
Abstract
A central venous catheter is often used when managing patients who need hemodialysis. Venous thrombus formation is often a complication of catheter placement. Most patients with catheter-related thrombus (CRT) are asymptomatic. Gray scale and duplex sonography have a high sensitivity and specificity rate for detecting CRT. This case study presents a patient with a CRT and reviews the structures a sonographer should assess when a patient presents for evaluation of the lower extremity venous system, with an iliofemoral catheter in place.
Deep vein thrombosis (DVT) is a blood clot in one or more deep veins, in the peripheral vascular system, usually in the leg. Deep vein thrombosis is found in as many as 600,000 people each year in the United States and accounts for 100 000 to 180 000 deaths each year. 1 A thrombus involving the iliac veins and/or the common femoral vein is known as an iliofemoral DVT and represents 25% of DVT cases. 2 This case study reviews an iliofemoral catheter-related thrombus (CRT) involving the common femoral vein and iliac vein in a patient with a central venous catheter used for hemodialysis. Central venous catheters are commonly used in hospitalized patients for long-term therapy but are also used in outpatient settings for the infusion of antibiotics, chemotherapy agents, and hemodialysis. Catheter-related thrombus is considered a unique form of DVT. At least 25% of patients with CRT do not present with symptoms, so when a venous catheter is imaged, careful sonographic evaluation should be performed to identify a potential thrombus. 3
Case Report
An 18-year-old man presented to the emergency department with respiratory distress, related to an upper respiratory infection. The patient had stage 3 chronic kidney disease with a hemodialysis port, in the common femoral vein. While at the hospital, the patient received dialysis and experienced vascular flow issues with the hemodialysis port. The same day, the physician ordered a bilateral lower extremity venous sonogram to help identify the reason for the hemodialysis flow issue. The sonogram showed the lower extremity veins, which appeared normal except for an echogenic mass attached to the catheter. This entity was in the right common femoral vein, with reduced phasicity and continuous forward flow (Figures 1 and 2). This diagnostic finding prompted a limited-iliac venous examination to further evaluate the mass. A noncompressible right external iliac vein with internal echoes was seen (Figure 3). The internal mass surrounded the catheter, as it moved through the external iliac vein, and into the distal common iliac vein (Figure 4). The thrombus did not extend into the inferior vena cava. Both sonograms were considered diagnostic, but deemed to be of poor image quality, due to patient habitus. The next day, the patient had the thrombosed catheter removed and a new hemodialysis catheter placed, along with starting anticoagulant therapy.
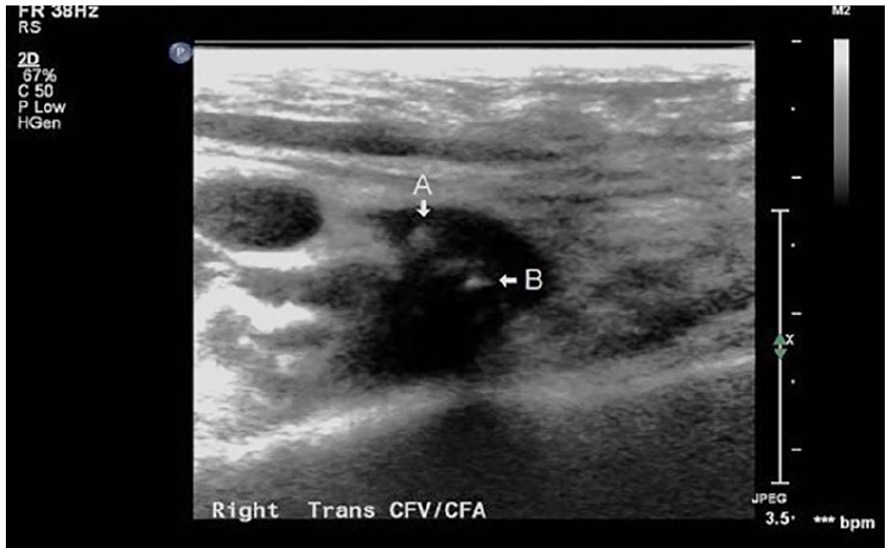
A transverse gray scale image of the common femoral vein. The arrow A is pointing to thrombus and arrow B is pointing to catheter.
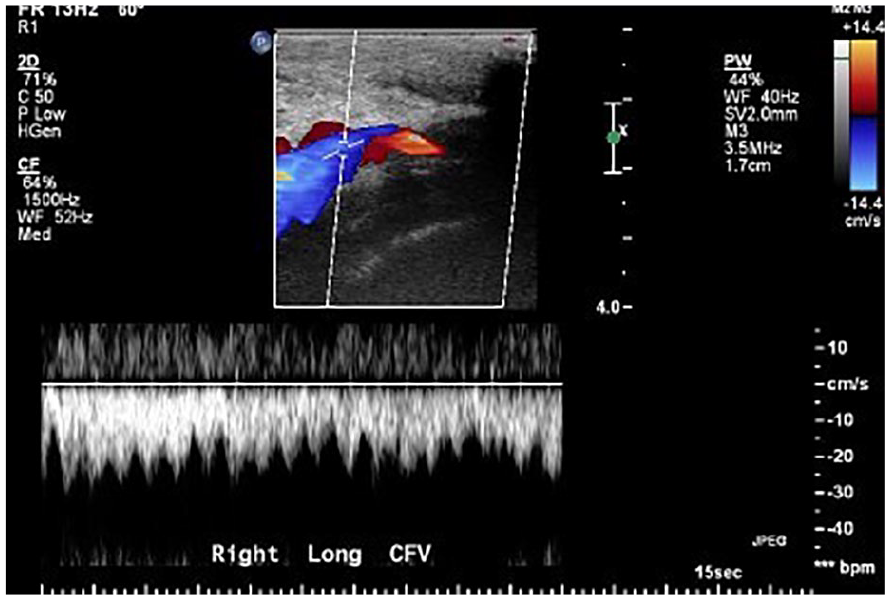
An example of a spectral waveform that demonstrated continuous flow within the vein.
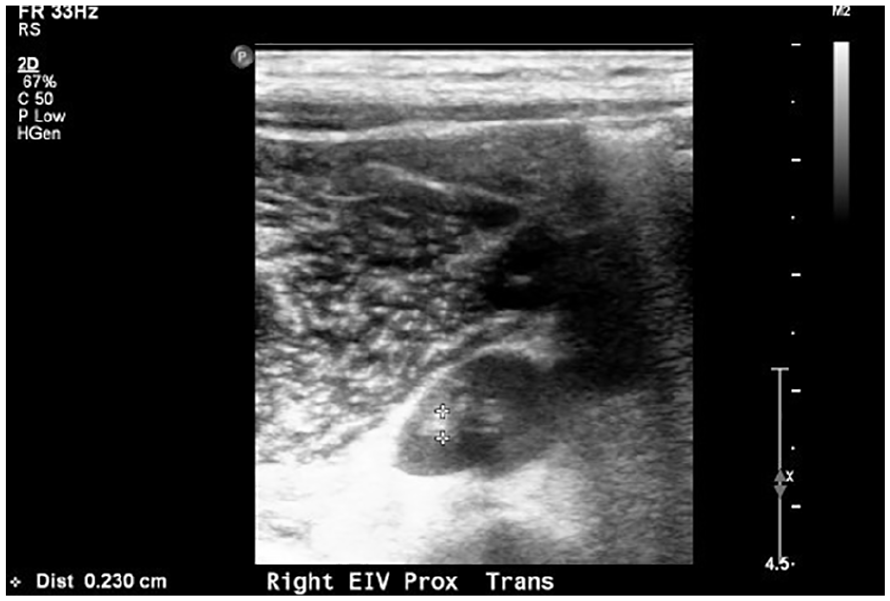
A transverse gray scale image of the external iliac vein. The calipers were placed on thrombus, which is adjacent to the catheter.
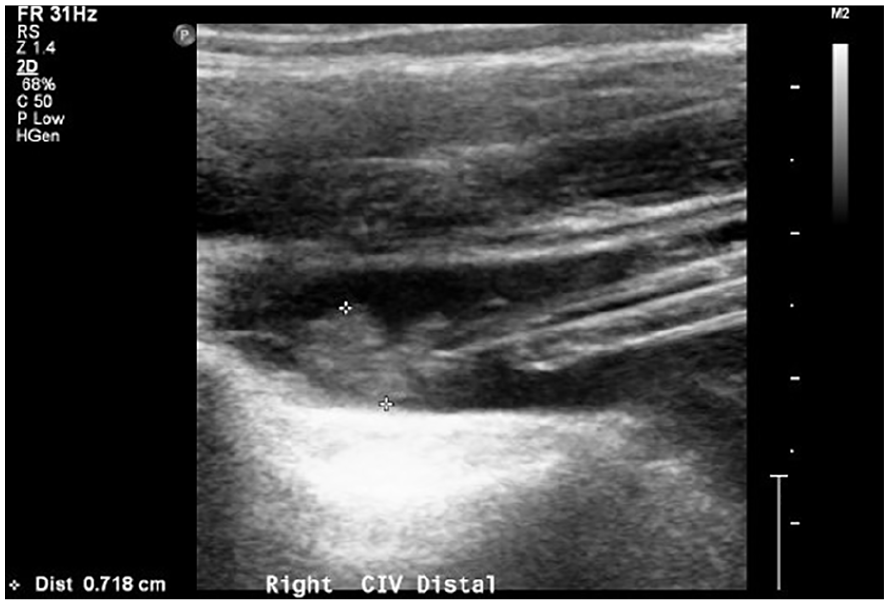
A sagittal gray scale image of common iliac vein. The calipers are placed on the venous thrombus.
Discussion
Deep vein thrombosis commonly affects the lower limbs, and the rate of involvement varies by location, with 40% in distal veins, 16% in popliteal vein, 20% in femoral vein, 20% in common femoral vein, and only 4% in iliac veins. 4 Iliofemoral DVT often affects patients with a predisposition to venous stasis. 5 Thrombosis occurs in 14% to 18% of patients after a catheter insertion and is more common with catheters inserted into the femoral vein, than the subclavian vein.6,7 Virchow’s triad of thrombogenesis summarizes the reasons for venous thrombus formation including venous stasis, endothelial damage, and blood hypercoagulable.
Catheter-related thrombus can be classified as a fibrin sheath, an occlusion of the catheter lumen, and a mural thrombus. 8 The insertion of a catheter causes damage to the vein wall triggering an inflammatory process. Coupling that process with the continual contact of the catheter against the vein wall creates persistent endothelial damage. Within hours, fibrin begins to form on the outside of the catheter and reduces blood flow by 60%, around the catheter site. 9 Erosion of the endothelium over time leads to a mural thrombosis. This pathophysiologic process causes intrinsic and/or extrinsic catheter dysfunction. An intrinsic thrombus is within the catheter and typically causes minimal patient morbidity. 10 Intrinsic thrombi can attach to the catheter tip and occlude or act like a one-way valve preventing back flow. Sheath thrombi can form when blood becomes trapped between the catheter and the fibrin sheath. In this scenario, dialysis fluids can flow into the catheter, but blood cannot be drawn from it. Mural thrombi are considered external and attach to the vessel intima where the wall touches the catheter. Risk factors involved in CRT include previous catheter infections, misplacement of the catheter tip, and having risk factors for thrombus formation. 11
Most patients with CRT are asymptomatic with as few as 5% presenting with symptoms. 12 When symptoms do appear, the patient may experience pain, edema, redness, vein distension, palpable cord, or catheter dysfuction. 13 The complications of CRT, regardless of location, include 10% pulmonary embolism, 10% loss of venous access, postthrombotic syndrome (PTS), infection, mechanical dysfunction (kinking, bending), and delay in treatment. 6 Specifically, iliofemoral DVT is associated with an increased risk of pulmonary embolism and PTS compared to DVT that originate in the lower leg. 14 Male et al 15 found that DVT formation in children is more common when the catheter is placed in the femoral vein than at other sites. Catheter-related thrombus occurs in up to 50% of children and 66% of adults who have a long-term catheter placement. 11 When catheters were used for dialysis, Sehgal et al 16 found a significant correlation between CRT and inadequate dialysis dose delivery.
There is some lack of consensus related to immediate versus delayed treatment of CRT. A delay in thrombus treatment can lead to inadequate dialysis. 13 Internal thrombi can be eliminated by removal of the catheter with only local vein damage. But if the catheter is too difficult or precarious to replace, then a thrombolytic can be a treatment option, to reopen the line. 11 External thrombi have a risk of propagation and embolization similar to other forms of thrombosis, resulting in a similar morbidity, so traditional treatments are often used. 10 With iliofemoral DVT, anticoagulation medications of heparin and warfarin are primarily used. 2 Other treatment options include the use of an inferior vena cava (IVC) filter, open surgical removal, direct thrombolysis, or endovenous removal. If using a removal technique, stenting of the iliac vessel may be helpful, particularly if the walls have significant damage.2,17
When a catheter dysfunction is suspected, a radiograph can visualize the catheter to assess for mechanical dysfunction or catheter malposition. As in this patient case, a dysfunctional catheter should prompt the evaluation for a CRT. A D-dimer test has lower sensitivity in patients with renal-impairment, so it is not considered diagnostic for assessing CRT. 18 Duplex sonography is the primary choice to help diagnose CRT. Sonography has an overall sensitivity of 90% to 94% and specificity of 93% to 98% for diagnosing proximal DVT.19 –21 Köksoy et al 22 assessed an overall sensitivity of 94% and specificity of 96% for diagnosis CRT.
Sonographically, a healthy vein has thin walls, an anechoic lumen and completely fills with color Doppler. Spectral Doppler demonstrates spontaneous continual flow that decreases with inspiration and increases with exhalation. Veins should collapse completely when compressed with the ultrasound transducer. The presence of echogenic material in the lumen and the failure of the vein to completely collapse should both occur, to fully demonstrate the presence of a thrombus. Of note, in patients with a venous catheter, the catheter will normally appear echogenic within the vessel lumen, and therefore, the line should be assessed closely for sonographic evidence of thrombus material. An acute thrombus may appear sonolucent therefore may not be seen within the lumen, but the vein should still be assessed for noncompressibility, and Doppler should be used to assess flow patterns. Color and spectral Doppler may be the only usable options to evaluate for a thrombus in patients with larger body habitus, edema, or inguinal thrombosis with or without a catheter. A proximal obstruction will show continuous flow without respiratory changes (See Figure 2). Köksoy et al 22 found the absence of respiratory phasicity had the highest sensitivity (94%) and specificity (100%), when assessing for CRT. If the sonogram is equivocal, then a contrast venogram can be ordered for a better diagnosis. Venography is also used for endovenous removal, direct thrombolysis, and stenting.
Conclusion
Catheter-related thrombus is a unique form of DVT that has certain diagnostic challenges. This case report reviews the sonographic presentation of a CRT, within the femoral and iliac veins, in a patient with a femoral hemodialysis catheter. Because patients with CRT are more likely to present as asymptomatic, anytime a catheter is present, the sonographer should interrogate it closely to identify the presence of thrombus. Much of the research devoted to catheter access is in relationship to the upper extremity. Additional research regarding the lower extremity complication rates could help in patient management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because only anonymous information was used in this report.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Peer Reviewer Guarantee Statement
The Editor / Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor / Associate Editor had no involvement in the decision-making process.