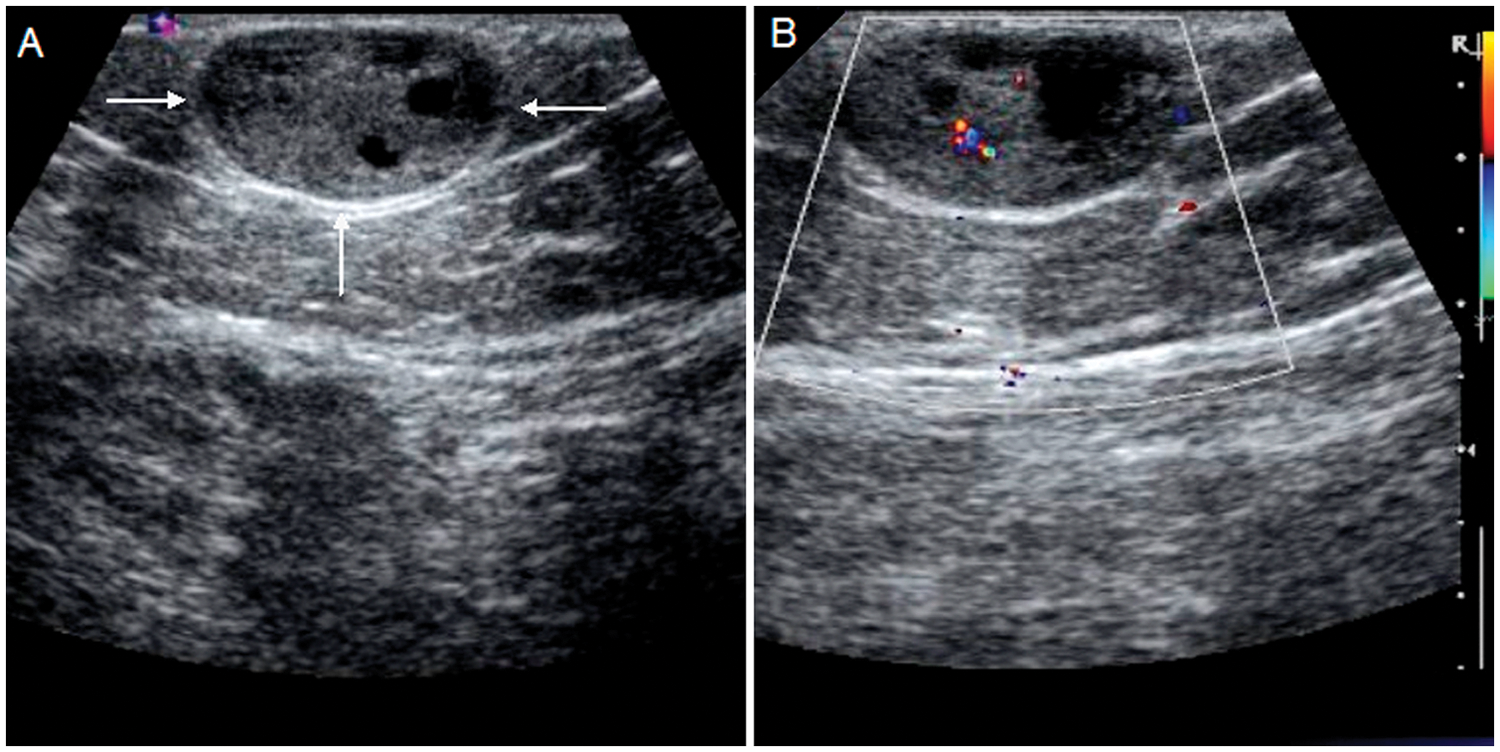
(A) B-mode ultrasound shows a well-defined mass with complex solid and cystic components (white arrows). (B) Color Doppler imaging shows a tumor with moderate vascularity.
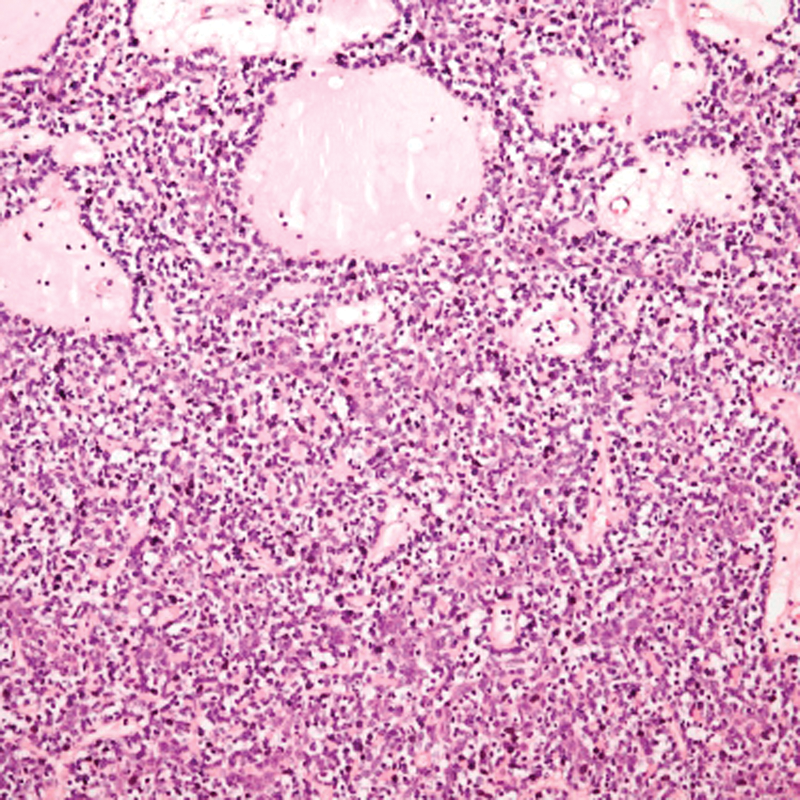
Solid neoplasm with two types of cells, edematous stroma, and lymphocytes (hematoxylin and eosin stain ×200).
Discussion
Superficial soft-tissue tumors can be classified into two categories: epidermal-dermal (or cutaneous) tumors and subcutaneous fat layer (or subcutaneous) tumors. Cutaneous tumors include tumors originating from skin appendages such as sweat glands, sebaceous glands, and hair follicles. 1 Eccrine spiradenoma is a benign tumor of the sweat gland that was first described by Kersting and Helwing in 1956. 3 Eccrine spiradenoma is characteristically located in the superficial and deep dermis and occasionally is located in the subcutaneous tissue. The tumor usually presents as a solitary firm, round dermal nodule on any part of the body but most frequently on the face, scalp, trunk, and proximal parts of limbs.1-7 These lesions are typically small, discrete, well defined, and embedded in normal eccrine sweat glands. There is no age, sex, or site predilection. 4 Clinically, the lesion is often a solitary nodule that can be as large as 5 cm.
Considering the anatomic location and clinical history, differential diagnoses should include anaplastic carcinoma, adenocarcinoma, squamous cell carcinoma, and adnexal neoplasms other than spiradenoma, such as cylindromas or basal cell carcinoma. 5 The most common mesenchymal superficial malignancy is dermatofibrosarcoma protuberans, which arises from the dermis and therefore is considered a cutaneous lesion. Peripheral nerve sheath tumor, angiomatous lesion, lipoma, malignant fibrous histiocytoma, liposarcoma, leiomyosarcoma, epithelioid sarcoma, and leiomyosarcoma are other common types of mesenchymal tumors. Nodular fasciitis and fibromatosis are two additional entities that may arise in the fascial layer. 2
Malignant eccrine spiradenomas are aggressive and metastasize to the lymph nodes, bones, lungs, and brain. 6 Clinical signs of malignant transformation include the new onset of pain, increasing tenderness, color change, and rapid enlargement or ulceration of a lesion that has been stable for years.
Sonography can play an important role in the diagnosis of benign, vascularized superficial soft-tissue tumors. Awareness of US findings is important in establishing the correct diagnosis and determining the optimal treatment. 7 Sonography provides high-resolution images in real time and is generally more readily available and less expensive than computed tomography or magnetic resonance imaging and can even be found frequently in small clinics. Furthermore, sonography is a useful noninvasive method for evaluating the cutis and subcutaneous diseases by acquiring information about the nature, size, and depth of the lesions, as well as their relationship to adjacent vessels and other structures. 8
Conclusion
This case reports the finding of a benign eccrine spiradenoma in an unusual anatomic location, the posterior thigh. The sonographic findings are reported and the sonographic characteristics of these lesions discussed. The use of sonography can be helpful in the detection and follow-up of eccrine spiradenoma as well as evaluation for other possible diagnoses of similar lesions noted on physical examination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.