
Abstract
Objective:
Musculoskeletal (MSK) conditions pose significant challenges for both patients and healthcare providers. Diagnostic Medical Sonography (DMS) is a cost-effective, user-friendly, and real-time diagnostic tool capable of accurately assessing soft tissue pathology. Additionally, ultrasonography-guided injections (USGI) are recognized as a treatment that may offer precise, safe, and effective pain relief. The aim of this study was to explore patient experiences receiving a USGI given by an advanced physical therapy practitioner (APP).
Materials and Methods:
A sample of seven participants who received a USGI, given by an APP, were recruited from a private healthcare setting. In-depth, face-to-face and semistructured interviews were conducted with the participants. The data was transcribed verbatim and analyzed using an inductive qualitative content analysis (QCA) approach.
Results:
The data analysis identified three main categories and nine corresponding subcategories. These participants favored USGI for its precision, effectiveness, and reduced reliance on oral pain medication. Most of the participants perceived USGI as safe, as well as unguided injections. In this cohort, DMS had several added benefits, such as precise diagnostics, valuable insights into disease progression, enhanced patient confidence, and improved injection success rates. The patient-clinician relationship played a pivotal role, with the ability to choose a clinician and clear outcome discussions being crucial to these participants.
Conclusion:
This qualitative study revealed essential factors that may play a part in the USGI process. This work would suggest USGI, as the preferred choice for rapid pain relief, for this participant group. However, maintaining high patient satisfaction hinges on skilful management of patient expectations by a communicative clinician. This deeper understanding of the perception of USGI highlights the important role of the clinician performing USGI and offers suggestions for an improved patient experience.
Musculoskeletal pain (MSK) is routinely managed using a combination of physical therapy and rehabilitation exercises. In situations where pain persists or is limiting the patient’s ability to participate in rehabilitation, then injection therapy can be utilized to control their pain. In the United Kingdom, injection therapy is within the scope of practice for both medical and non-medical healthcare professionals, including physical therapists.
Recent expansion and upskilling of healthcare practitioners within the United Kingdom has led to the development of advanced physical therapy practitioners (APP). Existing evidence has consistently affirmed the safety and effectiveness of APPs in delivering improved patient outcomes and access to care. 1 Moreover, this can be achieved without the financial implications associated with referring patients to external orthopedic providers. 2
The role of an APP is described by the UK Chartered Society of Physiotherapy as those experienced physical therapists who are working in advanced job roles, triaging patients, and reducing patient waiting times for orthopedics and rheumatology. 3 APPs are eligible to complete additional post-graduate training, such as MSK diagnostic medical sonography (DMS), the prescription of medication, and injection therapy. 3 With this combination of enhanced skills, an APP can complete interventional procedures, such as injection therapy, under DMS guidance, a technique referred to as ultrasonography-guided injections (USGI). To ensure safety, it is imperative that the APP’s intended scope of practice is clearly defined and relevant and that post-graduate qualifications and work experience are maintained.4,5
Diagnostic medical sonography has the ability to assess the presence and severity of soft tissue pathology. 6 Research has revealed DMS to be on par with magnetic resonance imaging (MRI) in detecting and diagnosing rotator cuff tendon pathologies of the shoulder, and it is considered a diagnostic gold standard for assessing tendon structure. 7 The use of DMS has the unique capability of providing real-time, dynamic images and can reveal tissue structures, while the patient demonstrates their aggravating movements. Furthermore, the use of MSK DMS is both time and cost-effective when compared to MRI examinations. 8
Interventional sonography allows for a more precise placement of a needle. 9 Research has indicated that USGIs are significantly more accurate than landmark-guided injections, based on studies that reported 80-100% accuracy for knee joint and biceps sheath injections, compared to landmarked techniques.10,11 Importantly, injection therapy is considered safe, with significant side effects rarely occurring.12,13
It is a fundamental principle that patients should be at the forefront of high-quality healthcare.14,15 The Department of Health, England, has proposed three pillars for quality healthcare: patient safety, clinical effectiveness, and patient experience. 16 A recent systematic review of 55 studies underscored the importance of patient experience and its direct links to clinical effectiveness and safety. 17 While DMS and USGI have been reported to be safe and clinically effective, when completed by an APP, there is a lack of evidence regarding patient experiences. Therefore, the aim of this study was to explore patient experiences receiving a USGI given by an APP.
Materials and Methods
This was conceived as qualitative research that used qualitative description (QD), as a specific methodology. Qualitative description is an appropriate methodology for researchers conducting small studies, with the aim of gaining a deeper understanding of a participant’s experience, especially when little previous information is available. 18 Qualitative description is a form of naturalistic inquiry which can provide rich, accurate, and comprehensive findings pertaining to person’s lived experience. 19 This is achieved by using a low inference analytical approach; staying close to the original data and using language drawn directly from the study participants ensures minimal interpretation. 20 Findings drawn from QD can produce information that states facts in a clear, accessible, and readily accepted format for the reader.21 –23 The objective of QD is to obtain a better understanding of a participant’s experiences, based on a phenomenon, from that participant’s viewpoint. 19 Because the objective of this small study was to identify the experiences of patients who have undertaken a USGI, provided by an APP, utilizing a QD methodology seemed appropriate.
The consolidated criteria for reporting qualitative research checklist was used to ensure that all necessary components of this study were reported. 24 Ethical approval was granted by the University of Hertfordshire’s ethics board on 12/12/2022 (HSK/PGT/UH/04283).
Participant Recruitment and Data Collection
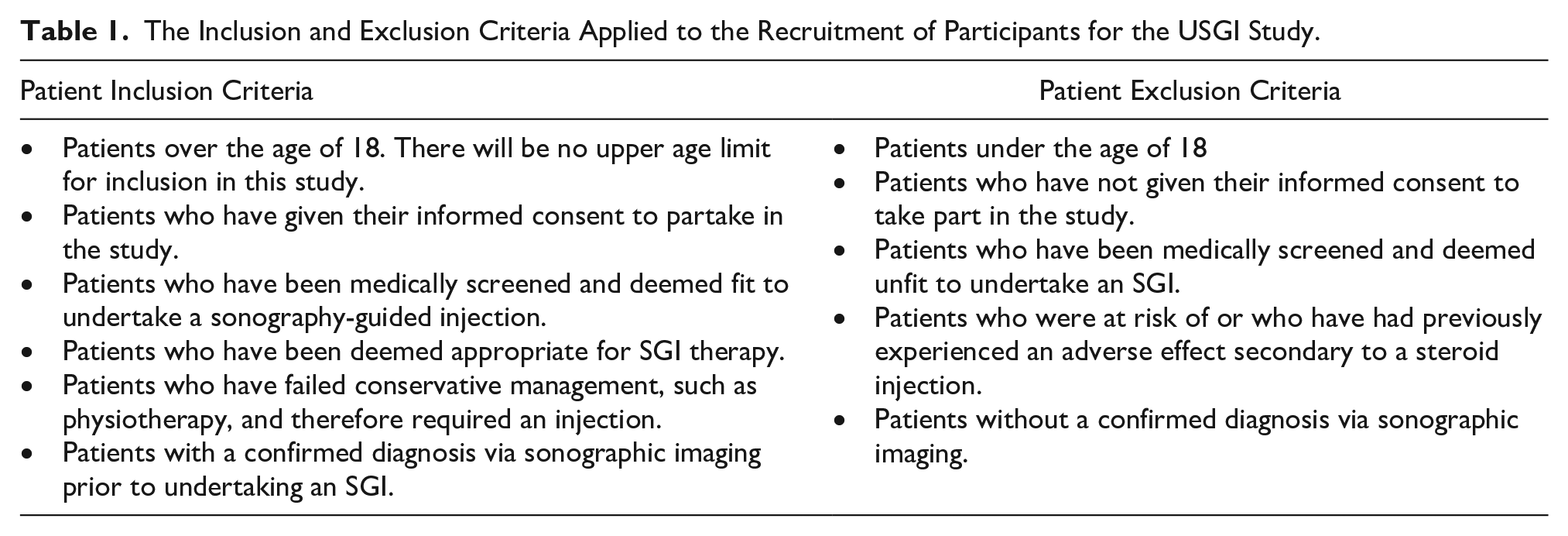
Purposive sampling, which is a non-randomized sampling method, was used in this study. This type of participant sample is made based on specific characteristics and then asked to answer specific research questions.18,22,25,26 In this study, the patient inclusion and exclusion criteria are provided (see Table 1).
The Inclusion and Exclusion Criteria Applied to the Recruitment of Participants for the USGI Study.
To mitigate bias, the principal investigator collaborated with two clinical experts (CM and DB) from a private USGI clinic and recruitment of participants was based on having been treated by these same clinicians, in an outpatient setting. 27 Prospective participants were sent an introductory e-mail outlining the study’s details, and further information was provided to those participants who expressed interest in joining the study. All participants signed a written consent of participation prior to being interviewed.
Participants were interviewed within 3 months following their USGI procedure due to the typical duration of corticosteroid effectiveness. 28 Data were collected through semistructured interviews. The semistructured interviews allowed for a gathering of information regarding personal experiences, attitudes, perceptions and beliefs related to their experiences. 29 The flexibility of a semistructured interview enabled the investigator to conduct the interview within the parameters of the research question, as well as giving participants the freedom to express their opinions. 30 The data collection process is provided in Figure 1.
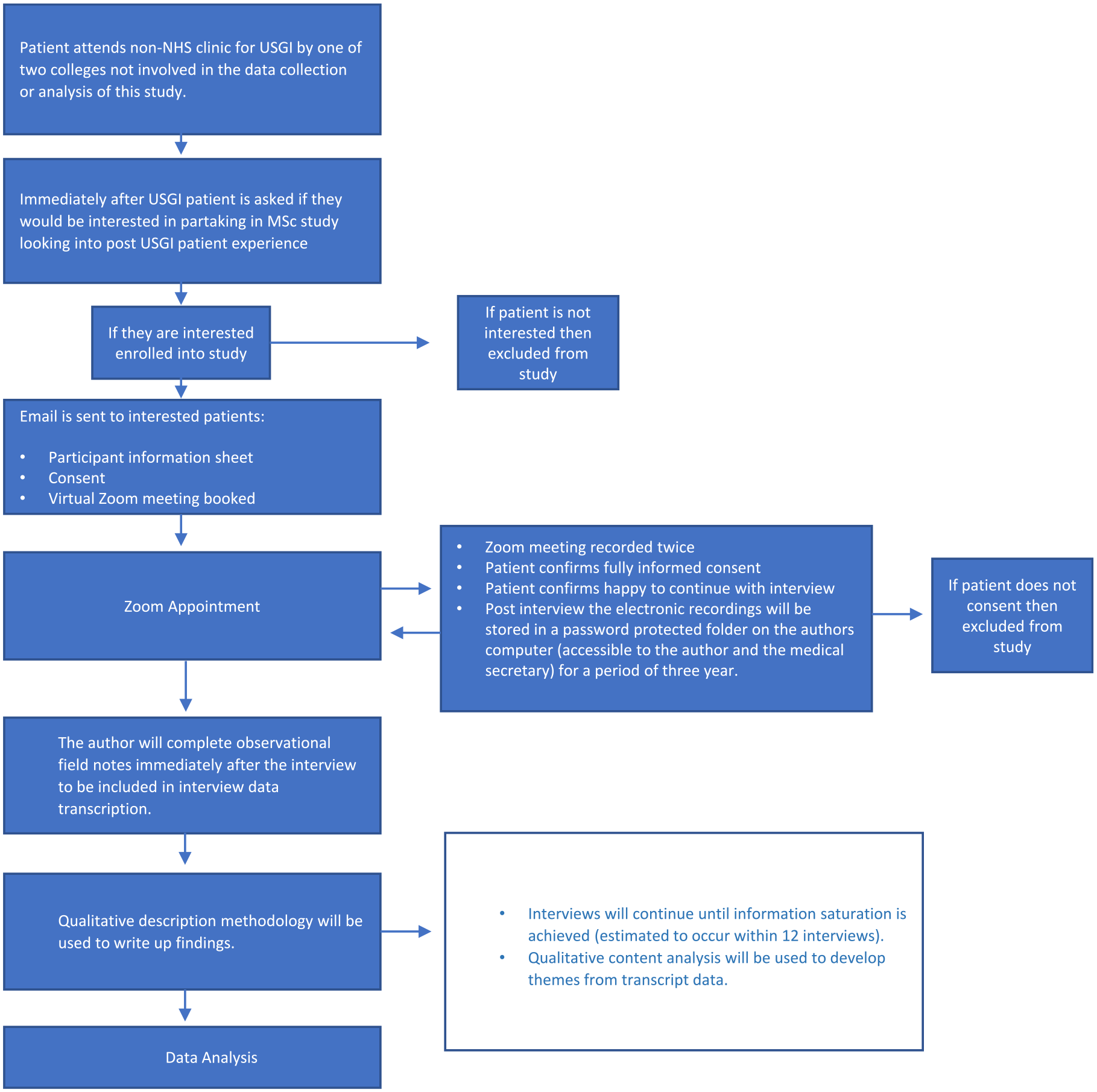
The data collection process utilized for the USGI study.
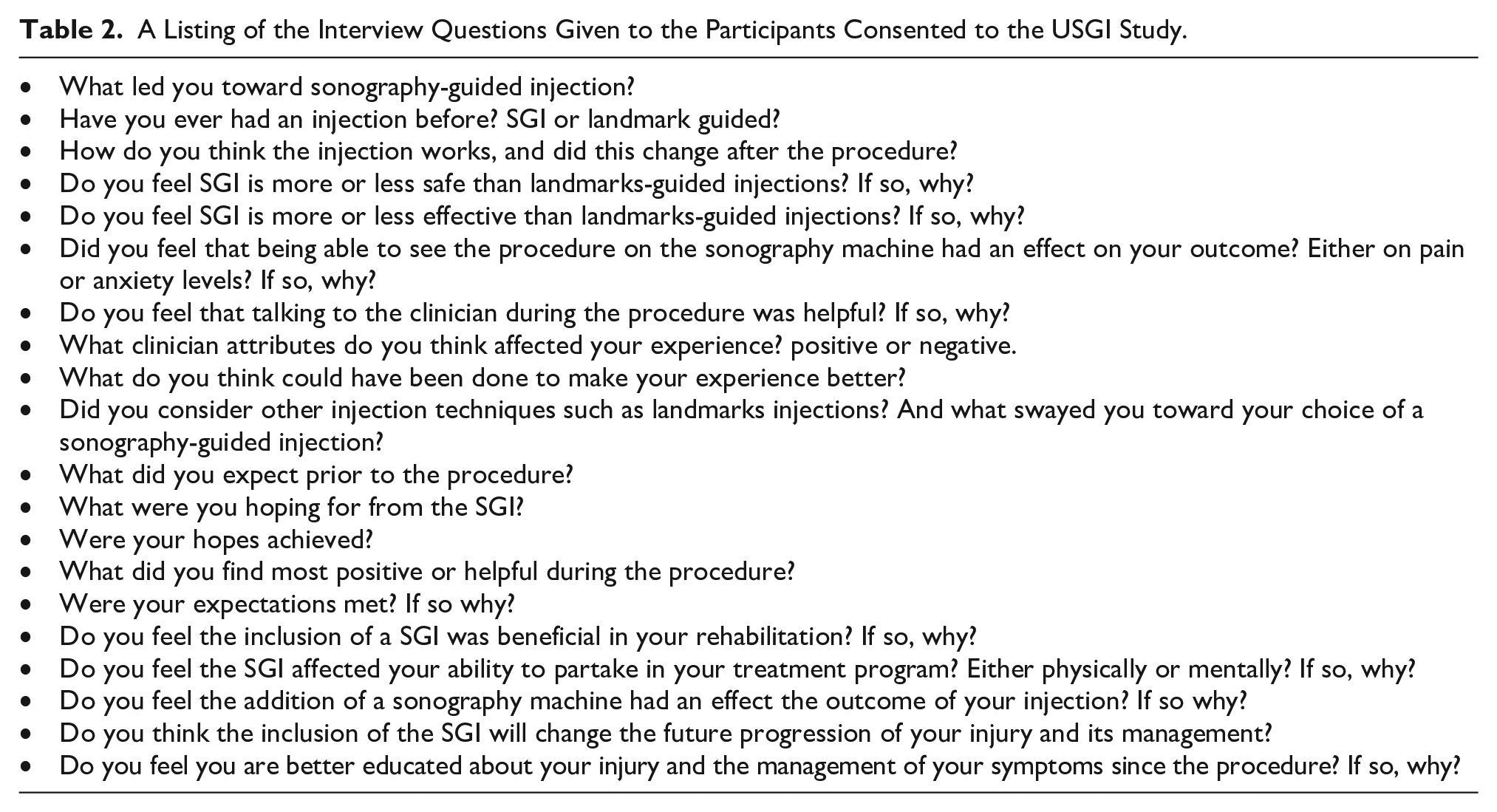
Given the limited evidence on patient’s experiences with USGI, open-ended interview questions were uniquely developed in collaboration with two expert physical therapy clinicians (CM and DB), who had 35 years of combined experience in providing UGSI. The specific interview questions are provided in Table 2.
A Listing of the Interview Questions Given to the Participants Consented to the USGI Study.
Because of concerns with face-to-face interviews being conducted during the COVID-19 pandemic, participant sessions were provided via Zoom. All Zoom sessions were recorded, and the interviews were transcribed verbatim by a transcriptionist. To enhance credibility, a post-interview reflective journal captured non-verbal cues, researcher impressions, and interview adjustments that helped to enrich the data collection.29,31 Reflexivity was achieved through continual self-reflection, maintenance of the journal, and acknowledgment of the researcher’s positioning as, a white, middle-aged, male physical therapist. To maintain an audit trail and ensure trustworthiness, detailed notes, researcher observations, and interview transcripts were meticulously documented, working closely with academic supervisor to review interview questions.32,33 A period of familiarization was undertaken where the raw data was analyzed prior to the development of analytical categories.
Data Analysis
This study and QD approach employed a reductive analysis method of qualitative comparative analysis (QCA).18,21,22 The analysis of the interview data involved three phases of QCA. Each interview transcript was considered as a unit of meaning, and repeated readings helped capture underlying sentiments. A comprehensive coding strategy was employed, with open coding identifying common words and terms. The coding process resulted in three primary analytical categories. These categories were refined, which resulted in the development of nine subcategories. The coinvestigator (RG) reviewed interview transcripts and cross-referenced them with the developed codes to enhance credibility.
Results
The principal investigator completed seven semistructured interviews, at which point data saturation was achieved, and no further interviews were conducted. From the data analysis, three primary analytical categories were identified. (1) USGI as an effective treatment procedure. (2) Patient education. (3) Private vs. National Health Service (NHS). These three primary categories were refined, which resulted in the development of nine subcategories (see Figure 2).
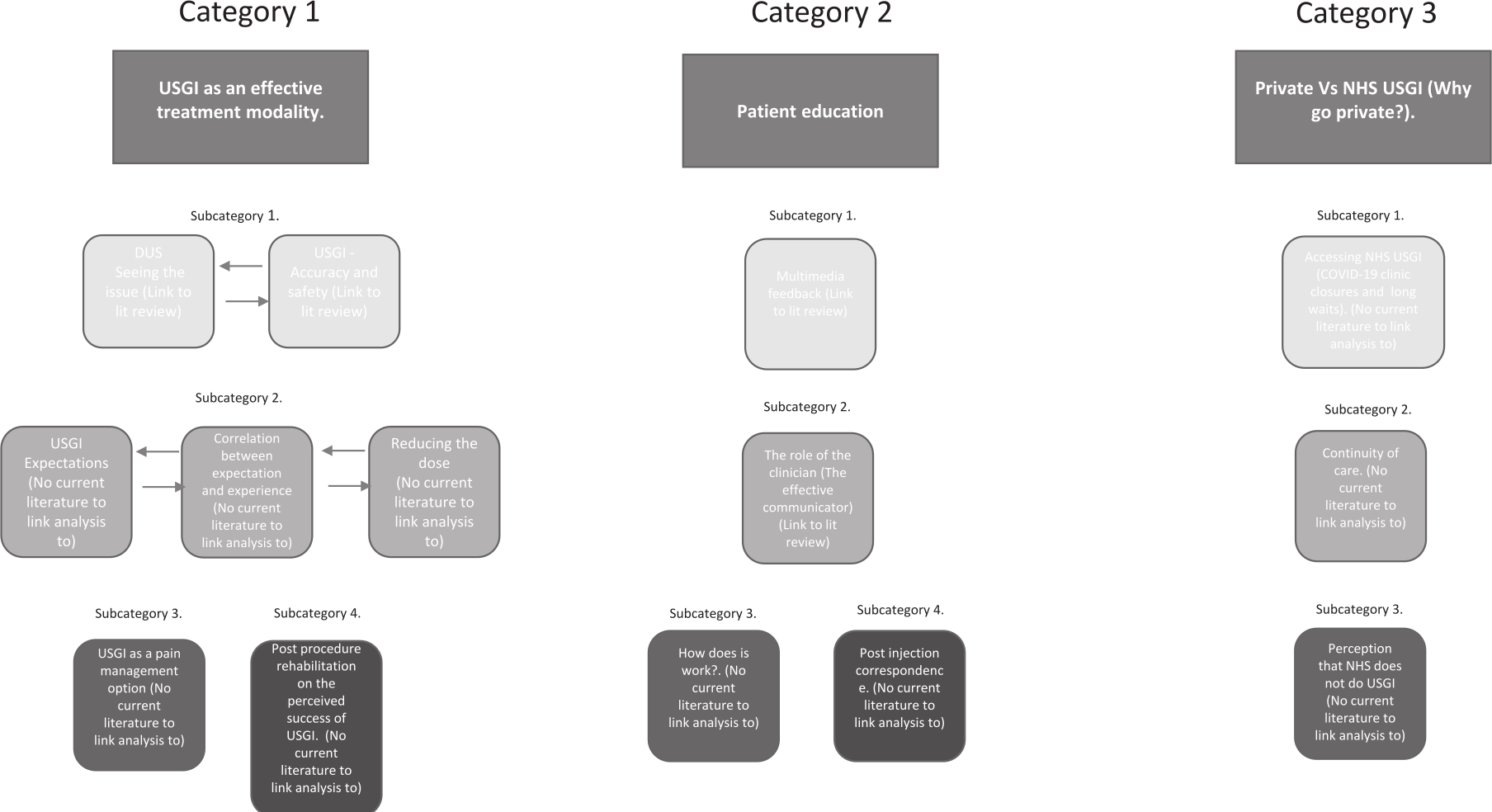
The qualitative scheme for data analysis and category development.
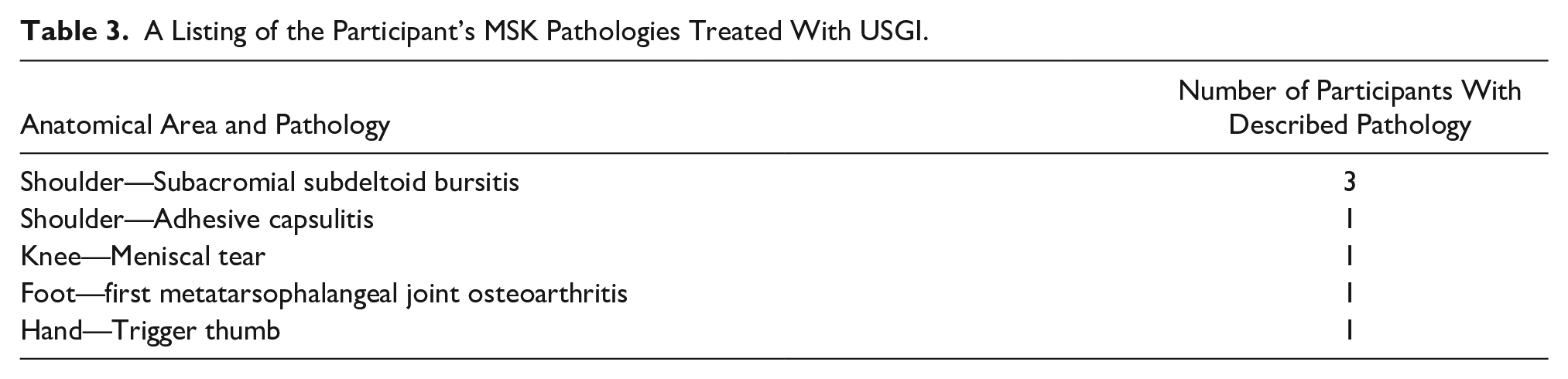
Participants were recruited solely from the private sector as the principal investigator worked within a single private clinic and not within a NHS setting. Participants ages ranged from 40 to 65 years (mean 52 years). Six participants were men, and one was a woman. All participants underwent USGI to alleviate MSK pain (see Table 3) and were interviewed within 3 months post-procedure. These demographics aligned with a typical patient profile that might undergo USGI, at the private clinic that serves these types of patients.
A Listing of the Participant’s MSK Pathologies Treated With USGI.
Category 1: USGI As an Effective Treatment Modality
This analytical category dealt with the procedural aspects and perceived effectiveness of USGI. It encompassed patient experiences of both DMS and USGI, along with exploring connections between preconceived notions, expectations, and actual patient experience.
The first subcategory highlighted the increased ability of DMS to accurately diagnose MSK pathology, with four participants believing DMS significantly enhanced their experience. Increased diagnostic confidence and diagnostic accuracy were both reported and considered as important attributes. Here is a participant example: “You could see unequivocally this structure had the issue and there’s something we can do about that.”
All participants agreed that USGI was highly effective for them, and they believed this was due to the increased accuracy. Here is a participant example:
“I really liked the guided one. I think it’s great, it’s using technology appropriately. I find it intriguing to see the actual area that the needle is going into. It’s going exactly where it should do in terms of if it’s going to have any effect it’s more likely to have a positive outcome.”
The perception that USGI could provide a specific, targeted treatment was associated with increased confidence in both the clinician and the procedure. Here is another participant’s response:
“Sonography gives the clinician the opportunity to give the exact dose in exactly the correct place. Gives me the confidence that the clinician is actually digging around to find the best place to inject. Without guidance you wouldn’t have a chance in hell, it would be potluck.”
There were differing views relating to the increased procedural safety compared to non-guided injections. An example of differing participant opinions is provided: “I don’t think there would be much difference in terms of safety.” (P#4) “More safe. You can see exactly where the inflammation is and exactly where the stock (medication) needs to go so you can use less of it.” (P#7)
Concerns regarding dependence on oral painkillers were a notable reason for seeking USGI. Several participants expressed a desire to minimize their reliance on medication, which was a key driver behind their decision to opt for a USGI. Interestingly, two participants expressed that the heightened precision offered by USGI led to a decreased necessity for oral painkillers. They saw USGI as an effective means of reducing their reliance on oral medication. Here is a participant’s response:
“I don’t want to be taking really strong painkillers that have a knock-on effect on your body. I wouldn’t even go down the painkiller road now. I would definitely go USGI. It allowed me to carry on living without constantly being on painkillers.”
When participants were asked about the influence of observing the USGI procedure on outcomes, three out of seven were unable to watch the injection process, primarily due to fear and anxiety. In contrast, two participants described how watching the procedure had a positive effect. It helped alleviate their anxiety and bolstered their confidence in the procedure. One participant stated, “Psychologically it helps.”
The second sub-category related to the correlation between expectation and clinician experience. The ability to select a clinician based on personal recommendations or reputation was considered highly desirable and was perceived as only attainable in a private healthcare setting. An example participant response is as follows:
“It’s always good to talk to an expert. He was recommended so it gave me confidence that he would be brilliant at giving the injection, something I couldn’t do via the NHS. It gave me confidence I was doing the right thing. A good recommendation that does it privately at a good price, why not get it done instantly.”
All participants expected the clinician to be able to perform the USGI confidently and in a calm and professional manner. One participant stated, “That the clinician is confident and that they could do it calmly and effectively—that’s exactly what happened.” Six participants expressed the expectation that USGI would lead to a swift decrease in pain and an improvement in mobility. In contrast, one participant anticipated short-term relief. Participant example statements were as follows: “After two or three days I’d have at least three months of pain free existence.” “Good short-medium term fix.”
Ultrasonography-guided injection was not expected to be an effective stand-alone treatment. Two participants anticipated a short period of pain relief, giving them a chance to address the underlying condition. ‘Long term solution and I see this (USGI) as a step in that process. It gives you a window of opportunity to do the rehab.”
Expectations regarding periprocedural pain were mixed; however, it’s notable that none of the participants reported experiencing pain during USGI. Preconceptions varied widely, ranging from: “fairly smooth relatively painless procedure.” to “Absolute agony. I expected to faint. I expected to not be able to use my hand properly for a period of time after that.”
Two participants reported that their expectations were not met following USGI. An example response was, “Were my expectations met? No, they weren’t. It could be technically the injection was a success. Since then, I feel I might as well not have had the injection.”
The third sub-category related to the effectiveness of post procedural rehabilitation on the success of the USGI. Attaining increased mobility and diminished pain, following what was described as a “relatively painless procedure” by one participant, did not always equate to resounding success. For some, the preconception that USGI presented a “window of opportunity to start the cure” (P3) correlated with their perceived success of the procedure. Notably, three out of seven participants believed that success was intricately tied to the effectiveness of a post-injection rehabilitation program. This is a sample response: “The injection is a sort of a step one to allow physio really. It’s just a precursor. More mobility in knee and start rebuilding it.”
Category 2: Patient Education
This category related to how the appointment for USGI, contributed to enhancing patient comprehension regarding underlying pathology, symptom management, and rehabilitation requirements. It illuminated the role of DMS and clinicians in providing patient education.
The first subcategory described the effectiveness of DMS as a multi-media feedback tool. Six out of seven participants reported that DMS is a highly effective educational tool that provides visual feedback. This resulted in an enhanced overall patient experience. An example was provided in this statement, “I understood the problem much more seeing the problem, and you can get your head around that. I know how to work with it to stop it happening again.”
The second subcategory related to the effectiveness that clinician communication has on the outcome of a USGI. All participants believed that the clinician played a pivotal role in the patient experience. A common theme was a calm and professional demeanor, which was highly rated by five participants, here is an example, “good bedside manner, coming across competent and caring.” Additionally, three participants reported that a realistic discussion, that was free of technical terms or “jargon,” was important for managing expectations and achieving a successful outcome. Facilitating a genuine discussion allowed the clinician to gain patient confidence and manage expectations. Here is a sample participant response: “I would rather know exactly where I stand rather than someone be overly optimistic. A reassuring voice. Left me with clarity as to what the injury is and what a realistic expectation would be for outcome.”
The third sub-category highlighted the patient’s understanding of the mechanism of action of an injection. When participants were asked, “How do you think a steroid injection works?” there was a unanimous belief that a steroid injection functions by diminishing inflammation, thereby restoring mobility and alleviating pain. A participant’s quote was, “(It) reduces the inflammation, it goes inside to reduce inflammation and brings back mobility.”
The fourth subcategory related to the perceived benefit of post-procedural correspondence. All participants received a clinical procedure letter that explained their diagnosis and the USGI procedure that they had undergone. The participant’s reported these letters to be beneficial to other physicians and healthcare professionals, as needed. One participant remarked, “Only to hand to my doctor he used more medical terms in the letter, already explained to me in non-medical terms so I knew exactly what the letter was containing.”
Category 3: Private vs. NHS
This category described how the closure of NHS MSK services during the COVID-19 pandemic influenced participants’ choices to seek a private office for USGI. It also underscored the perceived disparities in continuity of care between the private sector and the UK NHS.
The first subcategory highlighted participant difficulties with assessing NHS treatment, prolonged waiting lists, and canceled MSK services, which resulted in three participants seeking a private office for USGI. An example participant response was, “Thinking about procedure for 6 months, with COVID-19 having treatment on the NHS means there was no chance.”
The second subcategory reflected the perceived importance of continuity of care. All participants appreciated the fact that their private USGI was completed by one clinician in one appointment. Here is an example statement, “Very good to have it all in one place. The whole thing was dealt with as a whole. You feel you are being passed from pillar to post (NHS service).”
The third subcategory related to the belief that USGI could only be performed in the private sector. One participant believed the NHS did not undertake USGI’s and, therefore, sought a private procedure and stated the following, “I could have gone to the NHS but I decided not to because they don’t have USGI, so that’s why I went private.”
Discussion
The aim of this study was to explore patient experiences after receiving a USGI given by an APP. This is likely to be the first qualitative study to provide an analysis of patient experiences, undergoing a USGI procedure, completed by an APP. This study highlighted the important role that the APP has when providing a USGI. The ability to convey important information and educate the patient about their diagnosis was seen as an important factor in managing patient expectations. Having the ability to discuss both the imaging and treatment in a free and open manner increased these participants’ understanding and their perceived outcomes. The ability to select a specific clinician, rather than an individual search or peer referral, was indicated to positively impact the USGI outcome. This supports previous research which revealed positive treatment expectations were associated when a personal recommendation was made to a particular clinician.34 –36
Participants of this study highly valued the DMS diagnostic capabilities and the precision of USGI. Previous research consistently shows that DMS enhances patient satisfaction by confirming a diagnosis.37,38 The current study also demonstrated this fact. Participant satisfaction, in the current study, was linked to increased confidence in diagnostic accuracy, monitoring pathology, and improving adherence to treatment. 39 All participants believed USGI more accurate and effective than non-guided injections, consistent with a systematic review that demonstrated increased accuracy in upper and lower limb USGIs. 40
Existing evidence has suggested that USGI is safer than unguided injections.12,13 A systematic review on patient expectations found that 65% tended to overestimate treatment benefits, while 50% underestimated the risks. 41 Participants in this study found USGI highly effective and safe, with no reported concerns for safety. However, opinions on the safety of USGI compared to non-guided techniques varied. Furthermore, some participants were concerned about the potential side effects of oral painkillers, which strongly influenced their decision to choose a USGI. Contextual factors can significantly impact patient outcomes. 36 Interestingly, more invasive interventions tend to yield more favorable results, as observed in a study where injections had a stronger effect than oral medication. 35 In the current study, participants reported positive experiences associated with USGI, with high treatment expectations, that possibly amplified the placebo effect.
Treatments targeting fear and anxiety have been shown to improve treatment outcomes.42,43 However, the results of the current study do not provide conclusive evidence in this regard. Surprisingly, none of the patients reported experiencing pain during the procedure, with three participants choosing not to watch it; however, the experience of pain was not explored or measured during the data collection process. Future research including the assessment of pre- and post-USGI pain by recording their responses, with a Likert scale, would be advocated.
Past research suggests that expectations are shaped by previous experiences.35,38,44 This prompts questions about whether watching the procedure could lead to positive outcomes in anxious patients. This would be an aspect for further research and investigation.
A recent systematic review found that patients with a strong internal health locus of control are more likely to make healthy choices, seek medical help, and adhere to treatment plans.
The proactive approach of seeking a private USGI, which was observed in the current study, may explain the positive outcomes noted. Research exploring patient expectations of USGI undertaken by an APP, in an NHS setting, is needed. Carroll et al. 44 suggested that “expectation is a self-fulfilling prophecy,” with positive attitudes associated with better outcomes. 43 In the current study, participants strongly believed USGI would provide rapid pain relief, which was realized in the majority of cases. Ultrasonography-guided injection was viewed as a “window of opportunity” for addressing underlying pathologies. Whether self-empowered patients with positive attitudes and self-management skills consistently achieve better outcomes is uncertain. Once again, further research is needed to assess the effect of patient attitude on treatment outcomes.
Limitations
This was a qualitative study that was based on a small sample of participants. Although data saturation was achieved with seven interviews, expanding the study to include NHS patients could have strengthened the findings. Due to the investigators (LM, CM, and DB) working within a private office setting, participants were exclusively non-NHS patients with similar characteristics. Furthermore, all had prior negative experiences with the NHS, possibly influencing their views toward private sector services. These findings are context-specific and may not apply to other MSK patient groups. To enhance transferability, more diversity of participants, including NHS patients, would be important in future studies.
Conclusion
The aim of this study was to explore patient experiences after receiving a USGI from an APP. The study found that participants highly valued the use of both DMS and USGI, as well as acknowledging its precision and effectiveness. Most of the participants reported significant pain relief. The presence of these skilled clinicians and their patient outcomes were linked to their engagement with patients, shared decision-making, provided clear information, set realistic expectations, and maintained high professional standards. This qualitative study can serve as a foundation for broader and more comprehensive research on this topic. Future research in the use of USGI should include a larger cohort of participants and sample and incorporate patients in a more (NHS) hospital-type setting.
Footnotes
Acknowledgements
The authors thank Dr. Lee Cameron, Consultant Physical Therapist, Royal Gwent Hospital, Newport, Wales, for his guidance and support. The authors extend their gratitude to Mr. Anuj Punnoose, Clinical Specialist Physical Therapist & NIHR Doctoral Fellow, Cambridge University Hospitals NHS Foundation Trust, for his contributions to the drafting and preparation of this paper. None of the above personnel were compensated for their contributions.
Ethics Approval
Ethical approval for this study was obtained from the University of Hertfordshire’s ethics board (HSK/PGT/UH/04283).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.