
Abstract
“May-Thurner syndrome” (MTS) or “Cockett’s syndrome” is a vascular disease in which the left common iliac vein is compressed against the spine by the right common iliac artery, very rarely by the left or by both common iliac arteries. The congenital form is even more rare and is due to an anomaly of embryological development. This case describes compression and thrombosis of the left common iliac vein. A 12-year-old girl reported for observation with fever and arthralgia in the left lower limb. Sonography and computed tomography revealed thrombosis of the left common iliac vein caused by a congenital reduction of the iliac-vertebral space. Due to the rarity and non-specificity of the symptoms related to MTS, patients can suffer from repeated thrombosis and potentially pulmonary embolism.
May-Thurner syndrome (MTS) 1 or “Cockett’s syndrome” 2 is part of the vascular compression syndromes that result from extrinsic compression of the left common iliac vein (LCIV), caused by the common iliac arteries. This can occur due to congenital or acquired reduction of the iliac-vertebral space, often causing thrombosis (See Figure 1). There are no unequivocal data reported in the literature on the incidence of MTS in children, but it is much rarer than deep vein thrombosis, which has an incidence of 0.07 to 0.14 per 10 000. 3
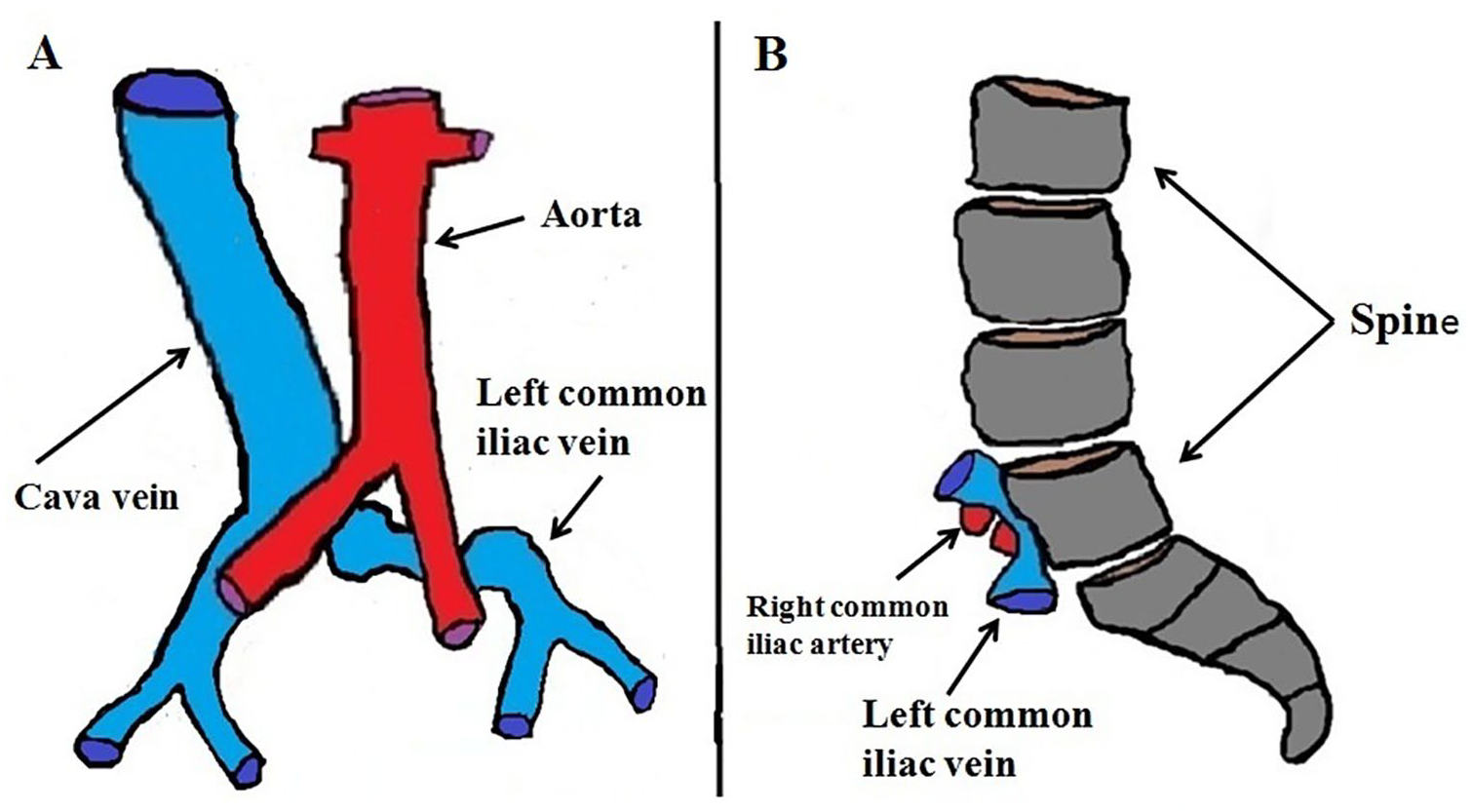
A diagram is provided that illustrates the anatomical relationships in patient with May-Thurner syndrome. (A) A coronal diagrammatic view is provided. (B) A compatible sagittal diagrammatic view is also provided.
In the acquired form, typical of adults, the iliac-vertebral space is reduced due to vertebral osteophytosis or calcifications of the common iliac arteries. However, when there are no causes of compression, it is believed that the reduction of the iliac-vertebral space is congenital. At least two mechanisms have been demonstrated at the origin of the syndrome: the narrowing of the iliac-vertebral space, which causes venous congestion, and the pulsations of the iliac artery. Over time, this can induce intimal fibrosis in the LCIV and the formation of intraluminal spurs that cause mechanical obstruction, hypertension, and thrombosis. 4 In most of the cases (84%), the LCIV is compressed by the right common iliac artery, infrequently by the left common iliac artery, and very rarely by both arteries. 5 Compression of the common iliac vein is an equally rare occurrence. 6 As in most vascular compression syndromes, the stenosis is often an incidental finding as it is mild and asymptomatic. The symptoms are typical of venous congestion with pain in the left lower limb and claudication. Clinically, limb swelling, lymphedema, thrombophlebitis, and thrombosis may occur. In more severe cases, pulmonary embolism 7 or spontaneous rupture of the iliac vein 8 may occur.
This pathology should be suspected in patients with repeated episodes of deep vein thrombosis of the left lower extremity or pulmonary embolism. Ultrasonography is the first-level diagnostic examination; however, the diagnosis can be made using magnetic resonance imaging (MRI), computed tomography (CT), or intravascular ultrasonography (IVUS). 9 Ultrasonography allows easy identification of LCIV compression and thrombosis and can provide an estimate of the stenosis degree, due to the flow ratio (FR) that is obtained from the ratio between the peak systolic velocity (PSV) post-stenotic and the PSV pre-stenotic. 10 If pulmonary embolism is suspected, the sonogram must be integrated with CT angiography. Treatment of MTS can be pharmacological or with endovascular stenting. May-Thurner syndrome can be a very debilitating chronic disease and, in most cases, is described in the literature, in predominantly elderly patients, caused by spondyloarthrosis or calcifications of the iliac arteries. The clarity of the diagnostic results and diagnosis will be helpful for a thorough understanding of the signs, symptoms, sonography appearance, and treatment options. A rare case of congenital MTS with LCIV thrombosis is provided.
Case Report
A 12-year-old girl came to the hospital for observation based on a fever associated with arthralgia of the left lower limb. On physical examination, the patient exhibited intact sensoriality, fair general conditions, and a body temperature of 38°C. Her weight was 36 kg and was measured at a height of 137 cm. Ultrasonography, CT, and laboratory tests were ordered and performed. The ultrasonography examination was completed with a May Lab 9 device (Esaote biomedica, Genoa, Italy) and two transducers that were a 1.5 to 8 MHz convex and a 5 to 14 MHz linear. The ultrasonography examination was performed by a medical professional with 20 years of experience. The CT was completed with Optima 64 slices device (GE Healthcare, Waukesha, Wisconsin). The LCIV caliber and distance between the common iliac arteries and spine were measured. On the CT images, the LCIV appeared obstructed by a thrombus extending from the confluence of the LCIV in the inferior vena cava to the iliac bifurcation, with an extension of approximately 3 cm (See Figure 2). The CT and ultrasonography measurements of the iliac-vertebral space were taken on the axial images (See Figure 3).
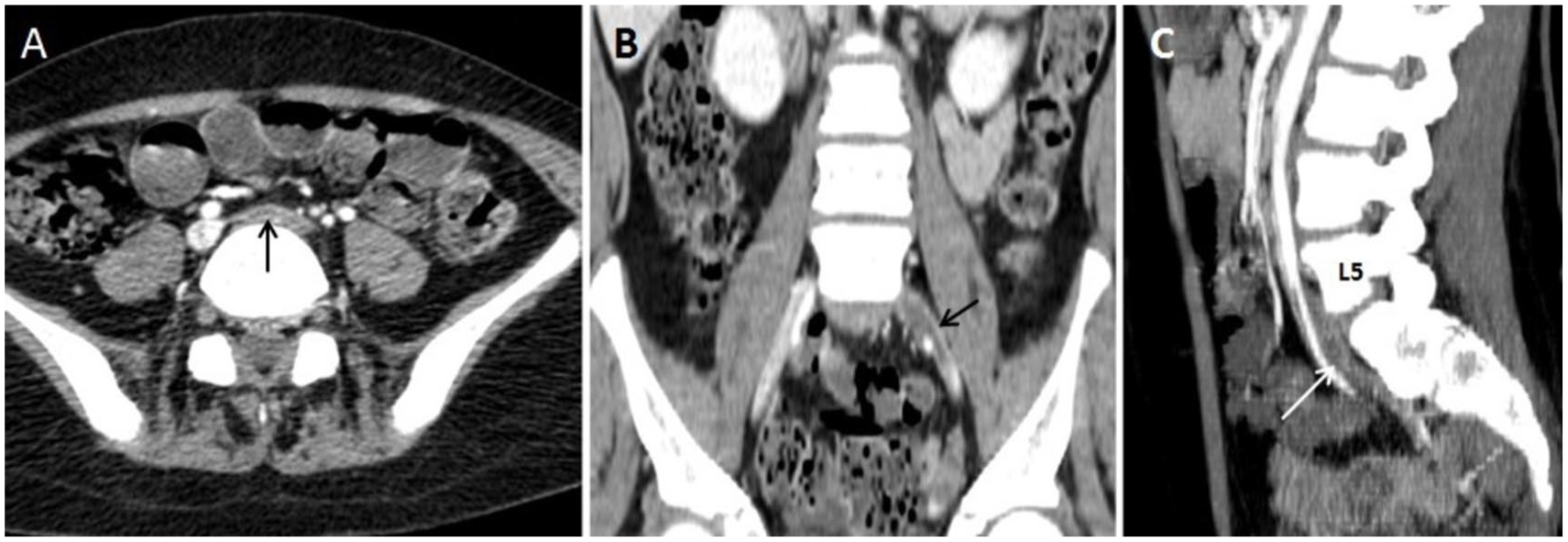
The detection of May-Thurner syndrome with computed tomography (CT). (A) An axial CT slice is provided of the iliac-vertebral space in axial, which showed an LCIV thrombosis (See black arrow). (B) A coronal CT slice demonstrated a thrombus (See black arrow) that obstructed the LCIV and extended from the iliac-vertebral space to the iliac bifurcation. (C) A sagittal CT slice indicated a thrombosis of LCIV (See white arrow) starting from the anterior wall of the fifth lumbar vertebra to the iliac bifurcation.
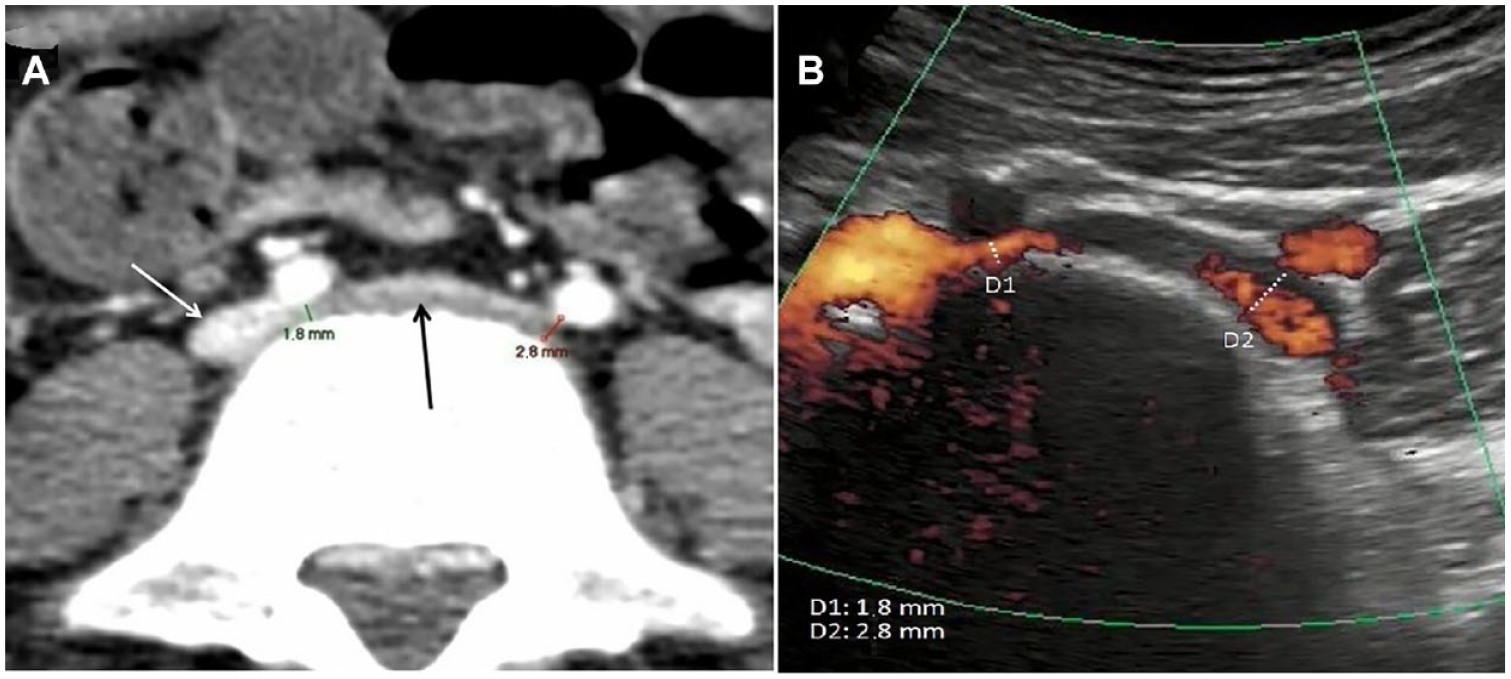
(A) An axial computed tomogram (CT) image showed the distance between right (1.8 mm) and left (2.8 mm) common iliac arteries and spine. The left common iliac vein is seen on the image (See black arrow). The inferior vena cava vein is also seen (See white arrow). (B) The sonogram allowed for the measurement of the stenotic tracts and, in this case, confirmed the data provided on the CT.
The ultrasonography examination also demonstrated significant narrowing (1.8 mm) of the space between the right common iliac arteries and the fifth lumbar vertebra with significant stenosis (>70%). The FR measurement is considered the best criterion for identifying a hemodynamically significant venous stenosis. When the FR is recorded, it can establish the degree of stenosis of the LCIV: an FR greater than 2.5 corresponds to a stenosis greater than 50%; if the stenosis exceeds 70%, it is considered hemodynamically significant. The CT excluded other causes of compression and other abdominal pathologies. The ultrasonography examination also confirmed LCIV thrombosis, which was characterized by the absence of flow signals (See Figure 4) (
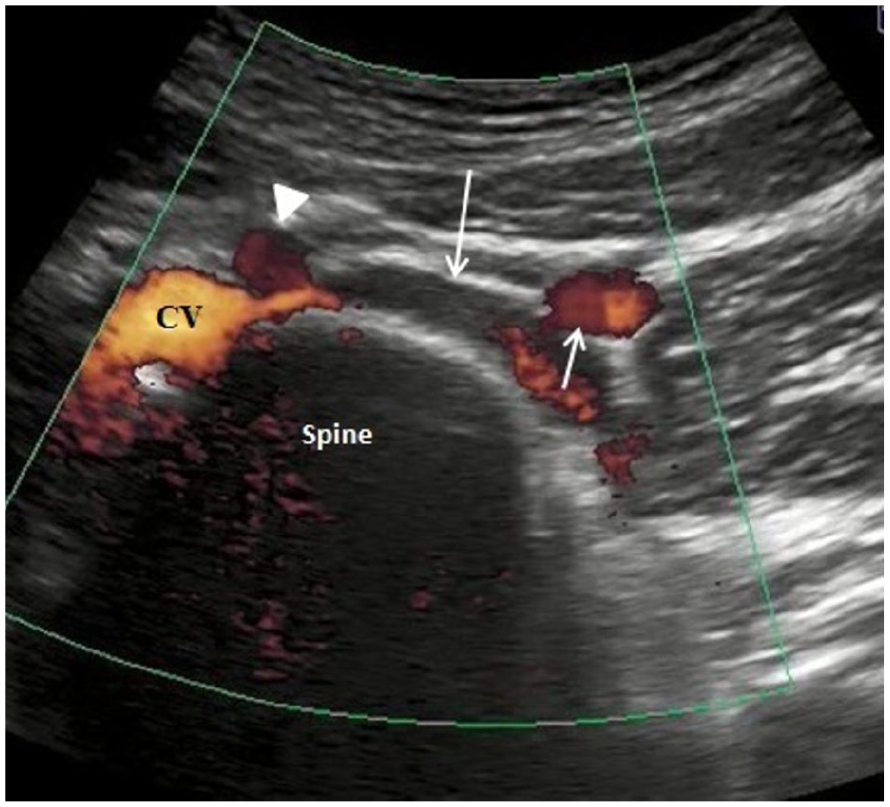
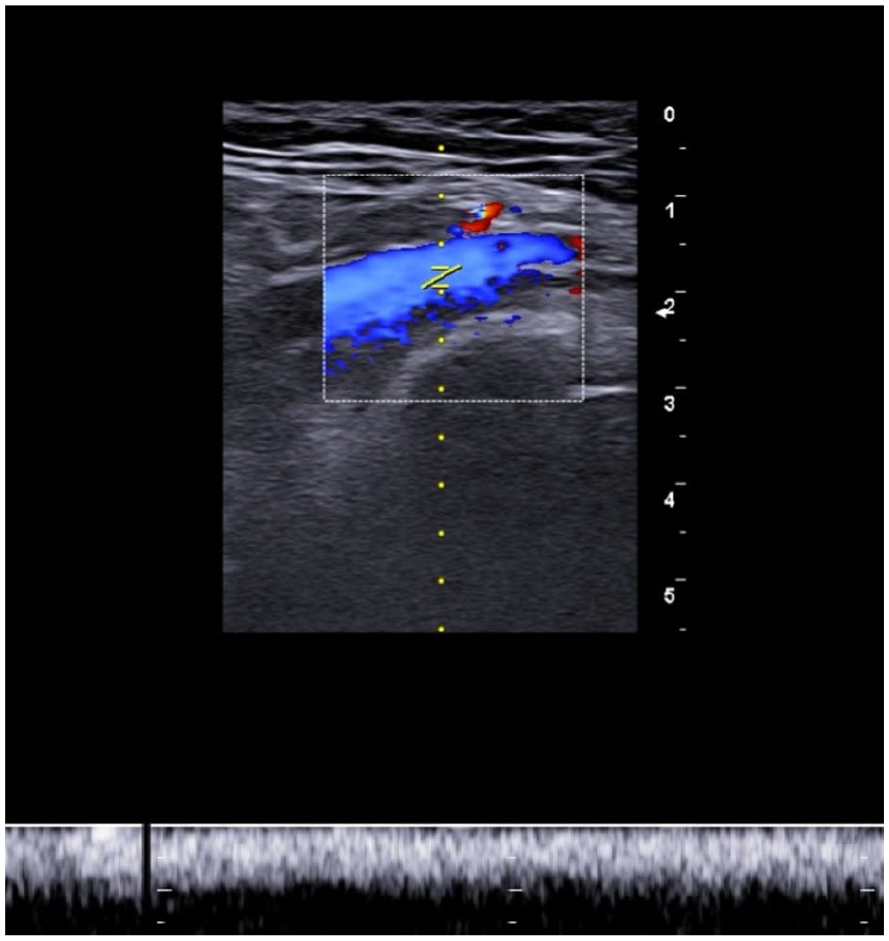
A power Doppler transverse image is provided and was performed with convex transducer, at the level of the iliac bifurcation, and highlighted the left common iliac vein (long arrow). It appears thrombotic, without flow signals, due to the compression exerted by the right common iliac artery (See white arrowhead). The inferior vena cava is labeled as CV.
The ultrasonography examination showed no alterations in the right iliac vein, which had a maximum diameter of 12.3 mm, a minimum diameter of 9 mm, and a PSV of 18.7 cm/s. The patient was treated with high-dose antiplatelet therapy and after 1 month, a repeat ultrasonography examination confirmed the restoration of regular flow in the LCIV (See Figure 5).
The Doppler examination, performed 1 month later after therapy, demonstrated proper vascular flow, in the left common iliac vein.
Discussion
In healthy pediatric patients, the distance between the common iliac veins and the spine ranges from 8 to 12 mm. The diameter of the LCIV ranges from 12 to 14 mm and the diameter of the right common iliac vein (RCIV) ranges from 12 to 16 mm. The LCIV crosses the iliac-vertebral space between the right common iliac artery and the spine, 11 at the level of the fifth lumbar vertebra, before joining the inferior vena cava. In MTS, this space is significantly reduced, to below 3 mm and can cause compression of the LCIV. When the LCIV is compressed, the pre-stenotic and post-stenotic tracts dilate and the vascular flow diminishes. If the compression is mild (<50%), 12 it is generally asymptomatic, but if it increases (>70%), it can become symptomatic, causing the typical signs of venous congestion. The management of patients affected by MTS, as for other vascular compression syndromes, is complex and to set a correct therapeutic setting it is necessary to first exclude other causes of compression: neoplastic masses, 13 aneurysms, 14 pseudoaneurysms, surgical outcomes, or other pathologies. It is equally important to know the extent of stenosis extent and, if present, thrombosis, as all this diagnostic information allows for the most appropriate treatment to be chosen. Compression of the LCIV is often asymptomatic and is usually highlighted in tests performed for other pathologies; this is generally due to mild compression, or in more severe cases to the presence of collateral circulation that decongests the flow of the LCIV. In these cases, even if asymptomatic, it is necessary to quantify the compression entity as even stenosis of less than 50% can cause clinical manifestations; in the literature, stenoses greater than 25% are reported in 66% of MTS cases 15 and only in 24% of cases greater than 50%, therefore, even if not hemodynamically significant, compressions can cause the syndrome. Ultrasonography plays a fundamental role in the diagnosis and above all in determining the degree of stenosis degree, which dictates the type of treatment. The ultrasonography measurement of the degree of stenosis is based on Doppler of the LCIV and is obtained from the difference between the PSV of post-stenotic tract and PSV of pre-stenotic tract (FR). 16 It may be useful to perform measurements of the caliber and PSV of the right common iliac veins 15 to highlight flow deficits in the LCIV. In the current case, it was not possible to measure the FR, due to the complete thrombosis of the LCIV which therefore represents a limitation of the method. In asymptomatic cases, the extent of compression must be monitored over time to prevent worsening, but if their stenosis degree is greater than 50%, patients should still be subjected to long-term low-dose antiplatelet drug therapy to avoid LCIV thrombosis. In symptomatic patients, a conservative therapeutic approach could be adopted with high-dose antiplatelet drug therapy or treatment with endovascular stenting could be considered. 17 This is predicated on the risks associated with the procedure such as the stent migration or obstruction. Other procedures have also been proposed, some of which are very effective such as thrombectomy 18 associated with antiplatelet drug therapy. In severe cases with repeated episodes of pulmonary embolism, the possibility of positioning a vena cava filter 19 should also be evaluated. In the current patient, due to the extremely narrow iliac-vertebral space, it was not possible to resort to stenting, as it did not guarantee good long-term stability. Given these facts, the best course of action was a pharmacological treatment with high-dose antiplatelet agents was administered, which allowed the resolution of thrombosis, in a month. The patient was then advised short-term ultrasonography surveillance (3 months) and long-term low-dose antiplatelet therapy.
Conclusion
Vascular compression syndromes are rare, poorly understood, and difficult to diagnose due to nonspecific symptoms. May-Thurner syndrome causes chronic thrombosis and, in severe cases, pulmonary embolism. Diagnostic cut-off values of the iliac-vertebral distance, below which the syndrome occurs, have not yet been reported in the literature. This may be due to the limited case series present and makes it difficult to classification of patients at risk and their management. In all patients with deep vein thrombosis of the left lower limb, it is recommended to extend the study to the iliac-vertebral space to exclude MTS, especially in fragile patients such as children and pregnant women. Failure to diagnose can expose you to serious health risks. Disclosure of these cases can significantly contribute to reducing the number of false negatives and increasing awareness of this rare disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
A waiver of informed consent was granted as part of the ethical approval before the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.