
Abstract
Catheter-related thrombosis is a relatively common complication of central venous catheter insertion. Central venous catheter use is ubiquitous in the critical care setting and often in patients with multiple risk factors for venous thromboembolism. With a trend towards increased use of peripherally inserted central catheters, the incidence of catheter-related thrombosis is likely to increase further. Despite the scale of the problem, there is a paucity of evidence-based guidelines concerning the management of patients with catheter-related thrombosis, particularly in critically unwell patients. This has led to heterogeneity in clinical practice. In this review, we describe the risk factors for developing catheter-related thrombosis and provide practical advice for clinicians on how to recognise, diagnose and treat this common problem.
Keywords
Introduction
Indwelling central venous catheters (CVCs) are ubiquitous in the critical care setting. Thrombotic complications can occur with CVC use with reported rates varying from around 5% for symptomatic events 1 to an overall rate of 14–18%. 2 Despite being relatively common, there is heterogeneity in clinic practice when it comes to the management of catheter related thrombosis (CRT). There are limited evidence-based guidelines for the best diagnostic approach and preventive measures for CRT, particularly in critically unwell patients. This review aims to provide clinicians with a pragmatic approach to dealing with CRT.
Risk factors
Risk factors for the development of CRTs.
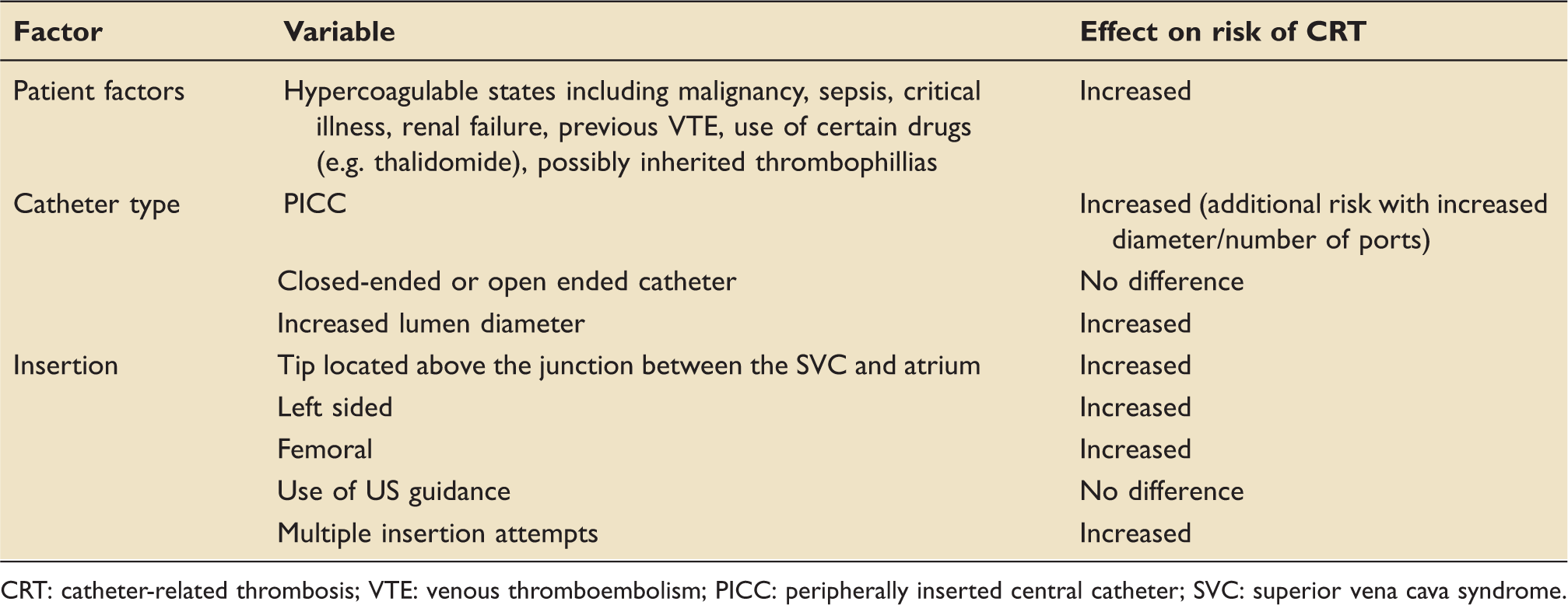
CRT: catheter-related thrombosis; VTE: venous thromboembolism; PICC: peripherally inserted central catheter; SVC: superior vena cava syndrome.
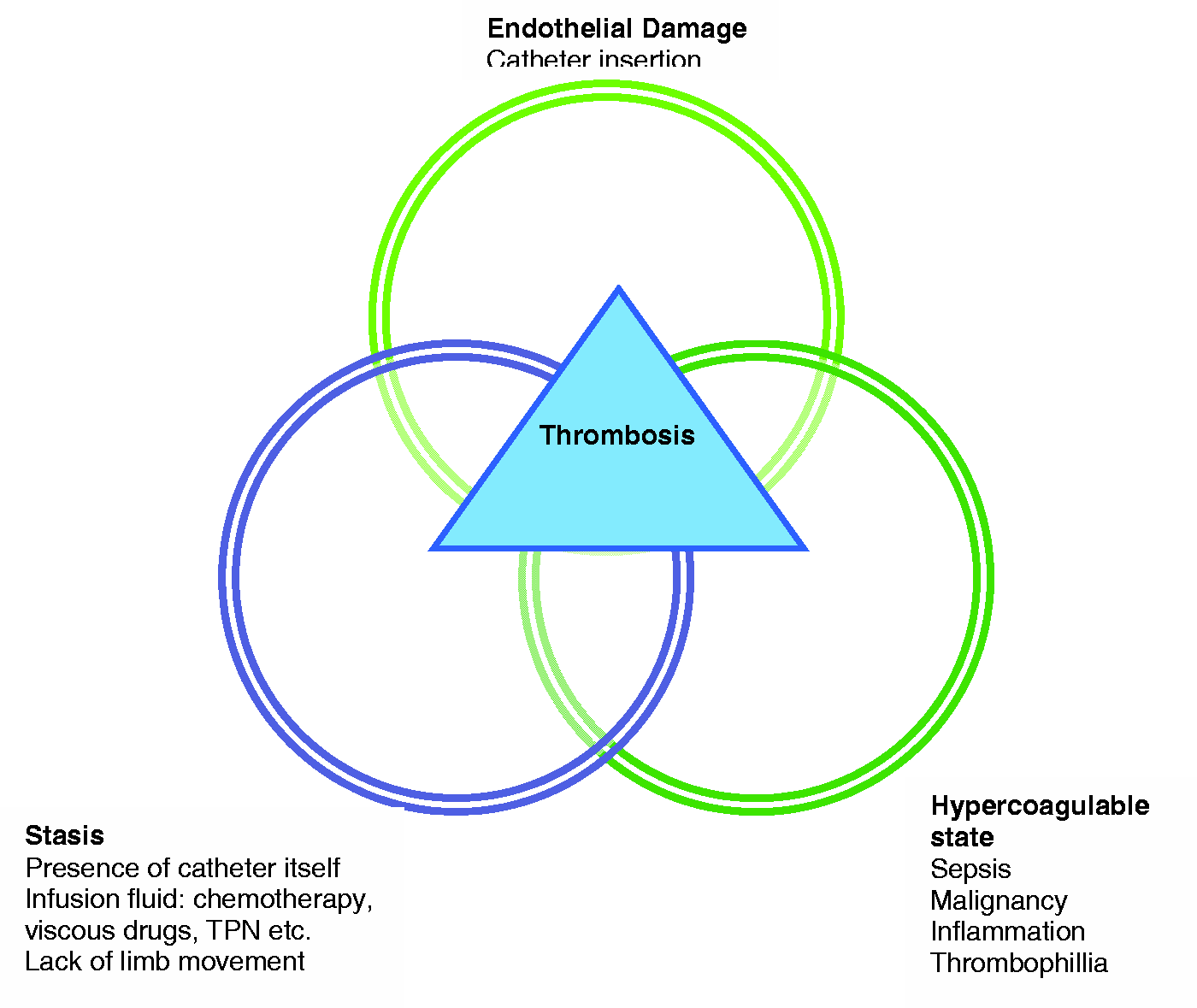
Postulated mechanisms by which the presence of a CVC may contribute to the development of thrombosis.
Prevention is better than treatment when it comes to CRT. Some of the risk factors for CRT such as (a) location of insertion and (b) the type of CVC are modifiable and careful consideration of these can minimise the risk for thrombosis. The International Society of Thrombosis and Haemostasis guidelines recommend that where possible, CVCs should be inserted on the right side, in the jugular vein with the tip located at the junction of the superior vena cava and the right atrium to minimise the risk of thrombosis.3,4
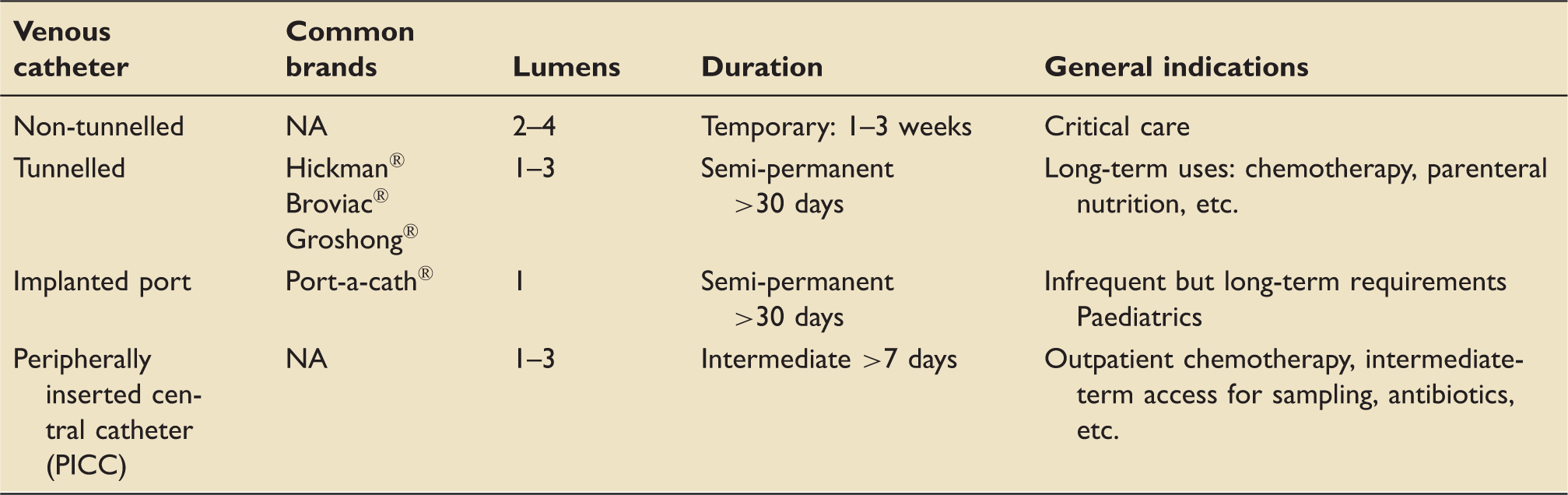
Summary of commonly encountered CVCs.
Sepsis is of course commonly encountered in critical care patients and is widely recognised as a risk factor for venous thromboembolism (VTE). In relation to CRT there is evidence to suggest this relationship endures. The presence of a CVC-related infection increases the risk of symptomatic CRT, with the highest rates seen systemic rather than localised infection. 13 It may be argued that the presence of catheter-related infection should prompt screening for CRT with ultrasound, even in the absence of other clinical features. 13
Clinical symptoms
Possible presentations of CRT.
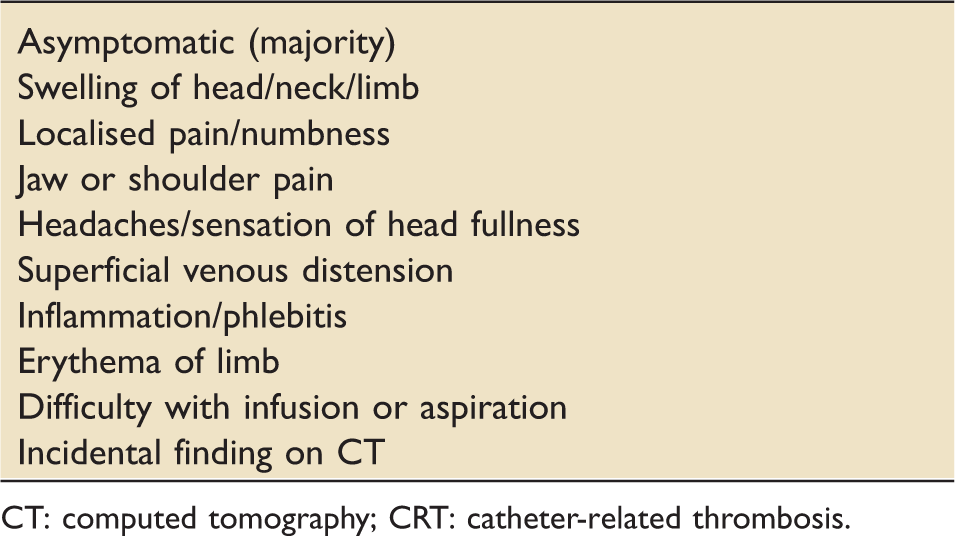
CT: computed tomography; CRT: catheter-related thrombosis.
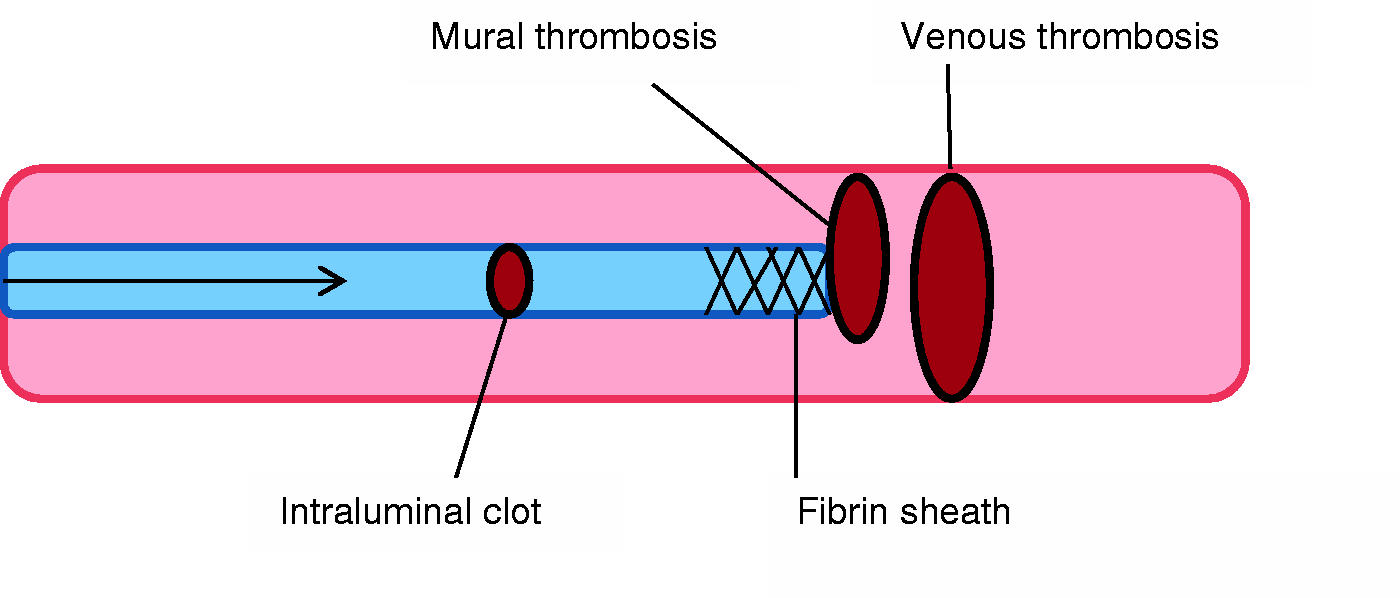
Schematic image of thrombotic events that may be associated with central venous catheters.
Is CRT the cause of symptoms?
Whilst it may be common practice in many centres to simply remove CVCs that are malfunctioning, difficulty with line aspiration or infusion may be secondary to CRT and a high index of clinical suspicion is required. It is also useful to consider other causes of line occlusion as some are amenable to simple measures. This is particularly relevant to patients with ‘precious lines’ such as those with difficult access
Check the tubing for mechanical obstruction such as a kinked line, an overtight suture or tip abuttal to vessel wall and inspect for a malpositioned port.
14
Repositioning manoeuvres include raising the ipsilateral arm, having the patient sit or stand, or rolling the patient onto one side may be helpful in these cases. It is worth reviewing preparations administered through the line. Lipid emulsions, such as parenteral nutrition, may leave a residue causing obstruction. These blockages may be amenable to instilling the line with a 70% ethanol solution, although no large studies have been conducted into this practice.
16
A medicines review can also yield clues as to the cause of obstruction as incompatible medications may precipitate within the lumen.
17
Occlusion by catheter thrombosis is the next consideration if no other cause is identified. In the case of an intraluminal clot or fibrin sheath formation (see Figure 2), lumen patency may be restored by instilling the line with a thrombolytic agent such urokinase which is commonly used in the UK and Europe. Urokinase 10,000 units/ml is reconstituted with 3 ml of 0.9% normal saline or water for injection. Each lumen of the occluded catheter is instilled with 5000 units of urokinase and left for 2 h.
18
An alternative thrombolytic agent to urokinase is alteplase, which has been shown in the cardiovascular thrombolytic to open occluded lines trial (COOL) to have a good efficacy and safety profile. Following the administration of 2 mg alteplase with a dwell time of 120 min, 78% patency was achieved with one dose, rising to 87% after a second.
19
Whilst the trial data on local thrombolytic therapy are not extracted from critically unwell patients, the doses of thrombolytic agents are small and for the majority of patients are unlikely to cause harm. It would however be prudent to review potential risks on an individual basis.
Complications
The consequences of CRT are not insubstantial; complications can include pulmonary embolism (PE) in 10–15%, loss of venous access in 10%, infection, post thrombotic syndrome (PTS) and delays in treatment.
2
PE: whilst thankfully rarely fatal, PEs are the most serious complication.
2
PTS: a chronic complication of VTE that manifests as oedema, chronic pain, a sensation of limb heaviness, and in the worse cases ulceration. It is thought that patients with large, proximal VTEs which fail to completely resolve are at the highest risk of developing PTS. Future lines: there is consensus on the criteria for line removal when CRT develops; however, there is no evidence to guide when it is considered reasonable to insert a new CVC. Clinicians must therefore assess the risks of further thrombosis against the urgency for central access.
Diagnostic approach
A ‘linogram’ (contrast study) may theoretically be used to confirm internal line kinking or the presence of an intraluminal occlusion, but it is not commonly performed. In practice, trial of a thrombolytic agent empirically may be used which is particularly useful in ‘precious’ lines that cannot be easily replaced. 14
Duplex ultrasound is the initial imaging modality of choice if a CRT is suspected clinically or if lumen patency is not restored with simple measures. 20 It is non-invasive and particularly reliable for assessing thrombi in anatomically accessible veins including the jugular, axillary, distal subclavian and arm veins. In the more proximal veins, sited inside the thorax, clearly duplex ultrasound is less sensitive.
If clinical suspicion of CRT is high despite a negative Duplex scan, then contrast venography may be considered as it is the ‘gold standard’ investigation but does confer risks associated with contrast and radiation exposure.14,21
It is worth noting that the use of the D-dimer assay has not been validated for use in patients with suspected CRT and is therefore not recommended for use in this context.18,22
Treatment
Factors to consider when treating CRT include
assessment of ongoing need for central access, the functional status of the line, the presence of an underlying prothrombotic state and review of any contraindications to anticoagulation.
Systemic anticoagulation
There is limited good quality data available for the systemic anticoagulation in CRT, particularly relating to critical care patients. Recommendations are therefore largely extrapolated from data for lower limb DVTs and small, non-randomised studies on CRT (of which a significant number are conducted on patients with malignancies).
3
Figure 3 provides a proposed treatment algorithm for the treatment of CRT.
Proposed treatment algorithm for patients with confirmed CRT.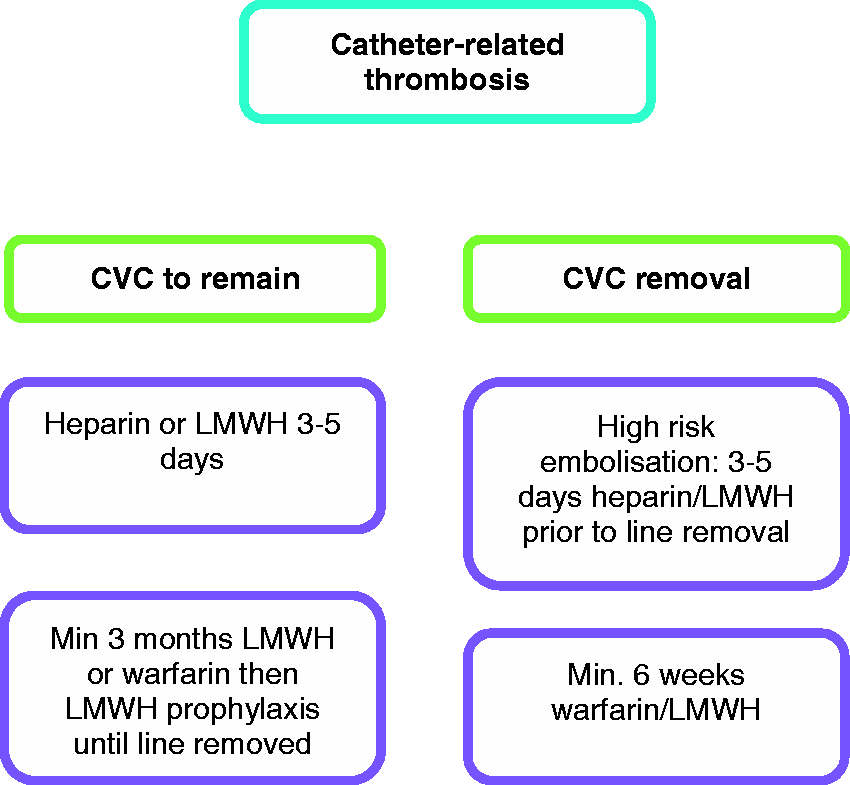
Consensus opinion for the treatment of CRT is for systemic anticoagulation for a minimum of three months.3,13,23 In patients with malignancy, treatment dose low-molecular weight heparin (LMWH) is recommended due to its superiority over vitamin K antagonists (VKAs) in preventing recurrent thrombosis.23–25 In critical care patients who frequently have unpredictable pharmacodynamics and are on multiple medications, this also confers the advantage of having fewer potential drug interactions which can be a problem with VKAs like warfarin. In patients with a rapidly changing clinical picture, such as developing acute kidney injury, LMWH may require monitoring with anti-Xa levels. In patients with extensive CRT and particularly high bleeding risk, the use of unfractionated heparin may also be considered due to its short half-life and ease of reversal.
If the catheter remains in situ beyond completion of three months anticoagulation, prophylaxis is recommended until line removal. 23 In patients without malignancy, VKAs may be commenced following an initial period of LMWH.
The duration of anticoagulation following line removal in patients without other ongoing thrombotic risk factors is again controversial due to a lack of good quality data. Some physicians continue to anticoagulate for three months whilst others shorten the duration. The decision making process should include thorough consideration of other potential risks for thrombosis, the size of the clot and the extent to which it occludes the vessel. Duration of six weeks’ anticoagulation may be appropriate if there are no risk factors and the clot is small and non-occlusive.14,23
There are no trials yet published using non-vitamin K antagonist oral anticoagulants (NOACs), although in the absence of malignancy, there is probably no reason to exclude their use for CRT. Trials are underway with the use NOACs in cancer patients with VTE.
Line removal
The current recommendations3,23 state that if the CVC is still required and functioning well, it does not have to be removed provided it
is well positioned is non-infected demonstrates good resolution of symptoms on surveillance.
The line should be removed if not all the criteria are met, if anticoagulation is contraindicated, if the thrombosis is life or limb threatening or if symptoms are not resolving.
The thrombocytopaenic patient
Treatment options in patients with CRT based on degree of thrombocytopaenia.

LMWH: low-molecular weight heparin.
Patients who develop thrombocytopaenia following anticoagulation with heparin should be reviewed to exclude heparin induced thrombocytopaenia (HIT).
Prophylaxis
Current guidelines, based on the evidence available, do not recommend anticoagulation for the routine prevention of CRTs,7,25,28,29 although it is expected that the vast majority of critical care patients will receive LMWH prophylaxis as standard care.
Previously, low-dose warfarin (1 mg/day) had been used for patients with indwelling catheters and malignancy 30 but subsequent trials disproved its benefit. 31 The largest contemporary trial, WARP (Warfarin thromboprophylaxis in cancer patients with CVCs) compared the use of adjusted dose warfarin (INR 1.5–2.0), low-dose warfarin (1 mg/day) and no anticoagulation in the prevention of CRT in cancer patients. 32 The data from this trial did find a benefit in CRT reduction in the dose adjusted arm but this was offset by increased bleeding risk. There was no significant benefit in taking low-dose warfarin.
In 2011, a Cochrane review analysed the available data on prophylaxis with UFH and LMWH in the prevention of CRT. It concluded that despite no increase in bleeding risk, there was also no benefit in the reduction of symptomatic thrombosis. 33
There is ongoing debate in respect to maintaining line patency with local measures. Following The National Patient Safety Agency (NPSA) report in 2008, which highlighted potential dangers associated with heparin flushes, the use of saline-only flush solutions was recommended. 34 This led to a dramatic fall in the use of heparin flushes in critical care, with some centres questioning if this has resulted in increased thrombotic complications and reduced catheter lifespan. Tully et al. performed an observational study of 445 arterial lines flushed with either saline or heparin solutions and found significantly decreased rates of line occlusion with increased catheter lifespan in the heparin group. 35 Whilst there is insufficient evidence to recommend the practice of flushing lines with heparin to maintain line patency at this time,28,36,37 it is an area that requires further evaluation with adequately powered, blinded randomised controlled trial.
Problem areas in relation to CRT
The increasing use of CVCs, and particularly increasing PICCs usage, will likely increase the incidence of CRT. Although most cases are easily treated, there are still some dilemmas when it comes to CRT. These include
Patients with thrombocytopenia – is not anticoagulating safe? Choice of catheters – there is ongoing debate on the relative risks of PICC and CVCs in regards to thrombosis and infection More data on sepsis/thrombosis relationship Absence of epidemiological data for complications
Probably the biggest issue in relation to CRT management is lack of best evidence.
Conclusions
CRTs are a relatively common occurrence with the potential for significant morbidity. Given that the majority of cases occur asymptomatically, a high index of suspicion is required for diagnosis. The non-invasive nature and sensitivity of venous duplex scanning lends this imaging technique to be the imaging modality of choice in the majority of patients. To date, there is insufficient evidence to support prophylactic anticoagulation in the prevention of CRT; however, careful consideration of modifiable risk factors prior to line insertion can reduce risk. Where feasible, CVCs should be inserted in the right jugular vein with the tip at the cavoatrial junction and despite the increasing usage of PICCs, acknowledgment of their propensity to increase CRT risk needs to be addressed. Providing that a line is still required, functioning, in the correct position and there is no evidence of infection, current recommendations advise against removal. Except in the lowest risk groups, three months systemic anticoagulation is generally recommended. In patients with malignancy, LMWH is the preferred anticoagulant, with warfarin being an alternative in patients without malignancy once their critical illness has resolved. The most pertinent issue to be derived from this report is the lack of good quality evidence on CRT in the critical care population. We are currently extrapolating data from the management of DVTs and small studies of CRT in patients with co-existing malignancy. Adequately powered RCTs are required to definitively establish how best to managed CRT in the critical care arena.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.