
Abstract
Objective:
The aim of this product evaluation was to investigate the workflow and occupational health benefits of implementing augmented reality (AR) technology (MediView XR Inc, Cleveland, OH) paired with a portable ultrasound equipment system.
Materials and Methods:
A diverse sample of sonography users was consented and ranged in experience levels. They were asked to complete a video training session, a hands-on demonstration, and remote instruction while using the augmented reality ultrasound (AR US) system. The duration of participants’ tasks was assessed during the use of both AR US and the 2-dimensional ultrasound (2D US) system. Participants’ postures and positions were evaluated using the Rapid Upper Limb Assessment (RULA), which assessed ergonomic risk factors, linked to body position and muscle usage. Participants also completed the System Usability Scale (SUS). Finally, participants were invited to complete a qualitative interview session, regarding the use of the AR US system.
Results:
A total of 20 participants provided data after using both the AR US and 2D US systems. The assessment data revealed positive SUS scores, which reflected favorably on both the product, education, and the training provided. The time spent on simulated work (20 minutes), with both imaging systems, remained consistent. The Rapid Upper Limb Assessment tool (RULA) scores for the cohort indicated a lower (better) median upper body score when using the AR US system. The cohort also had a statistically significant lower median subscore for the neck, trunk, and legs, compared with 2D US (p < 0.00).
Conclusion:
Although larger studies are necessary to validate these findings, this cohort identified several opportunities for integrating the AR US system. Preliminary evidence suggests that an AR US system may offer occupational health benefits, as part of the imaging workflow.
Innovations to ultrasound equipment systems have continued at a steady pace and in many ways have improved imaging quality but also required sonographers and vascular technologists to adapt to changes in workflow. Although a relatively “young” diagnostic imaging technique, sonography has been through a parade of innovative upgrades, to the ultrasound equipment system, over the last 76 years. 1 An overview of these hardware and workflow changes has not only been historic but can be divided into themes or generations.2 –4 As a profession, sonography has moved through 3 generations of significant upgrades to the basic ultrasound equipment system and this parallels the evolution of personal computers. 4 Following the progression of the personal computer, historically, the hardware has gotten smaller and the software more robust. Likewise, the ultrasound equipment system has also changed in size and configuration; however, the changes in workflow were not considered simultaneously. The ergonomic adaptions required of sonographers and vascular technologists were secondarily addressed and historically this resulted in manufacturers focusing on reducing fatigue and creating operations that were more intuitive. 2 The introduction of augmented reality (AR) coupled to an ultrasound equipment system marks a potential new generation of imaging but this time being designed with an ergonomic focus.
Augmented reality refers to the overlaying of digital content onto the real world, often through a smartphone, tablet, or other display.5,6 This emerging tool is closely related to virtual reality (VR). VR refers to the complete immersion of the user into a digital environment where the real world is no longer visible.7,8 While both technologies may have the ability to place a digital display directly in front of a user, via a head-mounted display (HMD) system, the display of AR systems allow the user to visualize the real world and digital content at the same time. The innovation of coupling AR with a third-generation ultrasound system allows the sonographer to choose where digital content is overlaid, within the real world. This allows for optimal placement of digital screens by the sonographer while performing procedures or completing diagnostic exams. It has been stated that there are suspected technological, personal, social, and cultural challenges to health care workers wearing technology. 9 In addition to addressing these facets, the risk of work-related musculoskeletal injuries, among sonographers, needs be considered a concomitant factor. It has been documented that 80% to 90% of sonographers and vascular technologists report working in pain.10 –12 To move into this potential next generation of imaging with an AR-based ultrasound (US) system, ergonomics needed to be considered in parallel, as part of the implementation. To this end, product testing was designed to address both functionality as well as adaption to workflow. Therefore, a product evaluation was designed for sonography users and the clinical utility of an AR US system and compared with a traditional 2-dimensional ultrasound (2D US) system, during a simulated sonogram. The product testing was driven by the hypothesis that the AR US system would lead to less neck strain and negate the need to alter between looking at the patient and monitor, as that could be accomplished simultaneously.
Materials and Methods
After obtaining Institutional Review Board (IRB) approval (IRB #2022H0180), study participants were recruited and consented to complete a simulated sonographic exam utilizing both the AR US system and the 2D US system (without AR). All simulations took place in a dedicated research lab or critical care simulation lab, in a university setting. Study participants were consented to the study, after which, participants completed the same simulated sonography exam using the AR US system (MediScout, MediView, XR Inc., Cleveland, OH) and a Vivid IQ (GE Healthcare, Waukesha, WI). The total product evaluation process took place over a 6-month time frame, to accommodate varied participant work commitments.
AR US System Description
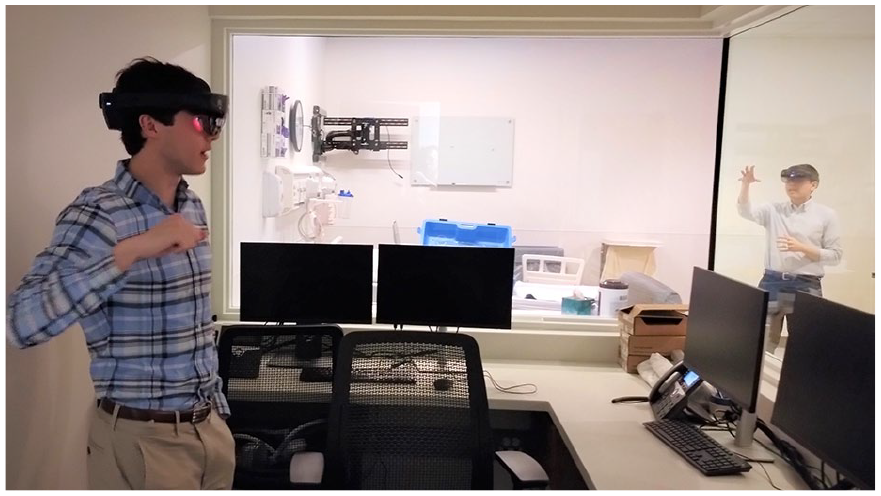
The AR US system used for the product evaluation streamed live sonographic data into a holographic HMD system allowing for the virtual placement of the sonographic viewing screen. The holographic screen could be moved, resized, rotated, or scaled to a configuration of the participant’s choosing. The AR US system was comprised of a wearable HMD (Microsoft HoloLens 2, Microsoft, Redmond, WA), data streamer PC, router, and the Vivid IQ (see Figure 1). For the simulated sonogram, a soft tissue abdominal phantom (Kyoto Kagaku, Davie, FL) was used and included abdominal and vascular anatomy.

A vascular technologist and a vascular interventional technologist (MS degrees) are shown piloting AR US system and receiving remote AR instruction through the head-mounted display (HMD) system. An undergraduate researcher is seen making observational assessments.
Study Population
A series of e-mail invitations were sent to selected participants who were recruited by personal contacts with the study’s supervising radiologist and a PhD student’s network of contacts. An individual session took an average of 2 hours to complete. A snack was provided as well as a US$20 gift card for participating. Emergency department (ED) physicians were recruited for this study as point of care ultrasonography (POCUS) users. Vascular interventional practitioners, sonographers, sonography educators, and nurse practitioners were also included in the recruitment, as they routinely perform sonography guided procedures.
Procedure Setup and Training Session
The project was accomplished by inviting study participants to gain training on the use of the AR US system and how it could be used in adjunction to a standard sonography examination. A training session was designed to allow the participant to gain an appreciation for how this technology might be used in clinical practice. Participants were given a narrated training video relative to introduce the AR US system. The video and hands on instruction took place in the research lab and then moved to the simulation center. The simulation center had an intensive care unit setup, as well as a private 2-way mirror for viewing and assessment (see Figures 2 and 3). This allowed the researchers to create a more realistic patient case scenario.
Physician shown going through the practice session to master basic AR skills with the head-mounted display (HMD) and the AR systems. Undergraduate researcher (also wearing HMD) in the control booth of the simulation lab, providing instruction in real time.
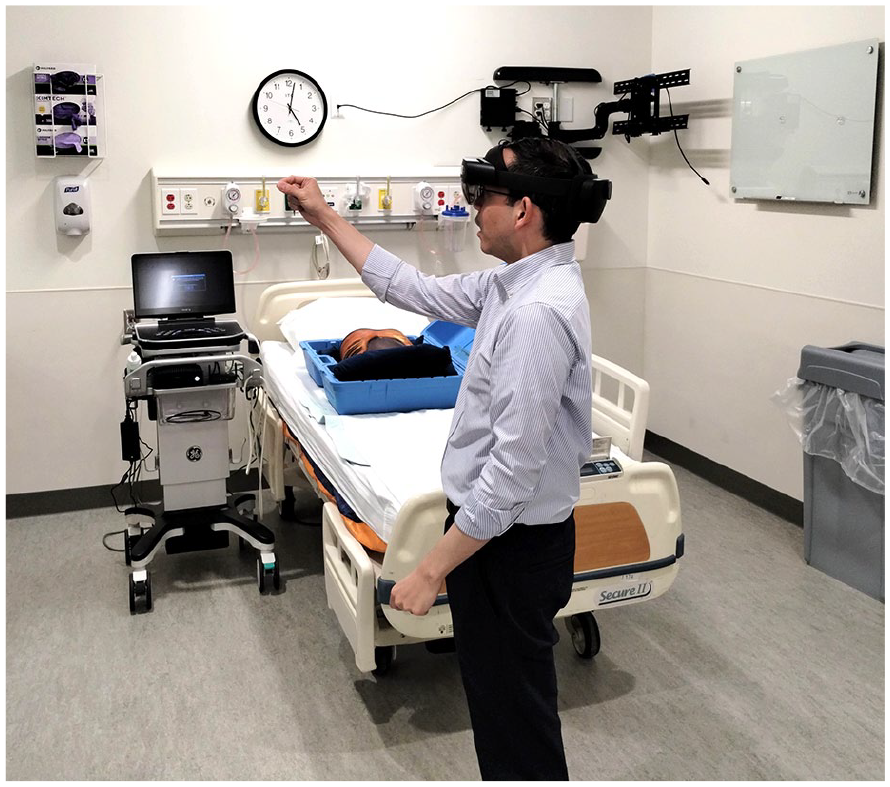
Physician, wearing HMD, is working to master his “far touch” AR skills before beginning his AR US examination of the aorta, using the Kyoto phantom.
The Design of the Training Session
This 1-hour educational session was devoted to reviewing and assisting participants to gain mastery of the AR US system. Remote assistance allowed for the researchers to view the participant’s point of view remotely and this was accomplished by establishing a video connection between the 2 HMD devices (trainer and participant). Remote assistance was enabled to allow the researcher-trainer to monitor and assess the participant’s learning progress. Participants were instructed on the use of specific techniques, while using the AR US system. The following skills were taught and assessed, during the educational session:
“Near AR touch” interactions for screen manipulation: The participant “physically” touches the holograms to manipulate and personalize them.
“Far AR touch” interactions for screen manipulation: The participant manipulates the holograms from a distance with a cursor to alter them.
“AR touch-free” interactions (voice command) for screen manipulation.
The Training Session for Participants
Participants were allowed to explore the system interactions on their own and become accustomed to the AR US system. Participants were provided time to use the GE Vivid IQ, if they were unfamiliar with that system. Researchers also assessed participant’s ability to utilize the various AR interactions. Accurate implementation of these skills was a requirement to move on to the evaluation session.
Evaluation Session Protocol
Participants were asked to focus on how this technology would translate to their daily job tasks. While wearing the HMD, as part of the AR US system, participants were contextually placed in a procedural setup to attempt to simulate their workflow. Participants were asked to translate the skills learned in the previous training session to this experiential part of the study. Time was provided to allow the participants to gain practice, imaging the aorta on the phantom. The evaluation session involved completing a gray-scale sonographic evaluation of the aorta. All participants completed the aorta sonogram with both the AR US and the 2D US systems (this sequence was randomized). Participants were asked to do the following tasks:
Image the phantom and save sonographic images of the aorta (sagittal and transverse).
Complete the individualized aorta sonogram twice, with the AR US and 2D US systems.
Take the time needed to achieve diagnostic quality images, while being assessed on their physical ergonomics. The assessments were done using the Rapid Upper Limb Assessment tool (RULA) (see Attachment 1.0 QR Code). 13
Provide participant feedback on the overall session and the data collection.
The scoring of the RULA tool was rechecked, upon completion, by a second researcher. Immediately after finishing the 2 aorta sonograms, participants were asked to complete the System Usability Scale (SUS), which has 10 Likert scale questions (see Attachment 2.0 QR Code). 14 Finally, interview questions were composed such that the participant’s impression of the usability, usefulness, and desirability (UUD) of the AR US system were recorded (see Attachment 3.0 QR Code).
The quantitative data were based on survey responses, executing a time study, and the scoring of the participant’s posture and position while using the equipment. The qualitative data came from observations of participants, recorded feedback during the session, and the UUD qualitative interview session.
Statistical Analysis
A statistician/methodologist was used to refine the research design and the anticipated statistics. All the data endpoints were pulled together to form a mixed-method analysis of the equipment and recommendations for next steps. Primarily, this was conceived as a descriptive study with means, medians, and frequencies, as the primary endpoints. Statistical comparisons of the study variables were anticipated therefore tests for normality, as well as correlations were planned. The p-level was chosen as .05, a priori.
Results
The results were based on a cohort of participants that reflected a cohort of sonography users (4 physicians, 8 MS-graduate providers, and 8 BS-graduate sonographers). All the participants were actively using sonography and had no prior experience with AR and limited VR skills. As planned, the data was evaluated for descriptive statistics first and assessed for normality. The distribution of the data and the small number of participants (N = 20) resulted in a nonnormal distribution of data; therefore, medians and standard deviations were reported (see Figure 4).
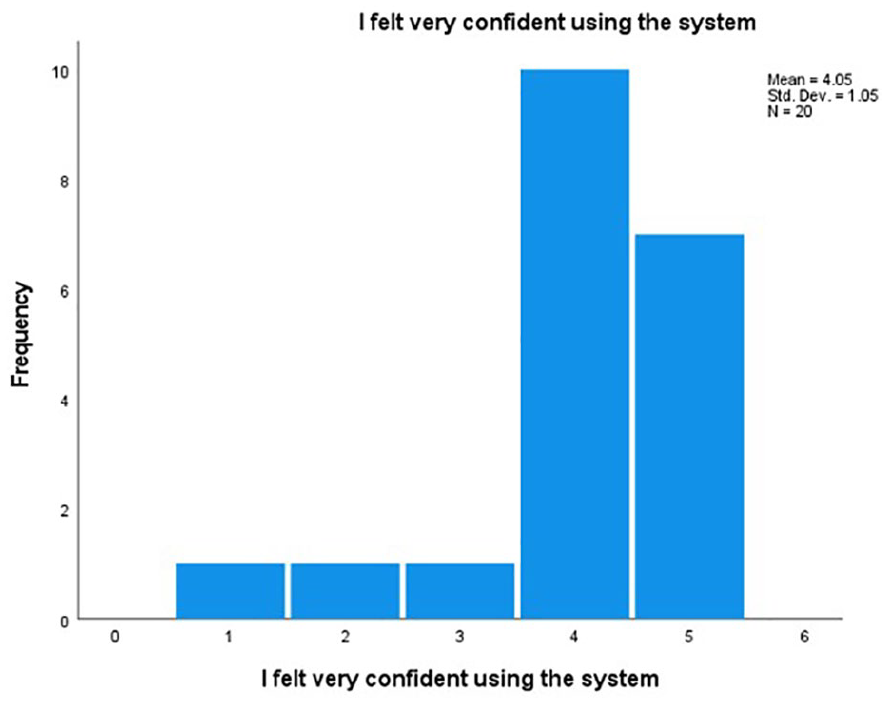
Box plot that demonstrates the nonnormal distribution of the SUS response item data.
The first set of survey questions, posed to participants, were based on the evaluation of the AR US system, and it was evaluated for usability using the SUS. Each question was scored on a 5-point Likert scale with “5” representing strongly agreeing with the prompt, and “1” representing strongly disagreeing with the prompt. The survey questions and the median response of the cohort are provided in Table 1.
Participants Overall Results, Based on the SUS Survey Provided to Participants.
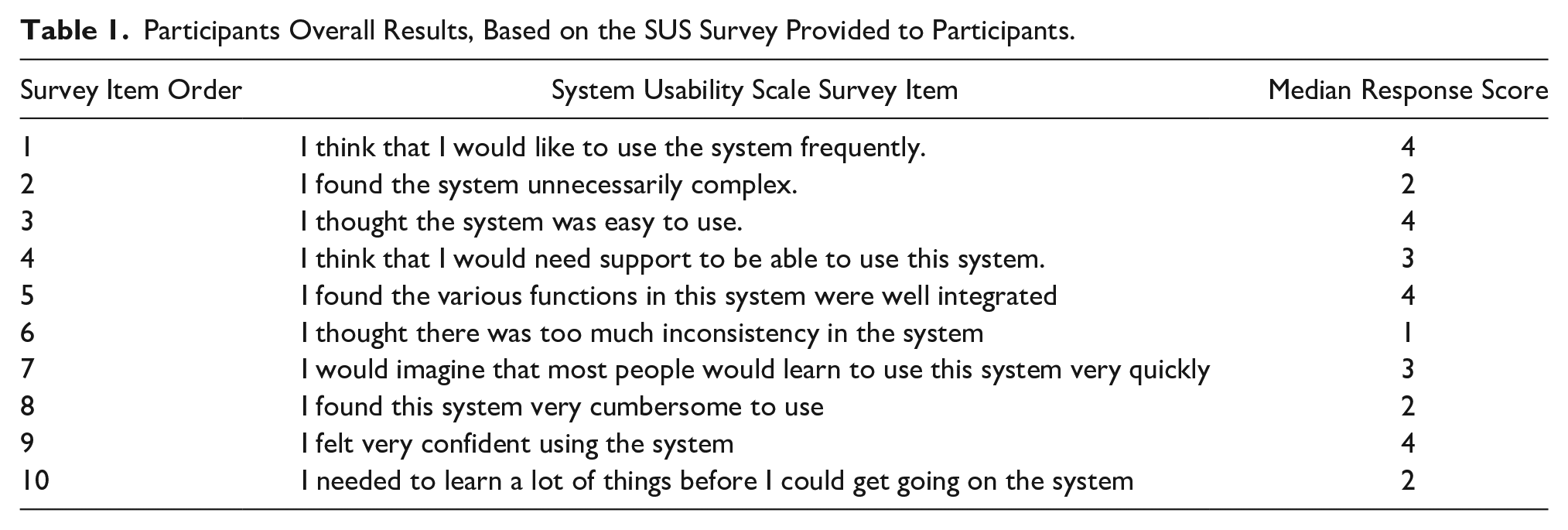
System Usability Scale can be individually scored and benchmarked; 15 however in this study, participant scores may have been conflated with attitudes about the education and training provided prior to using the AR US system. Given this threat to validity, the size of the cohort and the contextual ratings made benchmarking seem inappropriate.
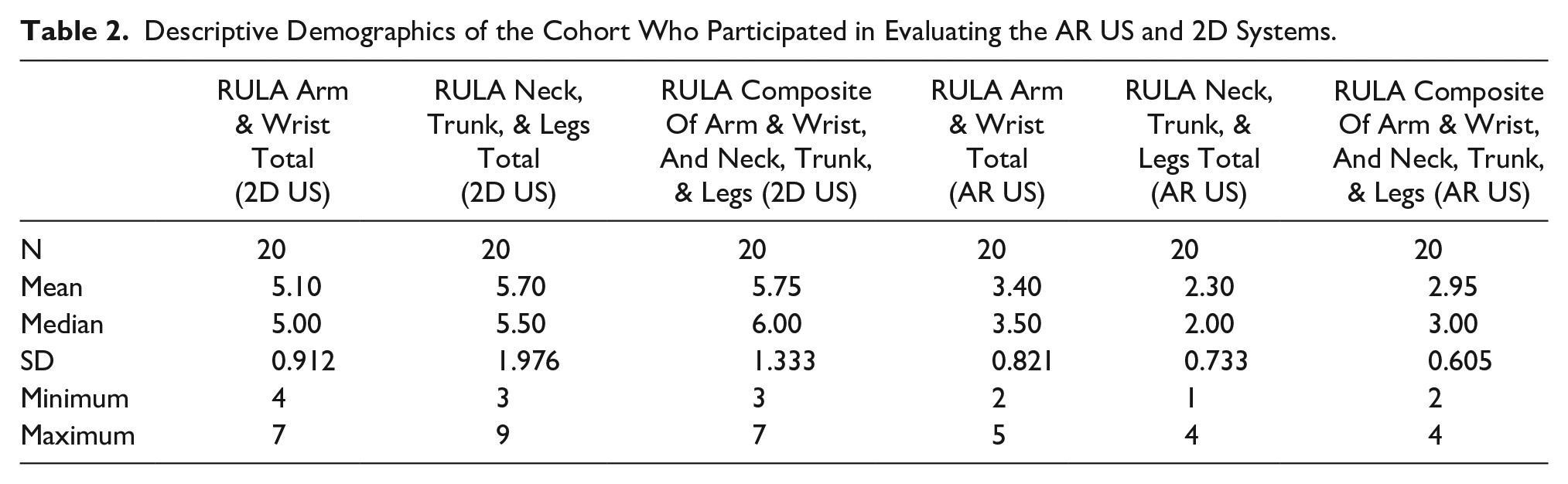
Participants were also assessed while using the AR US and 2D US systems. They were graded on their physical movements and postures, using the RULA tool. Lower RULA scores indicate less stress/strain on the neck, trunk, and legs, while performing specific actions. It was observed that using the HMD, provided an improved or neutral effect on posture, depending on participant’s position. RULA scoring also demonstrated nonnormal distribution of the data. Table 2 demonstrates the cohort’s RULA scoring mean, medians, and standard deviations.
Descriptive Demographics of the Cohort Who Participated in Evaluating the AR US and 2D Systems.
As indicated, the nonnormal distribution of the data required the use of nonparametric statistics, so the Wilcoxon signed ranks test was used to determine the significance of improvement for these participants’ RULA subscores. Table 3 provides the results, and the overall statistical significance was at the P = .000 level. Overall, this cohort demonstrated an improved set of RULA scores for their neck, trunk, and legs, while using the AR US system.
The Statistical Analysis of the RULA Score Improvement for Upper Extremity (Neck, Upper Extremity, Trunk, and Legs, Based on the Wilcoxon Signed Ranks Test (a)).
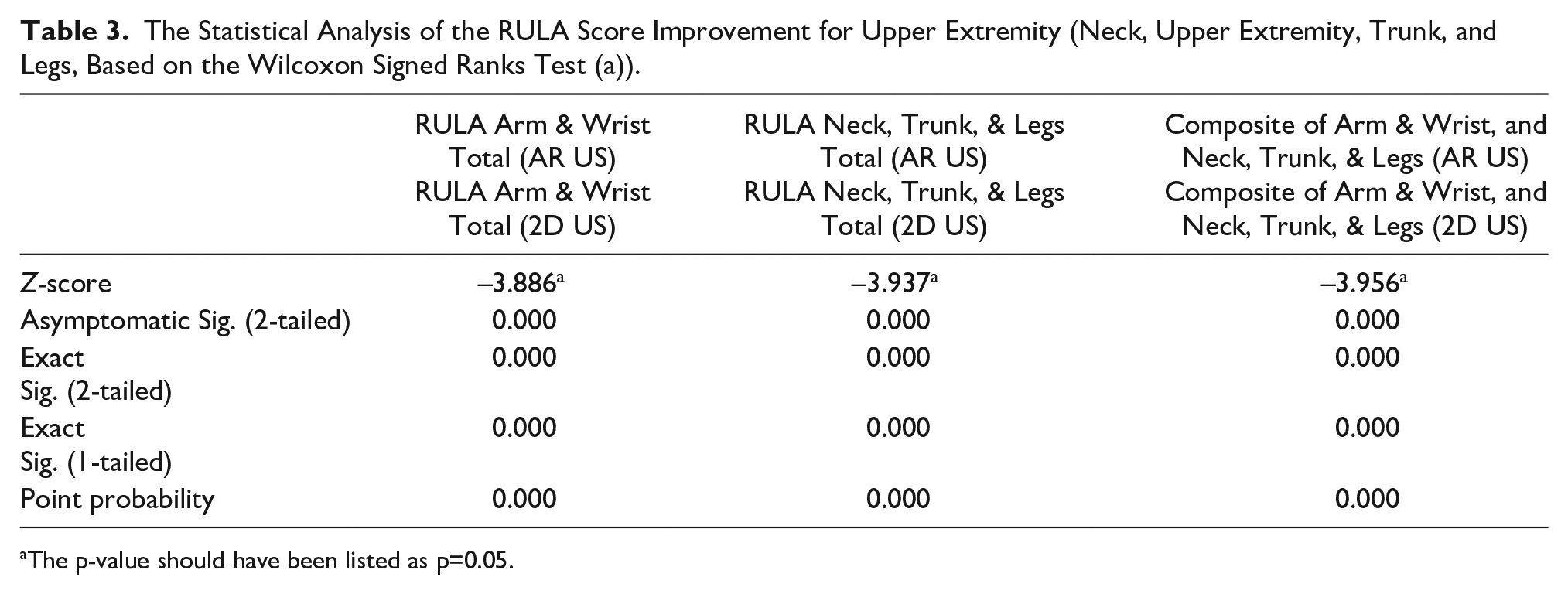
The p-value should have been listed as p=0.05.
An additional concern was whether these ergonomic gains were tied to the participant’s confidence using the AR US system. Although a great deal of effort was invested in training to use the system, the concern was the influence of it on the improvement of the participant’s upper body assessments. A correlation was completed to gauge that association (see Table 4).
The Strength of Association and Statistical Significance of AR US System Confidence Compared with RULA Composite Scores for the Upper Body.
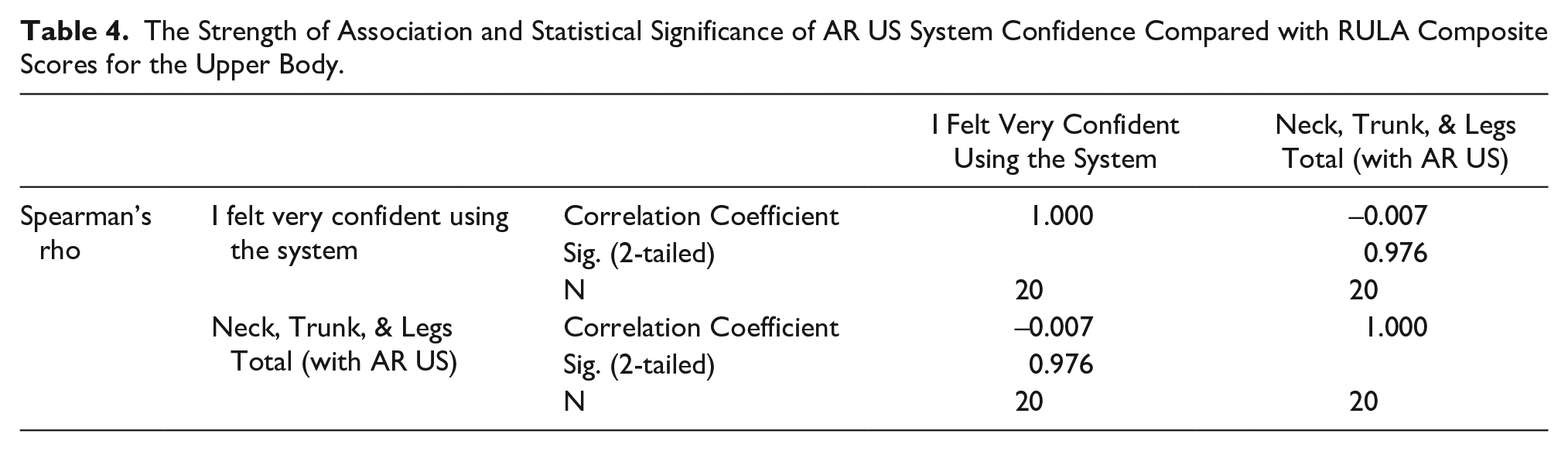
This demonstrated that for this cohort, confidence in using the AR US system was not statistically significantly related to the neck, trunk, and legs RULA scores, recorded while using simulation (e.g., r = –.007, P = .976).
Next, the timing study of the 2 examinations (AR US and 2D US) were compared. The examination time results, for this cohort, was an aorta examination completed on an average of 20 minutes. These participants demonstrated no difference in exam time when using the AR US system, compared with the 2D US system.
Based on the qualitative interviews conducted with this cohort, the participants repeatedly expressed the usefulness of having more access to the post-processing ultrasound equipment system controls, via the AR US system (i.e., overall gain, TGC, power, etc.). The participants also expressed the usability of being able to magnify the sonography image without turning to the keyboard. Results from these UUD based interviews provided further insight into initial reactions demonstrated beyond the SUS median scores. Alongside confirming previously held positive reactions to the AR US system, it also provided further insight into possible future modifications that could be made to the hardware or software. As previously expressed, increased control of the sonography image, inside of the equipment software, was the most desired system feature.
Discussion
As was highlighted in the introduction, generations of ultrasound equipment systems have been successfully launched, but ergonomic considerations had to be addressed after being introduced into the sonographer and vascular technologist’s workflow. These backward designs to address work-related musculoskeletal injuries, writ large, have not been viewed positively by the workforce. In a recent study of sonographers reporting pain, participants reporting work-related discomfort based on the percentage of using ultrasound equipment systems was highly significant for those sonographers conducting abdominal and OB/Gyn examinations. 12 Likewise, these same sonographers and vascular technologists reported visual discomfort based on the percentage of using ultrasound equipment systems. 12 This underscores the importance of designing and testing next-generation ultrasound equipment systems, coupled with AR, in parallel and making sure that these practices are not contributing to work-related musculoskeletal pain and discomfort.
This AR US system product evaluation was provided to a cohort of varied sonography users, as part of the market introduction and these participants provided very positive feedback, based on their SUS scoring. These SUS scores were considered an affirmation of both this next generation of imaging, as well as the education and training that was provided. These scores being tied to the investment in the education and training of the AR US is a translational component and needs to be considered for maximum benefit to workflow. Sonographers have also rated disruptions to overall workflow as being a significant factor in contributing to work-related pain by abdominal sonographers and vascular technologists. 12
Time savings is another important facet in persevering workflow and introducing these types of innovations. According to Nguyen et al, 16 studies conducted with similar AR US systems demonstrated a 17% improvement in novice sonography exam times, although experienced participants were about 5% slower. In addition, continued use of this next generation of equipment might allow sonographers to have an easier transition, given that the timing is not a workflow disruption. According to Eckert et al, 8 AR application in medicine has a growing body of empirical research and many of these publications are devoted to exploring its maturing functionalities, as time moves forward. Furthermore, Farshad-Amacker et al, 17 demonstrated that in sonographic clinical procedures, coupling AR to an ultrasound equipment system reduced total examination time, adding further incentives to adopting these type of imaging systems. This was also explored in a study by Cattari et al 18 in which ultrasound-guided interventions using AR headsets demonstrated that 80% of participants were able to perform procedures with AR headsets at a similar level of accuracy as with conventional methods (see Figure 5). This next generation of imaging system is likely going to be pervasive in many areas within health care, and it will depend on its ease of use and minimal disruption to workflow.

The use of AR US system actively being used to conduct an ultrasound-guided medical procedure. Note the floating sonographic image that is being generated, as well as AR anatomical visualization on the patient.
Given the current focus on mitigating the risk of injury to sonographers and vascular technologists, the RULA subscores demonstrated a reduction in the neck, trunk, and leg stress, which is another important facet of this technology. In this cohort, the reduction of stress on the neck, trunk, and legs is important to consider, as a recent survey found that the frequency of individuals experiencing work-related musculoskeletal discomfort was 84.9% to 87.7% and that was regardless of sonography practice. 12 The generation of AR coupled to sonogram technology needs to demonstrate no further risk to sonographers and vascular technologists and based on the current study data, must have a potential risk reduction. It is also important to focus on the sonographers’ hand when holding the transducer, as that has been shown to be significantly related to reported pain and discomfort. 12 In the current study, the RULA wrist scores, when using AR US were a median of 3.5 compared with 5.5 when using current ultrasound equipment systems. The lower median score is an improvement and serves as a possible mitigation to the report pain and injury in the wrist. As important as the training in use of the system, it is important to underscore that this cohort got ergonomic benefit independent of their confidence in using all the facets of the system.
The qualitative UUD interviews provided a lot of useful information on how to further improve the user experience and incorporate the postprocessing of images during the examination. Voice commands were likely the next innovation and upgraded needed to provide this kind of control that was important to this cohort of participants. Instrumentation and image quality were a high priority as well as the importance of ergonomic training. In the survey that has been mentioned (53.3%–55.9%) of sonographers and vascular technologists completed ergonomic training but still reported work-related pain and discomfort. 12 This points to the need to make sure that ergonomic training is contextualized and specific to the hardware and software being used.
As part of this study, the researchers did also emphasize the way to address the patient (in this case, the phantom) while using the HMD system. The importance of lifting the viewing lens and always addressing the patient and explaining the US AR system (in lay language) was stressed with all participants. In no way should this innovative technology diminish patient rapport.
Limitations
The most significant limitation was the descriptive research design and the limited convenient sample of users. Moving forward, a greater diversity of participants should be recruited to test this type of AR US system, getting more physicians, residents, and other sonography professionals beyond the specialties already tested (radiology, emergency medicine, sonography) would provide greater diversity in perspective on the product’s usage. This study should be replicated with other sonographic examinations to determine the same benefits. The amount of time provided for instruction and practice using the AR US system was lengthy and as such likely makes these results connected to amount of teaching provided. One further limitation that was encountered was the need for proper lighting. Given the nature of holographic projections, it is difficult to conduct these tests in areas with a large amount of natural light, or in areas where indoor lighting must remain on. Further testing on the effects of lighting constraints on performance may be warranted. These constraints which are necessary to provide the most accurate representation of the AR US system could be explored further in future comparative analyses.
Conclusion
The advent of the clinical use of AR technology has introduced several new areas of study and potential worker skills needed in the workplace. This product evaluation provided promising early results and lends credence to the ergonomic value of this set of work tools. Continual developments in the technology will further progress in making the system more intuitive and all-encompassing. It is important to note that a code of conduct/etiquette for professionals utilizing the system will need to be further explored when interacting with patients. Development of a patient care centered protocol for implementing AR into clinical practice, an example being that the HMD lens should be flipped up to speak with the patient before lowering it to work, alongside explaining that some discussion will occur with physicians or experts through the HMD. Preliminary evidence suggests that an AR US system may offer occupational health benefits, as part of the imaging workflow.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793241268415 – Supplemental material for A Product Evaluation of Augmented Reality Equipment Coupled to Diagnostic Medical Sonography: A Potential Equipment and Ergonomic Innovation
Supplemental material, sj-docx-1-jdm-10.1177_87564793241268415 for A Product Evaluation of Augmented Reality Equipment Coupled to Diagnostic Medical Sonography: A Potential Equipment and Ergonomic Innovation by Kevin D. Evans, Peter Bradbury, Isaiah W. Bloom and Menglin Xu in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793241268415 – Supplemental material for A Product Evaluation of Augmented Reality Equipment Coupled to Diagnostic Medical Sonography: A Potential Equipment and Ergonomic Innovation
Supplemental material, sj-docx-2-jdm-10.1177_87564793241268415 for A Product Evaluation of Augmented Reality Equipment Coupled to Diagnostic Medical Sonography: A Potential Equipment and Ergonomic Innovation by Kevin D. Evans, Peter Bradbury, Isaiah W. Bloom and Menglin Xu in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-3-jdm-10.1177_87564793241268415 – Supplemental material for A Product Evaluation of Augmented Reality Equipment Coupled to Diagnostic Medical Sonography: A Potential Equipment and Ergonomic Innovation
Supplemental material, sj-docx-3-jdm-10.1177_87564793241268415 for A Product Evaluation of Augmented Reality Equipment Coupled to Diagnostic Medical Sonography: A Potential Equipment and Ergonomic Innovation by Kevin D. Evans, Peter Bradbury, Isaiah W. Bloom and Menglin Xu in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
Our researchers thank Carolyn M. Sommerich, PhD, CPE, FHSE, and Christopher Kanner, MD, for their guidance, input, and overall support. We also greatly appreciate the support of the staff and corporate executives at MediView XR, Inc., who gave us primary training in the AR US system.
Ethics Approval
Ethical approval for this study was obtained from Institution Review Board (IRB #2022H0180).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding provided by MediView LLC. An agreement was executed that the funding came without regard to the study outcomes.
Peer Reviewer Guarantee Statement
The Editor / Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor / Associate Editor had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.