
Abstract
Objective:
The objective of the study is to identify any intergroup differences or statistically significant correlations between paraspinal intramuscular adipose tissue (IntraMAT) deposition and variables such as low back pain, gender, self-reported activity level, body mass index (BMI), age, and academic class-year, as measured by sonographic intensity analysis. This study is specific to a cohort of first- and second-year medical students.
Materials and Methods:
The right lumbar paraspinal muscles, at the level of the fifth lumbar vertebrae, were investigated with sonography among a cohort of medical students. Image pixels, within the selected region of interest, were segregated by pixel intensity and analyzed for IntraMAT content. Participants reported on additional study variables by responding to a survey. The cohort responses were analyzed to seek correlations between those variables and IntraMAT.
Results:
The female participants were found to have more IntraMAT (P < .001). Most participants reported low back pain. There were no significant correlations between IntraMAT and reported low back pain, academic class year, or BMI. Moderate exercise increased IntraMAT deposition, and each year of increasing age decreased IntraMAT (P < .05). Second-year students experienced more self-reported low back pain than first-year students.
Conclusion:
A cohort of medical students who were reportedly sedentary had more low back pain than their peers. Back pain was more prevalent in second-year students, irrespective of age, suggesting that ill effects of a sedentary lifestyle may be cumulative. The validity of the sonographic pixel intensity analysis performed was supported by the highly significant increase in IntraMAT observed in female participants. The relationship between low back pain, exercise, BMI, and IntraMAT was uncertain based on available evidence and the results of this study.
Keywords
Sonography has a myriad of evidence-based uses across many medical specialties, 1 and many new clinical applications have emerged. One such emerging application is the analysis of changes in skeletal muscle composition, using sonographic pixel intensity analysis. 2 Adipose associated with skeletal muscle can accumulate between the muscles (external to the epimysium) or integrate between the muscle fibers that comprise the muscle (internal to the epimysium). These fat deposits are termed intermuscular adipose tissue (InterMAT) and intramuscular adipose tissue (IntraMAT), respectively. 3 Studies have suggested that increases in IntraMAT may be linked to metabolic disorders, infectious diseases, decreased muscular strength, and low back pain (LBP).4–9 It seemed important to add to the evidence on documenting IntraMAT with the use of sonography.
Lean muscle has lower sonographic pixel intensity and appears hypoechoic when compared with muscle, with higher levels of IntraMAT,10,11 or fibrous connective tissue. 12 They both have a higher sonographic pixel intensity and appear more hyperechoic. Magnetic resonance imaging (MRI) T1-weighted images remain the diagnostic gold standard for assessing tissue composition, as it can be used to delineate changes in soft tissue structure and differentiate between IntraMAT and skeletal muscle components.13,14 However, several studies have demonstrated that diagnostic sonography, which is less expensive, more convenient, and safer for patients, 15 has moderate to strong performance correlations compared with MRI, in determining adipose infiltration of skeletal muscle.16,17
The importance of evaluating the quality of IntraMAT, in patients, in addition to muscle quantity (i.e., cross-sectional area, CSA), has been increasingly recognized. Loss of muscle strength with aging cannot be totally accounted for by the decrease in muscle volume. Diminished muscle quality is likely to play a major role as well. 18 Muscle disuse consequent to limb immobilization demonstrates greater loss of muscle quality than muscle quantity in young adults. 2 In addition, IntraMAT has been shown to impair muscle contraction in experimental animals 19 and has been associated with muscle inflammation in the elderly. 20 Appreciation of the potential role of IntraMAT in patients with musculoskeletal (MSK) concerns is growing, but further research evidence is needed.
Low back pain is a common MSK issue affecting people of all ages, races, and gender.21–23 Failure to appropriately diagnose and treat LBP may lead to adverse effects such as impaired daily activities, anxiety, depression, and reduced quality of life. 24
Low back pain may be stratified etiologically as mechanical or nonmechanical,25–27 or chronologically as recurrent (RLBP) or continuous low back pain (CLBP). 28 Most reported back pain falls under the mechanical diagnostic spectrum. Mechanical issues are identified as those directly affecting the bony and ligamentous structures of the spine and surrounding soft tissues. 25 Identifying the source of nociceptive signals in patients is often difficult, complicating treatment. 21
The cause of LBP is often a mystery, but patients typically recover quickly. In some instances, recovery is transient, and the pain recurs (RLBP). 21 Studies have estimated the frequency of recurrence within 12 months after recovery to be as low as 24% 29 and as high as 69%. 30 Long sitting times and two or more previous episodes of back pain foreshadow a recurrence. 31
In a small number of patients, back pain becomes chronic, with few or no pain-free intervals. Available data suggest that the incidence of CLBP is increasing as the population ages.32,33
One approach to study LBP is to use diagnostic imaging to assess the quantity (CSA) and/or quality (IntraMAT) of the paraspinal muscles. The relationship of paraspinal muscles IntraMAT levels to LBP is complex. In one study, patients with CLBP had decreased paraspinal muscle CSA and increased IntraMAT when compared with healthy controls. 34 A similar study evaluating RLBP saw no change in the CSA of paraspinal muscle but did see an increase in IntraMAT. 35 Still other studies saw no association between RLBP and IntraMAT levels, indicating the need for more investigation. 36
Muscle quantity and quality are correlated with physical activity and can be modified by behavior. Exercise has been associated with lower IntraMAT levels while sedentary behaviors correlate with increased IntraMAT.20,37,38 In this respect, medical students provide an interesting cohort to evaluate, due to their relative inactivity. While medical students are typically young, active adults upon admission, navigating a rigorous curriculum imposes copious study time and often sedentary behaviors. 39
Materials and Methods
Study Design
A cross-sectional study cohort was recruited to explore relationships between paraspinal IntraMAT accumulation, as measured by sonographic pixel intensity analysis, and gender, age, body mass index (BMI), self-reported physical activity levels, time in medical school, and self-reported LBP. This study was approved by the host institution’s Institutional Review Board (IRB #2022-036).
Equipment
Body mass index was determined using a Tanita WB-3000 digital physicians scale with built-in stadiometer and BMI calculator (Tanita Corporation of America Inc.). An MX7 ultrasound equipment system (Mindray Medical International Ltd. China) and a curvilinear transducer with a transmit frequency of 1 to 5 mHz were used for all image acquisitions. The images were all uploaded into ImageJ software (National Institutes of Health and the Laboratory for Optical and Computational Instrumentation v.2.3.0/1.53q, build d544a3f481) to analyze each image.
Participants
The recruitment of participants was initiated via institutional email and was open to first- and second-year medical students enrolled at an accredited College of Osteopathic Medicine, located in the United States. Individuals with a BMI greater than 30, pregnant individuals, and persons with a history of spinal surgery were excluded from participation, for logistical reasons related to image acquisition. Participants were fully informed of the benefits and risks of participation and freely signed an informed consent form as part of the enrollment process. Participants were allowed to withdraw from the study at any time.
All participants underwent a BMI screening where their height and weight were measured to calculate their BMI. Students completed a survey (see Supplemental Appendix 1 QR CODE) that collected descriptive statistics, physical activity level, and self-reported information about experiences with LBP. Questions regarding LBP were adapted from the well-validated International Physical Activity Questionnaire. 40 All surveys were administered using Qualtrics XM (Qualtrics International Inc., Provo, Utah).
Sonograms were performed by a two-person team of trained sonographers. The sonographers received 4 hours of MSK sonography training from a sonography faculty member and the initial half of all the sonograms were directly overseen by this faculty member. Both researchers were present during each sonogram and both validated transducer placement, prior to image capture, to enhance reproducibility. For each participant, there were two sonographic images of the right paraspinal muscles, at the level of fifth lumbar vertebrae (L5), which were acquired using a practiced, methodical process (see Supplemental Appendix 2 QR CODE). The first sonographic image was captured using the base settings on the Mindray system and the MSK preset was selected (e.g., depth: 6 cm, gain: 55). For the second sonographic image, the gain and depth were optimized by the operator to maximize perceived image quality for each participant. All sonographic images were exported to an encrypted flash drive to be uploaded into Image J software for analysis.
Image Analysis
The images were imported into Image J for sonographic pixel intensity analysis. Each image was traced using the polygon selections tool. Two researchers independently performed the tracings. These individuals trained together extensively prior to the launch of this study to minimize variation in the tracing process. The tracing encapsulated the paraspinal muscle but excluded the bordering hyperechoic fascia. Image J was then used to generate output in the form of tables and histograms, to allow for both stratified numeric and stratified visual representations of the quantity of pixels, within the traced region. The units used in these histograms are arbitrary units (A.U.) and span from 0 (black pixels) to 255 (white pixels). The pixel intensity leveling and normalization of histogram data consisted of adjusting the beginning of the histogram to the beginning of the pixel intensity scale. This step assured that all histograms start at the same pixel intensity point at 0 (black). Histogram data were normalized (percentage scale) and were further divided into quintile bands consisting of 50 A.U.s each. Assessment of histogram quintiles rather than overall mean was shown to be advantageous in a previous study. 41 These data were used for statistical analysis.
Metabolic Equivalent of Tasks Calculation and Statistical Analysis
Activity data reported on the IPAQ survey were converted to metabolic equivalent of tasks (METs) by assigning a standard value to each reported activity (walking = 3.3 METs; moderate intensity activity = 4.0 METs; vigorous intensity activity = 8.0 METs) and multiplying by minutes engaged. Pixel intensity data extracted from Image J analysis were compiled, managed, leveled, and normalized using Microsoft Excel v.2306 (Microsoft Corporation, Redmond, Washington). All descriptive statistics and mean calculation statistical analysis were performed on SAS/STAT v.9.4 (SAS Institute Inc., Cary, North Carolina). Descriptive statistics and mean calculation were obtained using PROC FREC and PROC MEANS in SAS, respectively.
Leveled and normalized pixel intensity histogram quintiles (based on US A.U. counts dividing the 0-255 scale into five equal bands) were defined as the dependent variables while demographic data (class, age range, BMI, and gender), activity levels (METs: hours a week walking, doing moderate intensity activity, doing vigorous intensity activity, total active time, and sedentary time), and pain effects (having pain in the last 6 months, having pain <50% of the time, having pain today, and seeking treatment) were defined as independent variables. Demographic variables and pain effects were defined as categorical variables, while activity levels were defined as continuous. Associations were estimated using generalized linear mixed models (GLMMs) using individual subject measurements and repeated measurements effect by participant. Normality assumptions displayed no deviations as assessed in preliminary residual plots. For these models, covariance structures within subjects were optimized to achieve the best fit based on residual log-likelihood fit statistics (Akaike information criterion [AIC] and Bayesian information criterion [BIC]); the banded Toeplitz structure was selected as the best fitting covariance structure. This covariance structure effectively accommodates covariance across ordered sets of data 42 such as the pixel intensity histograms quintile bands. All modeling analyses were performed using PROC MIXED in SAS. Significant differences were declared at P ≤ .05.
Results
Participant Demographics and Self-Reported LBP
The cohort consisted of 78 first- and second-year osteopathic medical students. Their ages ranged from 21 to 46 years. Sixty percent of the participants were biological males and 40% were biological females (see Table 1, panel A). Of 78 participants, 42 (53.8%) had experienced LBP within the last 6 months, and 35 of those 42 (83.3%) reported LBP occurring less than 50% of the time. Of 42, 15 (11.9%) reported having LBP at the time of scanning, while 21 (50.0%) of participants reported having sought treatment for LBP in the past. Low back pain data aggregated by class-year and gender are depicted in Table 1, panel B.
Participant Demographics and Self-Reported Lower Back Pain Responses.
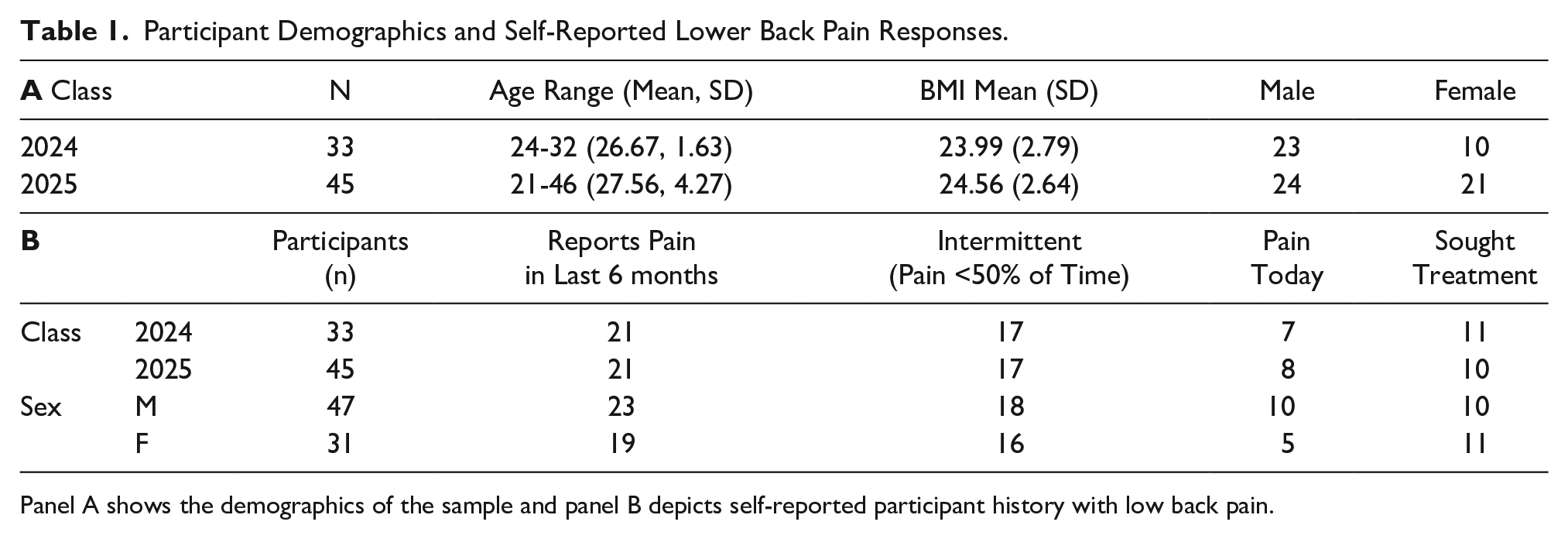
Panel A shows the demographics of the sample and panel B depicts self-reported participant history with low back pain.
Participant Self-Reported Activity
Activity data were reported by participants as average minutes per day of walking, engaging in moderate activity, and engaging in vigorous activity. Guidelines for activities to include in each category were provided to participants (see Supplemental Appendix 1 QR CODE). These data were converted to METs (h/wk) and used for analysis. 43 The average total METs across all participants was calculated to be 26.1 h/wk.
Total time spent exercising per week was calculated by multiplying vigorous exercise minutes by two and adding minutes spent in moderate exercise. 44 Using this calculation, 90% of women and 79% of men who reported exercise frequency met or exceeded the 150 minutes of physical activity per week recommended by US Department of Health and Human Services (DHHS) guidelines. 45
Time spent seated while studying was reported as average hours spent seated each day. The average time spent seated was 9.8 h/d across all participants (9.7 hours in the class of 2024, and 9.8 hours in the class of 2025). Activity and time spent seated data aggregated by class-year and sex can be seen in Table 2.
Participant Self-Reported Mean Activity Levels per Week.

Activity data were reported by participants as average minutes per day of walking, moderate activity, and vigorous activity; these data were converted to metabolic equivalent of task (MET) hrs/week and used for analysis.
Intramuscular Adipose Tissue Measurement
Statistical analysis comparing the data generated using the default MSK preset (see Figure 1, panel A) and the sonographer optimized settings (see Figure 1, panel C) from each participant did not show any differences. Therefore, all analyses reported in this work were generated using the Mindray MX-7 preset MSK settings.
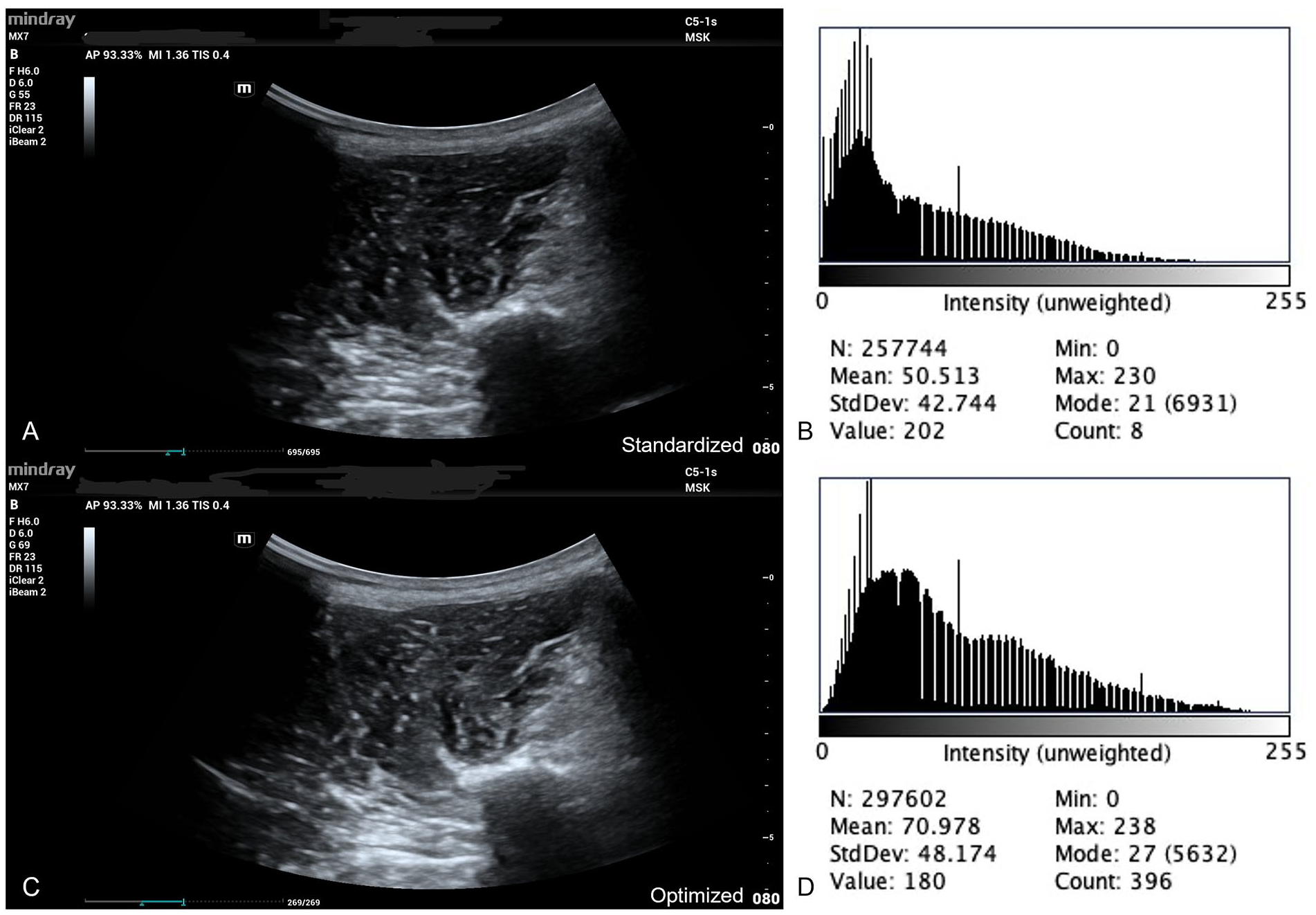
Sonograms of the left paraspinal muscles acquired using a standardized approach using default MSK machine settings (panel A), and an optimized gain-adjusted approach (panel C) for optimal visualization are shown. Panel B depicts the sonographic pixel intensity analysis output histogram generated from the pixels within the paraspinal muscles seen in the “standardized” image in panel B. Panel D is the histogram generated from the paraspinal muscles of the “optimized” image in panel C.
Analysis of quintile bands showed that women have an increase in IMAT compared with men (P < .001). On average, with each increasing year of age, participants showed a decrease in IntraMAT (P < .05). Participants with higher reported moderate activity METs (h/wk) showed an increase in IntraMAT (P < .05). The largest effect observed was for gender, followed by activity level. These findings are presented in Figure 2. Significant values that were identified were predominantly found on the left side of the histogram (pixel intensity values closer to zero). This suggests that effects are more evident in the dark end of the scale, which indicates less IntraMAT.
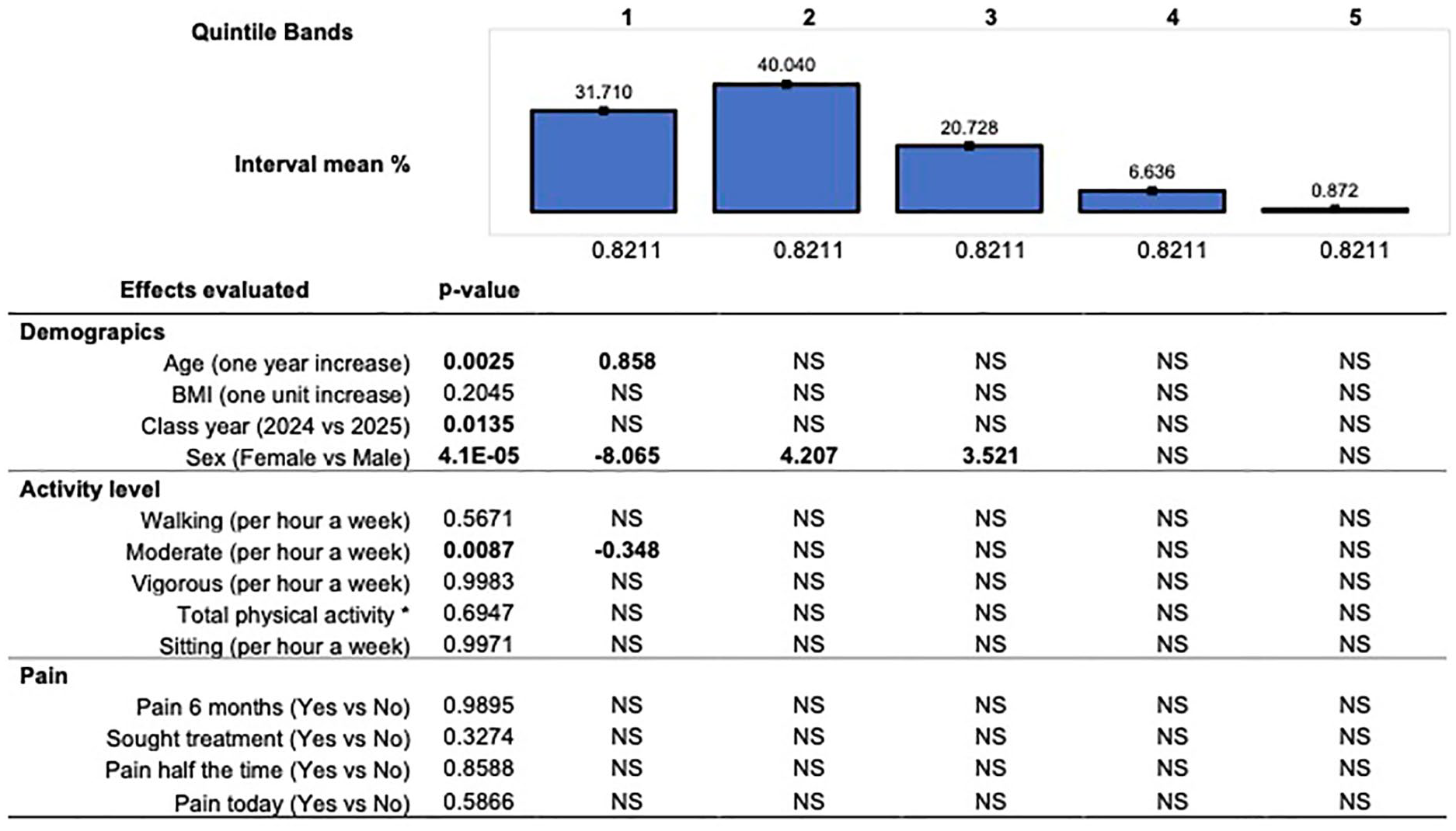
The effect size and association of demographic, activity level, and pain to histogram quintiles. Quintile bands represent sonographic pixels intensity that fall into five equally divided arbitrary unit ranges from darker pixels with less adipose (left bands) to lighter pixels with more adipose (right bands). p-values were declared significant at p < .05.
Results failed to show significant increases in IntraMAT in participants with a higher BMI (within our range of BMI:18-29), longer time spent in medical school (class year), and reported LBP variables. Table 3 displays the mean differences in arbitrary units across all variables in quintile bands (50 A.U.) of IntraMAT measurement.
Combined Associations of LBP Frequency Versus Other Measured Variables.
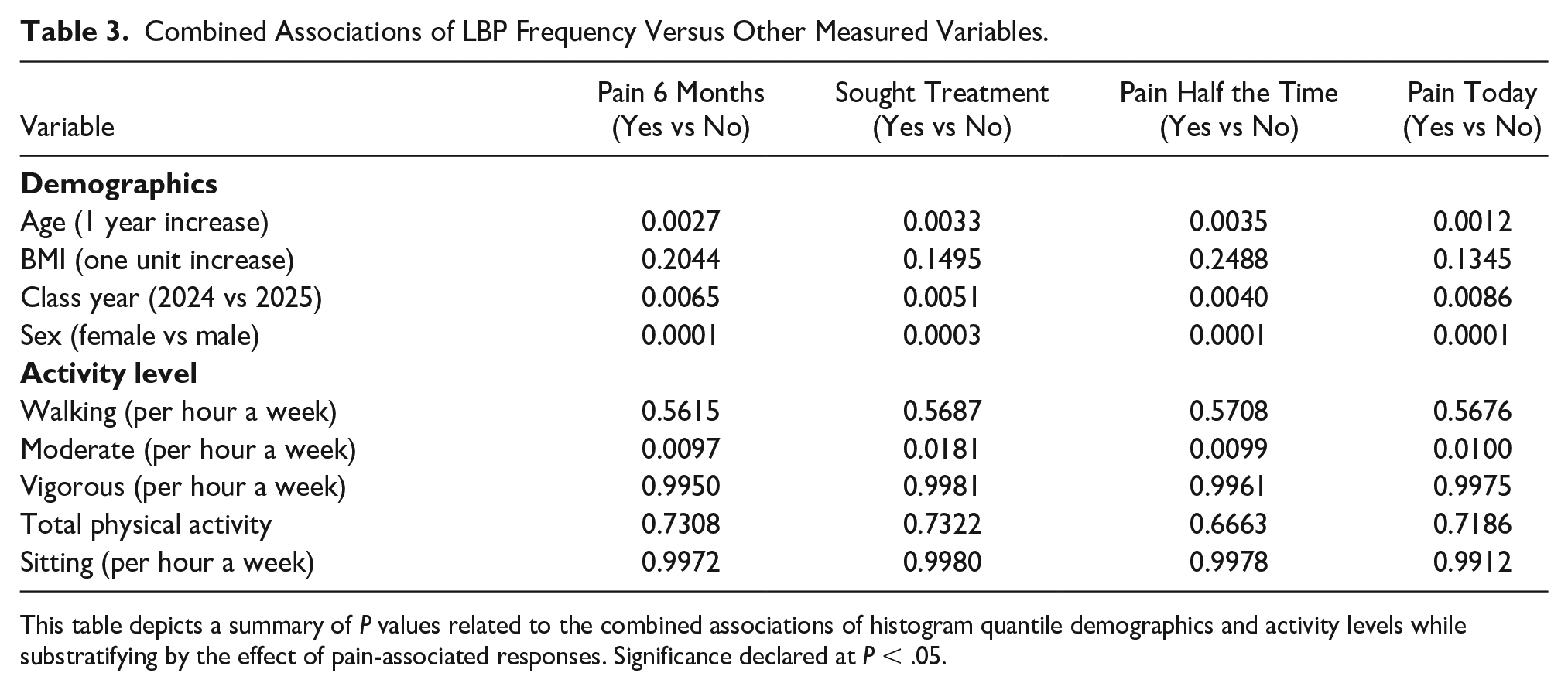
This table depicts a summary of p-values related to the combined associations of histogram quantile demographics and activity levels while substratifying by the effect of pain-associated responses. Significance declared at p < .05.
Discussion
Use of Sonography for the Assessment of IMAT Levels
This study used sonography as a diagnostic tool to assess IMAT levels in a unique cohort of medical students. The MRI is considered the gold standard for assessment of IMAT and has a long and successful track record for this use. Unfortunately, access to MRI equipment and the costs associated with image acquisition make this diagnostic imaging choice unavailable, for many researchers. Sonography has recently been shown to have utility in IMAT analysis. Sonography has the advantages of low cost and facile deployment in non-clinical settings. Very few studies to date have used this diagnostic imaging choice for IMAT analysis, and direct comparisons between MRI and sonography are lacking. More studies using sonography for IMAT analysis are needed to fully assess its value. This study provides additional evidence for the use of sonography in this area.
Low Back Pain in Medical Students
Lower back pain is often considered an affliction of middle age and is a major cause of debilitation in individuals over 60 years of age. 46 However, younger adults are not inexperienced with LBP. It is the most prevalent source of pain in adults, including those aged 18 to 29 years. 23 Lower back pain may be associated with sedentary lifestyles in younger adults and manifest through fatty infiltration (IntraMAT) of the paraspinal muscles.47–52 These associations were examined in preclinical medical students, a unique cohort prone to sedentary behaviors imposed by a demanding curriculum. Based on a limited search of the literature, activity levels, back pain, and sonography used to determine IntraMAT levels, in the paraspinal muscles, have not been assessed in medical students, at a North American institution.
A search of the published literature uncovered very few studies examining LBP in medical student populations overall and none looked at osteopathic students or students training in the United States.53–58 Therefore, expectations for the prevalence of LBP in this study were garnered from a National Center for Health Statistics (NCHS) study that reported 28.4% of 18- to 29-year-old adults, in the general population, had experienced LBP in the preceding 3 months. 59 This age demographic most closely aligns with that of this study’s cohort (e.g., average age = 27).
When compared with the NCHS study, the prevalence of LBP, in this cohort, was unexpectedly high. Fifty-four percent of participants in our study experienced LBP within the preceding 6 months, nearly twice the anticipated prevalence. There was an association between frequency of LBP and time spent in medical school. Forty-six percent of the first-year students in this study reported episodes of LBP. That increased to ~64% in second-year students, suggesting that cumulative time spent sedentary may have an adverse effect on back health. Reported LBP was recurrent in 81% of participants. The remainder (19%) was continuous. The level of LBP experienced by sufferers was often significant enough to interfere with normal daily activities and to seek treatment for. Consistent with published reports, women were more likely to have experienced LBP in the prior 6 months than their male classmates.22,60,61
Imaging IntraMAT
IntraMAT has been used in numerous studies as a surrogate for muscle quality. Increased IntraMAT has been associated with deleterious changes due to aging, obesity, and various acute and chronic diseases.4,7,8,62–65 Most germane to the current study, IntraMAT has been examined in the paraspinal musculature in the context of scoliosis, spinal degeneration, and LBP using well-established MRI or computed tomography (CT).62,66–68
Recently, sonography has shown utility in assessing IntraMAT in axial and appendicular skeletal muscle.5,16,17,69–73 Sonography was used in this study for its convenience and accessibility in a nonclinical setting.
When data collection for this study began, there was no clear guidance from the literature on optimal sonography equipment settings for IntraMAT quantitation. Therefore, two sonograms were performed on each participant, one examination using manufacturer default settings (Mindray-MSK) and one examination optimized by the operator. Downstream data analysis indicated that optimization of the images was not useful and did not influence IntraMAT analysis. Therefore, only data obtained using the default MSK settings have been reported in this article. Experiences garnered from this study would argue against including manual image optimization in future studies of this nature.
Exercise and Inactivity Levels in Medical Students
IntraMAT is not a static entity. Increasing age and sedentary behaviors can increase IntraMAT levels, while physical activity can protect against IntraMAT deposition.62–64,68,74–76 Assessment of IntraMAT levels may provide insights into current or impending health issues and monitor the efficacy of interventions.
Medical students represent an intriguing cohort to evaluate the interplay between physical activity and sedentary behaviors. Most medical students fall into the 18 to 34 age range, which represents the peak years of physical activity for adults. In the general population, ~ 41% of men and 28% of women meet the DHHS recommendations for physical activity levels. 77 As expected, the rigorous academic program needed to adequately train physicians imposes a more sedentary lifestyle on medical students than others in their age group. Study participants averaged just below 10 hours per day (class of 2025, 9.82 hours; class of 2024, 9.70 hours), 7 days a week, engaged in sedentary activity. This total far exceeds the 6.4-hour total “time spent sitting” average for American adults. 78
Despite this constraint, this study cohort still found the time and energy to exercise regularly. About 78% of men and 90% of women in the study who reported exercise frequency met or exceeded 150 minutes of exercise/week recommended by the DHHS, a surprisingly high fraction when compared with the general population. 77
Physical activity has been shown to decrease IntraMAT deposition in numerous studies.37,47,63,71 Surprisingly, vigorous exercise did not appear to influence IntraMAT levels in members of our cohort that achieved that level of engagement. Only moderate exercise was shown to correlate with IntraMAT levels, and the correlation was the inverse of what was predicted. Individuals engaging in moderate exercise had a statistically significant increase in IntraMAT. Based on the literature, physical activity should have protected against IntraMAT infiltration, yet that was not the case in this cohort. One possible explanation could be that prior works often looked at older populations, which would be expected to exhibit higher baseline IntraMAT levels. Against that backdrop, the positive effects of physical activity might be more apparent.64,79
An alternative explanation is that participants, in this study, were generous when reporting their exercise engagement. A recent report comparing results from an objective wearable activity monitor (e.g., Fitbit) and a subjective activity survey revealed that participants underestimated their time spent sedentary and overestimated the frequency and intensity of their exercise sessions. 80 While providing activity monitors to participants would have given us more confidence in the exercise data, that was beyond the financial feasibility of this study.
The relationship between IntraMAT and LBP seen in some studies 9,34,81,82 presents a classic chicken and egg conundrum. Does IntraMAT cause LBP or does inactivity consequent to LBP cause an increase in IntraMAT? 83 Increased IntraMAT fractions achieved through manipulation of experimental animals adversely affects the function of neighboring muscle fibers, highlighting the detrimental effects of IntraMat. 19 Anatomic and functional imbalance in the paraspinal muscles has been correlated with LBP. 84 Lower back pain, in turn, is associated with activity avoidance, sedentary behaviors, and increased IntraMAT levels. 85 Thus, IntraMAT and LBP have the potential to create a deleterious feed-forward loop that may ultimately manifest in chronic LBP. It may be that the young cohort in this study had not been in the loop long enough for a correlation between LBP and IntraMAT to manifest.
Limitations
The main limitation to this study was the recruitment of participants by convenience and the pre-experimental research design. The threats to internal and external validity make these results unique to this set of participants.
Sonography is a relatively new diagnostic choice for IMAT analysis. More studies are needed to establish appropriate parameters for use and determine comparability to more established diagnostic imaging techniques, such as MRI and CT. While some findings in this study were consistent with results obtained using MRI in previous studies, there were also incongruent results. It is unclear whether this is due to the novelty of the study cohort or reflects limitations of sonography for IMAT analysis.
Preclinical medical students are an interesting cohort with unique attributes. However, this uniqueness may also limit the broad applicability of the study findings. This cohort comprises young adults who predominantly suffered from RLBP rather than CLBP. IntraMAT levels associated with LBP are likely to manifest with time and might be more obvious in an older population that had experienced longer duration LBP.
Only sonographic images from the participant’s right side were analyzed in this study. This decision was based on including different scan parameters (default and optimized) in the study and a desire to minimally inconvenience participants. Recent reports suggest that asymmetry of the paraspinal muscles may be associated with LBP. 86 Sonographic examinations in any future studies, of the paraspinal musculature, should be performed bilaterally and eliminate the manual image settings optimization step.
This study required that paraspinal musculature be traced by hand on each sonographic image, to produce histogram data output. Although the tracing was done methodically and carefully, there was still some subjectivity to defining muscular borders in regions that were not clearly visible in some of the sonograms.
Conclusion
It was generally expected that lumbar paraspinal muscles in individuals with LBP would have more IMAT accumulation, than their non-suffering peers. The study expectations were tempered by a recent report showing no association between IMAT levels and LBP when confounding variables of gender and BMI were considered. 49 Contrary to the study expectations, no relationship between increased IMAT and LBP was identified. One explanation may be that 81% of reported LBP in this cohort fell into the RLBP category (occurring less than 50% of the time), which showed no correlation with IMAT levels in a previous study. 9 The confounding issue of relative youth of the cohort when compared with other studies of IMAT and LBP may also have contributed to this negative result.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793241262763 – Supplemental material for Intramuscular Adipose Tissue in the Lumbar Paraspinal Muscles Does Not Correlate With Low Back Pain in Medical Students
Supplemental material, sj-docx-1-jdm-10.1177_87564793241262763 for Intramuscular Adipose Tissue in the Lumbar Paraspinal Muscles Does Not Correlate With Low Back Pain in Medical Students by Brian Gloyeske, Brock Bakewell, Dale Woodbury, Isain Zapata and Nena Lundgreen Mason in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793241262763 – Supplemental material for Intramuscular Adipose Tissue in the Lumbar Paraspinal Muscles Does Not Correlate With Low Back Pain in Medical Students
Supplemental material, sj-docx-2-jdm-10.1177_87564793241262763 for Intramuscular Adipose Tissue in the Lumbar Paraspinal Muscles Does Not Correlate With Low Back Pain in Medical Students by Brian Gloyeske, Brock Bakewell, Dale Woodbury, Isain Zapata and Nena Lundgreen Mason in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-pdf-3-jdm-10.1177_87564793241262763 – Supplemental material for Intramuscular Adipose Tissue in the Lumbar Paraspinal Muscles Does Not Correlate With Low Back Pain in Medical Students
Supplemental material, sj-pdf-3-jdm-10.1177_87564793241262763 for Intramuscular Adipose Tissue in the Lumbar Paraspinal Muscles Does Not Correlate With Low Back Pain in Medical Students by Brian Gloyeske, Brock Bakewell, Dale Woodbury, Isain Zapata and Nena Lundgreen Mason in Journal of Diagnostic Medical Sonography
Footnotes
Ethics Approval
Ethical approval for this study was obtained from Rocky Vista University’s Institutional Review Board (#2022-036).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.