
Abstract
Purpose:
This study aimed to develop a subjective categorization of nerve shape and to examine the relationship of shape categorizations to measurement of nerve circularity.
Methods:
Wrists were evaluated with sonography in healthy participants. Images of the median nerve were obtained in the transverse plane at the level of pisiform with the fingers resting, gripping, and pinching. Nerves were categorized as ovoid, angular, or irregular, and the cross-sectional area and perimeter were measured to calculate nerve circularity.
Results:
Across 167 participants, the median nerve shifted from being primarily ovoid at rest to angular shaped when the fingers were in a full fist or pinching. Approximately three-quarters of subjects exhibited a shape change during dynamic movement. Irregular nerves had the lowest circularity values; however, the majority of nerves had similar circularity measures despite having different shapes.
Conclusions:
Subjective categorization of shape has the potential to be a valid technique for evaluation of the median nerve using sonography, and this evaluation may provide additional information regarding nerve compression that is not fully captured by a circularity measure. Further investigation is needed to determine how these two techniques may be best used individually or together to advance clinical diagnosis, prevention, and rehabilitative interventions.
Carpal tunnel syndrome (CTS) is the most common nerve entrapment of the upper extremity caused by compression of the median nerve in the carpal tunnel.1,2 Approximately 3.8% of the general population has CTS, 3 and the economic costs of CTS are a heavy burden to society. 4 Most cases of CTS are considered idiopathic, 5 but several environmental risk factors are related to the condition, such as repetitive hand motions6–8 and prolonged postures in extremes of wrist flexion or extension. 4 One underlying pathophysiologic theory behind these risk factors is that during hand motion, the median nerve is deformed due to a combination of pressure and available space within the carpal tunnel.9,10 For some hand motions or positions, the median nerve is more distorted and more vulnerable to pressures in the carpal tunnel.
Recently, sonography has been used to evaluate the median nerve in the carpal tunnel due to its ability to capture nerve anatomy and other advantages such as accessibility, low cost, and noninvasiveness.7,11 Most studies have used sonography to identify morphologic features and changes of the median nerve with quantitative measurements. Common nerve measures include cross-sectional area (CSA) and flattening ratio, that is, medial-lateral diameter divided by anterior-posterior diameter.12–14 A less common measure more recently appearing in literature is median nerve circularity.15,16 Circularity is a measurement calculated using the CSA and perimeter of the median nerve (4π * CSA/perimeter 2 ), which indicates how close the median nerve’s shape is to a circle.15–17 Using circularity measurement, studies have shown that the median nerve is deformed during hand motions and during forced gripping—that is, when grip force increases, the median nerve becomes more flattened.10,15,18–20 Identifying nerves that are more flat than round may serve as an indicator of increased compression, which is a risk factor for development of nerve pathology.
However, the quantitative measurement of circularity has several limitations. Calculating circularity is a challenging procedure that requires reliable and valid measurements of the CSA and perimeter of the median nerve. This process takes practice and time to develop the necessary skills and expertise. Calculating circularity also raises the potential for errors, because it is not an automatic value. Rather, the calculation requires additional steps beyond the measures directly reported on the machine or other imaging software. In addition, current studies using circularity have conflicting results,10,15,18–20 such that median nerves with a similar circularity can exhibit different shapes, which may correlate with different amounts of compression. The median nerve could be compressed by surrounding tendons and structures becoming flattened or irregular in shape during hand movement or have a different circular or ovoid shape than when the hand is at rest due to varied compression by different surrounding tissues (e.g., slightly taller than longer vs. slightly longer than taller).
As such, it may be useful to further understand circularity by evaluating the amount of compression or variations in shape, thereby improving upon the use of circularity as a singular method for evaluating nerve pathology. Given the current limitations of circularity measurement and need for further refinement of our understanding of the applicability of the circularity measurement, we aimed to develop a subjective categorization of nerve shape and explore the usefulness of adding the proposed subjective categorization of nerve shape to existing protocols for measuring nerve circularity. This process can help to further a more nuanced understanding of nerve compression as it contributes to the identification of morphologic changes or individual morphologic patterns that are predictive of the onset of CTS in future research.
Methods
Participants
A total of 172 asymptomatic students were recruited from two universities between June 2015 and September 2018. Participants were excluded if they reported history of a carpal tunnel release surgery, median nerve pathology, or other polyneuropathy that involved the median nerve. Participants with bilateral bifid median nerves in the carpal tunnel were excluded. For participants with a unilateral bifid median nerve, the wrist with the bifid median nerve was excluded and the wrist with the nonbifid median nerve was included in the final analysis. Demographic data, including age, sex, ethnicity/race, and hand dominance, were obtained via self-report. The study was approved by the institutional review board, and written informed consent was signed by participants prior to participation in the study.
Sonographic Technique
Participants were seated facing the sonographer with the shoulder adducted, elbow comfortably extended, the forearm fully supinated and resting on the table, and the hand in a relaxed position. Imaging was conducted using a Logiq-e portable sonography machine (GE Healthcare, Milwaukee, WI) with a 12-MHz linear array transducer by two experienced musculoskeletal sonographers. The transducer was placed on top of the wrist with no additional force than the weight of the probe on the skin. Sonographic images were taken on both wrists by placing the transducer over the carpal tunnel at the level of pisiform in the transverse plane to obtain short-axis views of the median nerve.
Static images of the carpal tunnel and the median nerve were taken with the fingers in three positions: resting, gripping, and pinching. For resting, the fingers were held in a naturally relaxed position, which resulted in slight composite flexion throughout all digits. During gripping, the participant started with the fingers fully extended and slowly flexed the fingers into a closed fist without any forceful gripping or squeezing with the fingers. After holding the closed fist for a brief moment, the participant opened the hand to a fully extended position. To capture the median nerve during pinching, participants held a pen in their hand using a tripod or modified tripod pinch, as if they were to write. While the pinch position was not standardized across participants, the technique was intended to capture the functional position most often used by each individual participant. Static images were obtained in both the resting and pinching positions, with image optimization focused on the median nerve. Dynamic cine clips were recorded while the participant completed the gripping motion, each lasting approximately six seconds. The sonographer ensured that the transducer was maintained in a stable position over the wrist throughout the motion, using the pisiform as a bony landmark. Each image and cine clip were obtained at least twice to ensure that a high-quality, valid image was obtained for evaluation of the median nerve.
Image Analysis
Image processing
Images and cine clips were archived and analyzed using ViewPoint 6 (GE Healthcare). Prior to analysis, all images within a participant file were screened to determine if a bifid nerve was present, within the carpal tunnel. During this screening process, the resting and pinching images that most clearly depicted the median nerve were identified for analysis. Similarly, each cine clip of gripping motion was evaluated to select the clip that most clearly represented the median nerve throughout the movement of the fingers and was most stable as identified by the lack of shifting of bony landmarks (pisiform) within the frame. The rater then identified a frame at the start of the clip prior to initiation of movement and a frame in the middle of the cine clip where motion had paused, thus indicating the hand was in a full grip position. These frames were used along with the still images in the analysis of median nerve shape.
Nerve shape
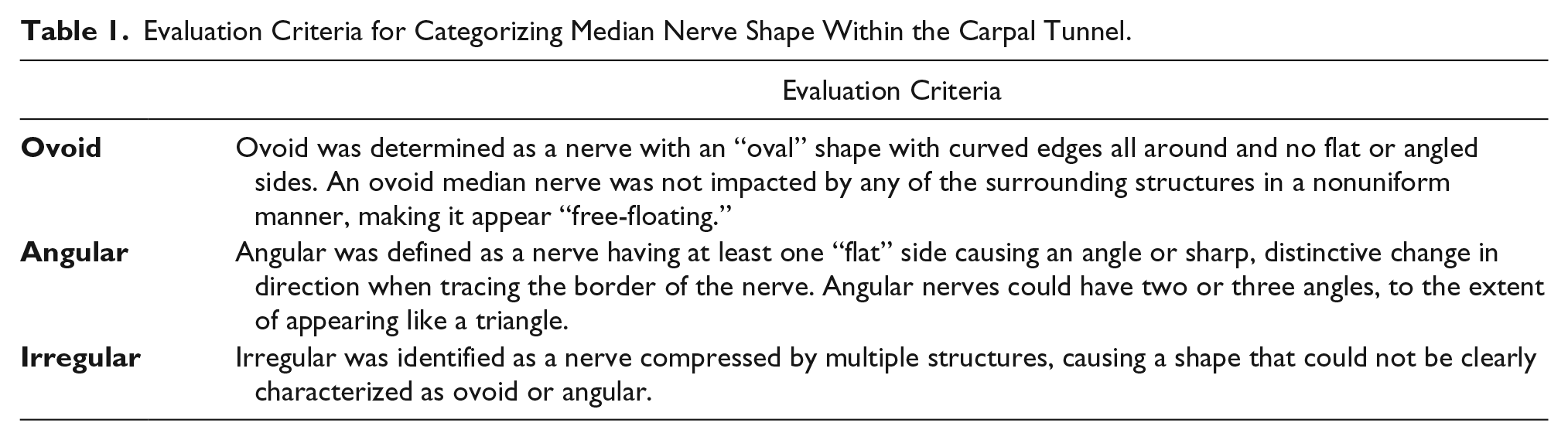
Through an iterative process of image review and discussion, the research team developed consensus on three categories of median nerve shape, which was followed by further iterations of image evaluation, review, and discussion to refine the evaluation criteria for categorizing nerve images. The research team consisted of a registered musculoskeletal sonographer and three students with limited previous sonography experience. As part of the criteria development process, three student raters analyzed nerve shapes in images obtained from the first 25 participants in the study across multiple rounds of 5 to 10 cases per round. In each round, we noted that a variety of shapes were represented within the images. Pairwise percent agreement between the three raters was calculated each time the raters completed analysis on a series of images. The evaluation criteria were refined through discussions with the sonographer until the research team agreed upon definitions that resulted in acceptable interrater reliability (i.e., >80%). The final evaluation criteria used to categorize nerves into ovoid, angular, or irregular shapes are detailed in Table 1, and examples of nerve with each shape are shown in Figure 1. Using these criteria and the images or still frames selected in the screening process, the shape of the median nerve, at the pisiform, was subjectively categorized for each wrist of every participant in the resting, gripping, and pinching position. All three trained raters evaluated images; only one rater categorized each image.
Evaluation Criteria for Categorizing Median Nerve Shape Within the Carpal Tunnel.
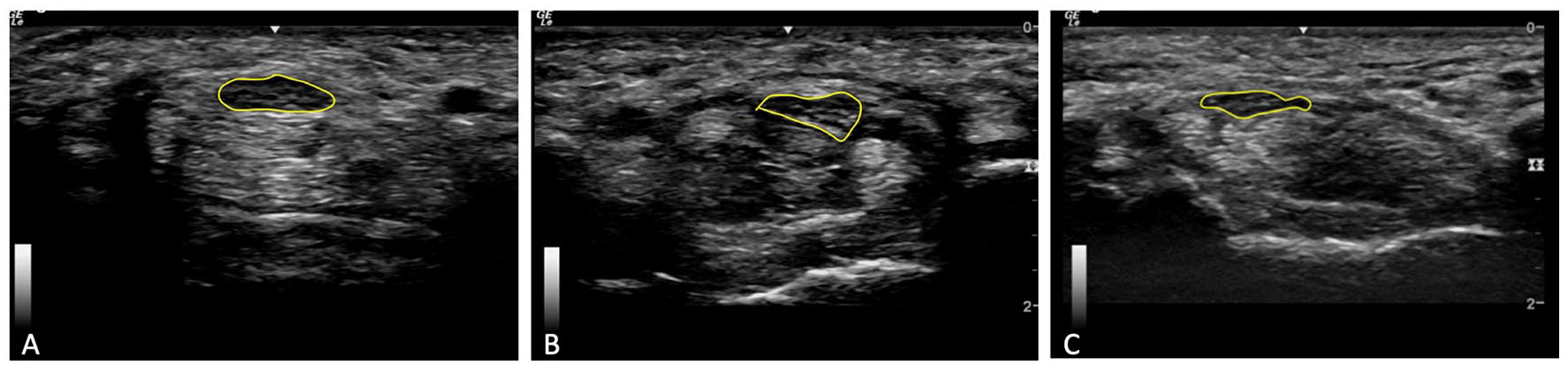
Gray-scale transverse images of the median nerve (yellow circle) at the level of the pisiform depicting three different categorizations of median nerve shape: (A) ovoid, (B) angular, and (C) irregular.
Shape change
In addition to identifying the shape of the median nerve in specific static positions, the cine clips were subjectively evaluated to determine if the shape of the median nerve changed at any point during the gripping motion. Any indication that the nerve was compressed or impacted by the surrounding tendons or other structures during the gripping motion was recorded as a “change.” This dynamic evaluation allowed for identification of nerve compression during functional movement, which may not have been apparent if the shape of the median nerve had been categorized as being the same using static images at the beginning and end of the gripping movement. If the nerve shape remained the same and was not visually impacted by the surrounding structures during the entire gripping movement, shape change was recorded as “no change.”
Nerve circularity
Nerve circularity was calculated using the CSA and perimeter of the median nerve measured on the static images of resting, gripping, and pinching. A direct trace along the inner hyperechoic border of the nerve was used to obtain CSA and the perimeter. 21 CSA and the perimeter of the nerve were measured three times, and the average of the three measurements was used to calculate circularity as follows 17 :

Statistical Analysis
Descriptive statistics were calculated for all demographic data. A chi-squared test was performed to examine if median nerve shape and shape change were associated with hand dominance. A Shapiro-Wilk test for normality was performed for median nerve CSA, perimeter, and circularity data, confirming that these data were normally distributed; as such, these data were expressed and evaluated as parametric data using mean ± standard deviation (SD). A two-sample independent t test was used to analyze the differences in the means of CSA, perimeter, and circularity between dominant and nondominant sides. An analysis of variance was performed to examine differences in mean values of CSA, perimeter, and circularity between rest, grip, and pinch positions, as well as between the three categorizations of nerve shapes. A post hoc Bonferroni test was performed to identify significant group differences. SPSS (version 24; SPSS, Inc., an IBM Company, Chicago, IL) was used for statistical analysis, and P values of <.05 were considered statistically significant.
Results
A total of 172 asymptomatic participants were enrolled in the study. Five participants had bilateral bifid median nerves, resulting in data from 167 participants for the final analysis. These participants were predominately right-handed (92.2%) females (85.0%) who had a mean age of 24.6 ± 3.3 years (Table 2). Across the sample, 11 participants had a unilateral bifid median nerve in the carpal tunnel on their dominant hand, and 10 participants had a unilateral bifid median nerve in the carpal tunnel on their nondominant hand. The analyses included data from 156 dominant wrists and 157 nondominant wrists.
Descriptive Statistics of Participants Enrolled in the Study (n = 167).
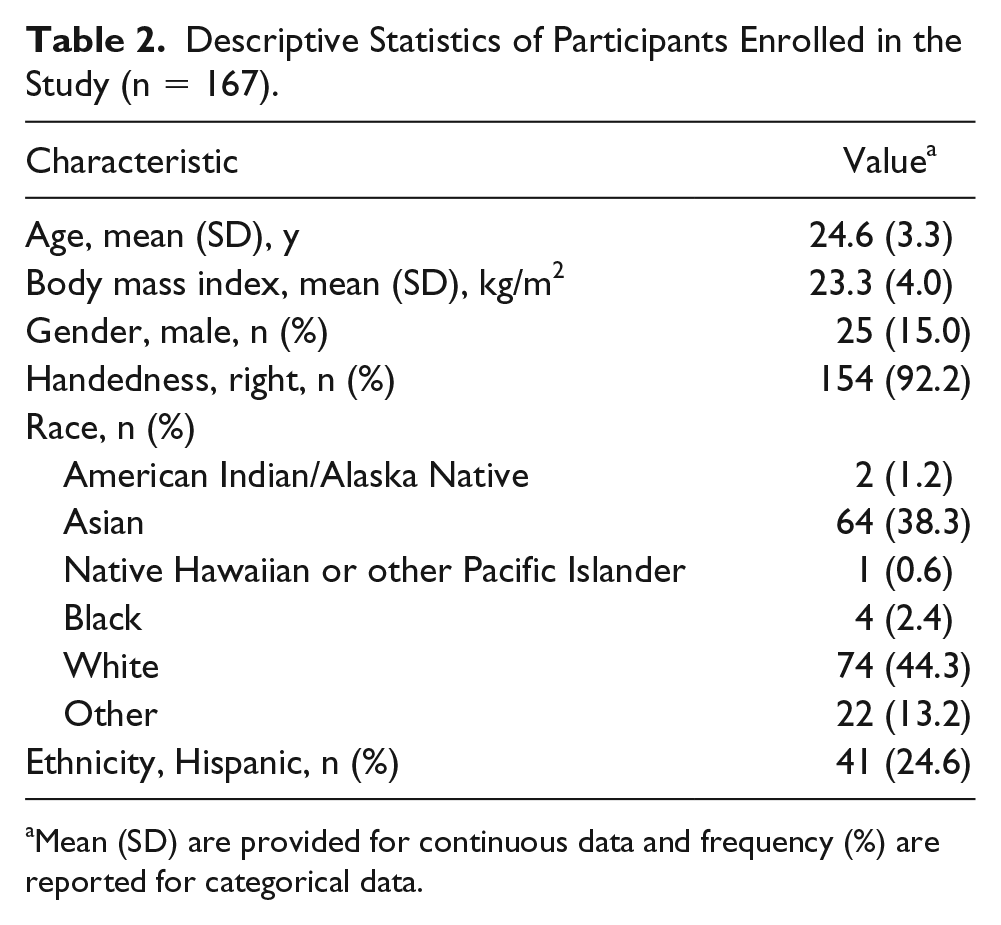
Mean (SD) are provided for continuous data and frequency (%) are reported for categorical data.
The frequency of the median nerve shapes across various finger positions in the static images and shape changes during dynamic gripping is reported in Table 3. When the hand is in the rest position, the largest number of the subjects exhibited an ovoid median nerve (48.7% and 38.2% for the dominant and nondominant side, respectively), with the nondominant hand having a higher proportion of irregularly shaped nerves with fewer ovoid nerves than the dominant hand (P < .01). In contrast, when gripping or pinching, the majority of participants had an angular shape of the median nerve in both the dominant and nondominant hands. Figure 2 depicts the distributions of median nerve shape across the three positions, highlighting a moderate shift in frequencies away from ovoid in resting to angular with grip and pinch. Despite moderate shifts in shapes between the start and end points of resting and gripping, approximately three-quarters of subjects exhibited a shape change at some point during the dynamic gripping movement (72.4% and 77.7% for the dominant and nondominant side, respectively).
Distribution of Median Nerve Shapes Across Finger Positions in Static Images and Shape Change During Dynamic Gripping Motion in the Dominant and Nondominant Sides.
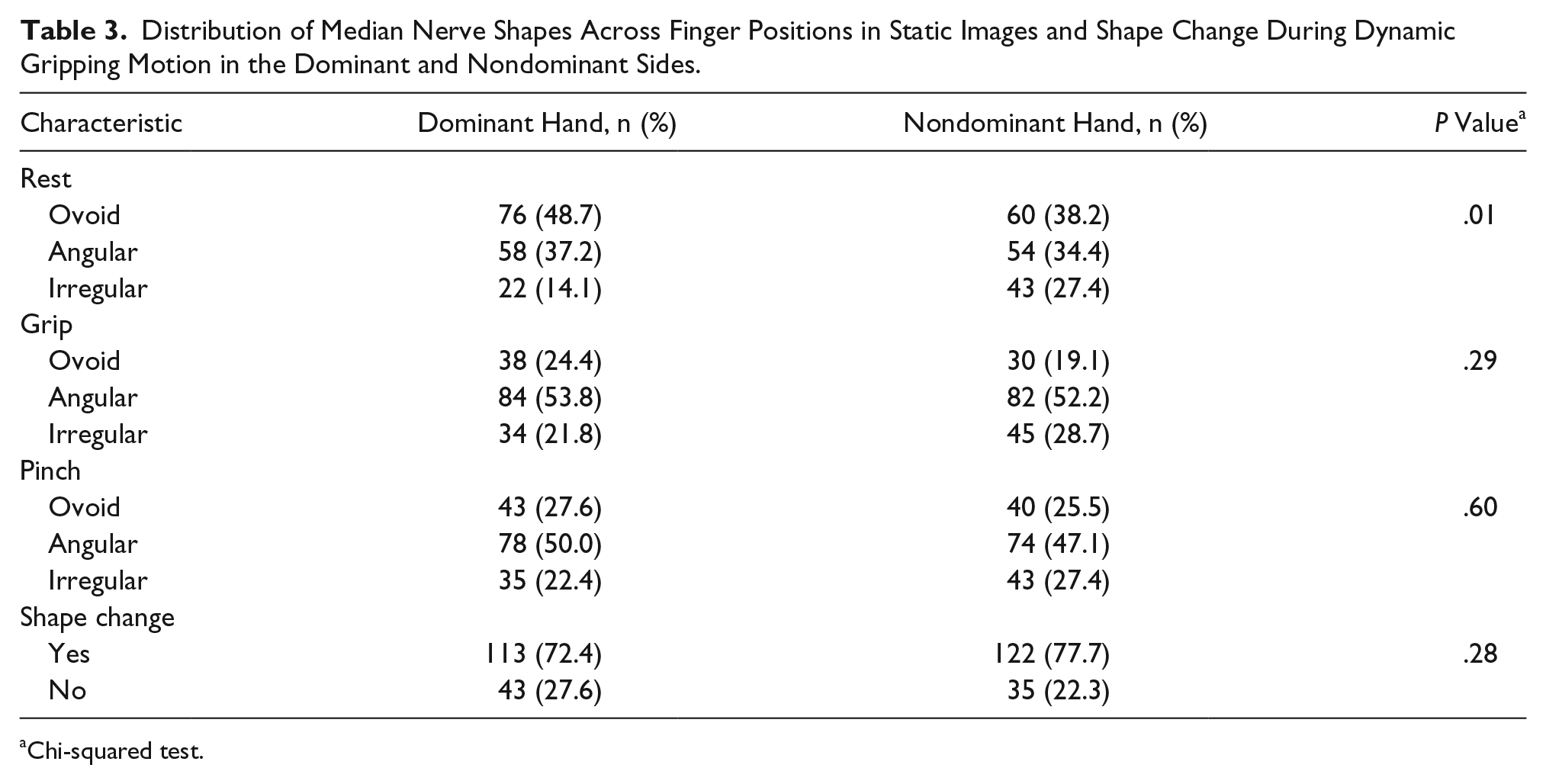
Chi-squared test.
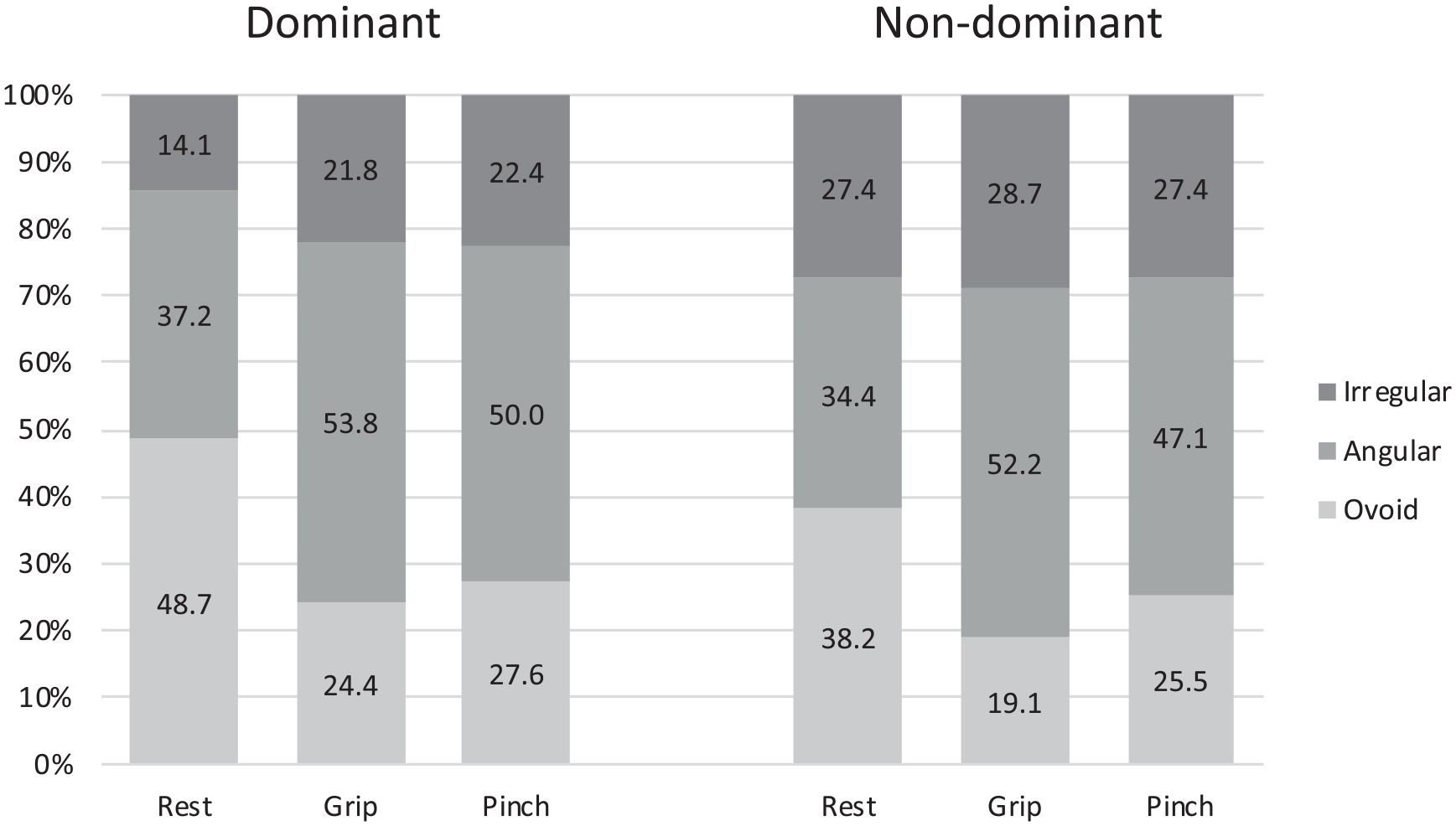
The distribution of median nerve shape during hand rest, grip, and pinch for dominant (n = 157) and nondominant (n = 156) wrists.
The mean and SD of median nerve CSA, perimeter, and circularity in resting, gripping, and pinching positions for the dominant and nondominant sides are shown in Table 4. The mean CSA of the median nerve of the dominant wrist was significantly greater than the nondominant wrist in gripping and pinching (P = .001 and P = .008, respectively), and the perimeter of the median nerve of the dominant wrist was significantly greater than the nondominant wrist in pinching (P = .013). There were no significant differences in average circularity measures of the nerve between the dominant and the nondominant sides or between resting, gripping, and pinching positions.
Comparison of Mean ± SD of Cross-Sectional Area (CSA), Perimeter, and Circularity of the Median Nerve by Finger Position Within the Dominant (n = 156) and Nondominant Sides (n = 157).
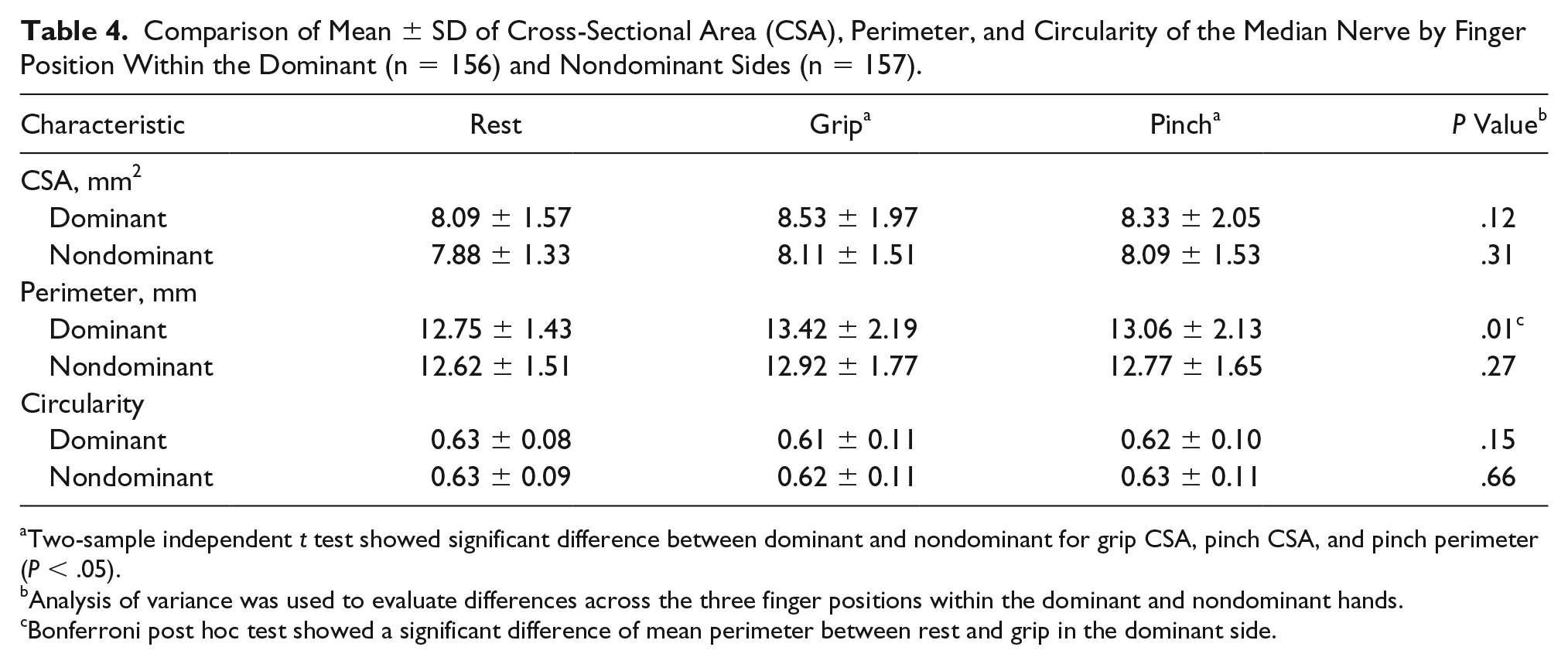
Two-sample independent t test showed significant difference between dominant and nondominant for grip CSA, pinch CSA, and pinch perimeter (P < .05).
Analysis of variance was used to evaluate differences across the three finger positions within the dominant and nondominant hands.
Bonferroni post hoc test showed a significant difference of mean perimeter between rest and grip in the dominant side.
Finally, the examination of differences in average CSA, perimeter, and circularity by nerve shape is presented in Figure 3. CSA measures were not found to be different among nerves of different shapes. In the dominant wrist, the average perimeter (14.14 mm) was significantly larger and circularity (0.55) was significantly smaller for median nerves with irregular shapes as compared to the same measures in nerves with an angular shape (12.85 mm, P < .001; 0.62, P < .001 respectively) and ovoid shape (12.77 mm, P < .001; 0.65, P < .001, respectively). These differences were also noted on the nondominant side in similar magnitudes (P < .001), with an additional significant difference in the circularity between ovoid (0.67) and angular (0.58) nerves (P = .007). While the average circularity calculations across the three shape categories were significantly different, the range of values overlapped across the categories. The ranges from 10th to 90th percentile for median nerve with the shape of ovoid, angular, and irregular were 0.54 to 0.79, 0.51 to 0.76, and 0.45 to 0.69, respectively; 80.6% of all the median nerves had a circularity between 0.45 and 0.75 and were distributed across all three shape categories. Given these overlaps, these statistical differences in circularity may not be clinically meaningful. For example, as demonstrated in Figure 4, three median nerves each having a circularity of approximately 0.63 belong to three different shape categories due to differences in compression.
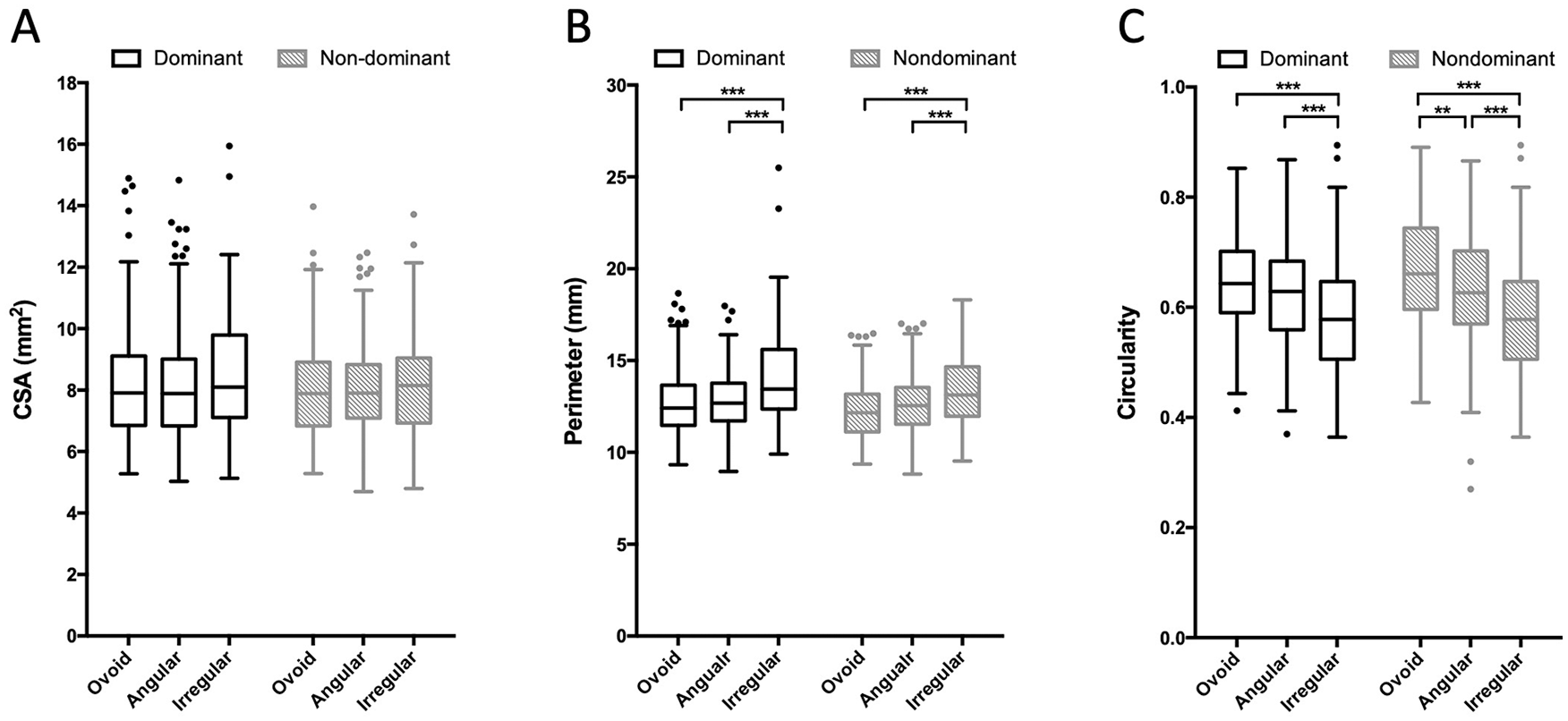
Comparison of average cross-sectional area (CSA, A), perimeter (B), and circularity (C) among ovoid, angular, and irregular median nerves by hand dominance. Results of analysis of variance testing, with Bonferroni post hoc testing for pairwise comparisons indicating significant differences: **P < .01, ***P < .001.
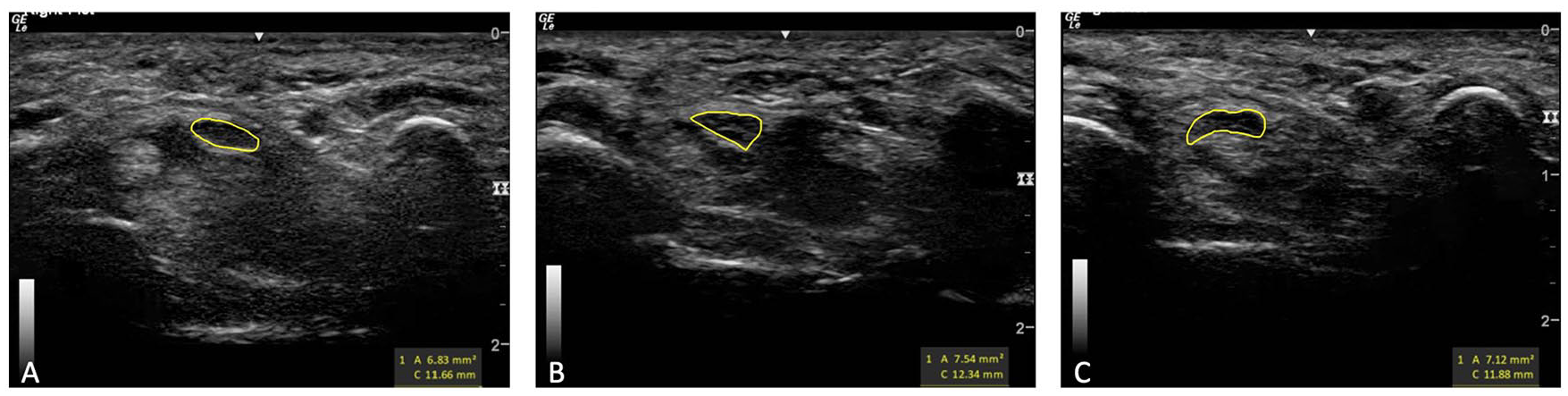
Gray-scale transverse images taken at the level of pisiform within the carpal tunnel for measurement of the median nerve (yellow circle) shape and circularity, demonstrating three median nerves with similar circularity but different shapes due to varying amounts of compression by surrounding structures. (A) Ovoid median nerve with a circularity of 0.63. (B) Angular median nerve with a circularity of 0.62. (C) Irregular median nerve with a circularity of 0.63.
Discussion
The purpose of this study was to develop a subjective categorization of median nerve shape representative of the amount of compression on the nerve and explore the usefulness of adding the proposed subjective categorization of nerve shape to the emerging measure of nerve circularity. We developed evaluation criteria for categorizing nerve shape into three categories, including ovoid, angular, and irregular. The median nerve was primarily found to be ovoid when the fingers were in a relaxed position, with the majority of nerves having an angular shape when the fingers were moved into a full fist or pinching to hold a pen for writing. While we explored the usefulness of these shape categorizations for concurrent measures of circularity, we found that subjective categorization provided additional information related to nerve compression. As sonography is being increasingly used to identify risk factors contributing to median nerve injury 15 and for diagnosis of carpal tunnel syndrome,22,23 these findings may be useful for advancing both research and practice.
Circularity is a quantitative method to identify the roundness of an object in a 2D plane. Circularly was first suggested in 1927 by Cox, 17 who measured the roundedness of sand grains using the formula noted in the methods section above. This concept has been translated into health care as a means for detecting deformation of the median nerve, with multiple studies using this formula.10,15,16,24 Others have used a reciprocal version of this formula whereby the perimeter value is placed in the numerator and the area value is placed in the denominator.18,19 In both methods, a value of 1.0 suggests a perfect circle; however, in the original method, lower values indicate a less circular object as opposed to higher values over 1.0 when using the reciprocal method. While both techniques provide an accurate measure of circularity because the same data inputs are used, the original formula may be easier to interpret and therefore should be used across the field to promote data comparison and eliminate confusion across studies.
Regardless of the method used, there is mixed evidence for the correlation between measures of median nerve circularity and finger positions. Cowley and colleagues 15 noted a slight, nonsignificant decrease in median nerve circularity from 0.57 to 0.54 when the hand was in a neutral position versus a pinching position. Using the reciprocal formula, Yoshii and colleagues 19 found a nonsignificant change in nerve circularity that increased from 1.69 to 1.75 when measured in full finger extension to full finger flexion. This equates to a decrease in circularity from 0.59 to 0.57, when using normal circularity. Also using the reciprocal formula, Van Doesburg and colleagues 18 reported a decrease in circularity that equates to a 0.03 change (from 0.58 to 0.55) with finger movement. In contrast to these studies that may suggest that a nerve becomes less round with finger flexion, a fourth study 10 noted that median nerve circularity improved when moving from finger extension to finger flexion (i.e., 0.52 to 0.55 using the original formula).
Results in the current study showed slightly higher circularity but were similar to the first two studies noted above,15,19 in that the current study did not demonstrate any significant difference in nerve circularity measures between resting, gripping, and pinching. However, irrespective of the position of the fingers, we were able to validate that circularity of the median nerve significantly decreased when the nerve was identified as ovoid shape versus angular or irregular. This was especially true for nerves, with high circularity values (>0.75) being primarily ovoid and angular and low circularity values (<0.45) being primarily irregular in shape. However, given that the majority of nerves had midrange circularity values (0.45–0.75) that were distributed across all shape categories, circularity may be limited in providing clinically relevant information when values fall within this range. Instead, the subjective categorization may be better at identifying nerve compression for these individuals than would be a circularity calculation alone.
As with providing additional information to circularity, subjective evaluation has other benefits in the examination of median nerve compression. Specifically, subjective assessment of dynamic cine clips identified that functional hand use such as gripping or pinching led to intermittent compression on the median nerve in approximately three-fourths of individuals. Moreover, the subject categorization identified a significant shift in the distribution of ovoid-shaped nerves to angular- or irregular-shaped nerves when moving from resting to gripping or pinching. These findings are consistent with theories and literature that suggest the median nerve becomes compressed during finger movement.15,25 Thus, subjective categorization has an advantage over circularity in that it can be evaluated dynamically rather than being limited to static images.
Both circularity and evaluation of shape or shape change may be useful in advancing research and practice for prevention and intervention for median nerve injury. It is important to further examine how each of these measures supports the identification of nerve compression, to build upon the findings in our data. While a circularity calculation may be most useful when the values are higher or lower, a subjective examination of the nerve may be more important to identify either intermittent compression during dynamic activity or sustained compression due to finger positioning that results in change in shape. Employing these two techniques together further elucidate nuances of nerve compression that could be useful in research and practice. Future research should consider these measurement techniques individually and together to identify utility within clinical diagnosis and intervention, such that individualized care recommendations or splinting may be provided to assist a patient with CTS in minimizing movements that lead to compression. Alternatively, longitudinal studies could examine these measures to determine their ability to identify individuals at high risk for development of median nerve pathologies, such as CTS, due to median nerve deformation during functional hand use.
Limitations
This study has several limitations. Interpretation and use of these study findings are primarily limited by having evaluated the measures in only healthy participants. As such, the authors are unsure how these measures would apply to individuals with median nerve pathologies who may have enlarged median nerves, edema, or other pathologic considerations. Despite not being able to interpret these findings in clinical care, the results of this study showed potential usefulness of this subjective categorization for median nerve shape. Translation of this work to determine the value of the shape categorization in differentiating high-risk populations from the healthy population is important. Future studies could also explore this shape categorization as a support to the diagnosis or treatment of individuals with CTS.
Conclusion
In this study, with a high-resolution sonographic image, the shape of the median nerve in the carpal tunnel could be easily distinguished as ovoid, angular, or irregular by tracing inside the hypoechoic border of the median nerve. Irregular shapes demonstrated the least amount of circularity as compared to ovoid shapes. However, subjective evaluation of shape was more sensitive than circularity for identifying differences in nerve shape in static images obtained in various finger positions. Shape change was highly prevalent in all individuals during movements, and more angular- and irregular-shaped nerves were identified during functional positioning of the fingers than when at rest; differences that circularity did not identify. These data suggest that a subjective evaluation may have additional value beyond what circularity may provide in the assessment of nerve compression for prevention, diagnosis, and intervention as a component of research and practice.
Footnotes
Acknowledgements
We thank Jennifer Mitchell for her help in image acquisition and identification and Ariana Cristino for her initial contributions in development of a preliminary image analysis protocol that led to the final protocol deployed in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Undergraduate Research Associate Program at the University of Southern California and the Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health (grant R01-OH010665). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.