
Abstract
Objective:
This study aimed to evaluate whether serial evaluations of cervical length (CL) have the potential to determine preterm labor in women with threatening preterm labor (TPL).
Materials and Methods:
This prospective study included pregnant women at 24 to 37 weeks of gestation referred to our institute because of TPL. Cervical length was measured at three successive time points using transvaginal sonography (upon admission, one-, and two-weeks post-admission). Data were analyzed using both parametric and non-parametric statistics.
Results:
The mean age of the 126 patients included was 25.60 ± 6.48 years, with age ranging from 14 to 42 years. The mean pregnancy age, at the time of the sonogram, was 33.54 ± 2.78 weeks. The initial CL had an area under the receiver operating characteristic curve (AUROC) of 0.854. The CLs measured one and two weeks later had AUROCs of 0.868 and 0.870, respectively. Based on these data, the cut-off points of 28.5 and 27.5 mm were identified for the initial and subsequent two-week CL measurements, respectively, capable of predicting preterm delivery. If the CL measured at initial admission was >28.5 mm, the likelihood of timely delivery was 92.22%. However, if the CL measured at initial admission was <28.5 mm, the chance of premature preterm delivery increased by 2.3 times. Patients with a CL <27.5 mm in the second week were 18.75% more likely to have a preterm delivery. If the CL was >27.5 mm, the probability of timely delivery was 89.7%.
Conclusion:
In this cohort of women, serially measured CLs taken during transvaginal sonography demonstrated promise as a method for indicating the possible risk of preterm delivery. Thus, measured CL may be a useful diagnostic component for prenatal care, as well as for classifying the risk of preterm delivery. Nevertheless, further studies are required to confirm the effectiveness and safety of these sonographic measures in larger and more diverse patient cohorts.
Spontaneous preterm birth, defined as delivery before 37 weeks of gestation, is a significant public health concern that accounts for a substantial proportion of perinatal morbidity and mortality.1,2 Thus, accurate prediction and effective clinical management of preterm labor (PTL) are critical and challenging aspects of maternal-fetal medicine.1 –3 Studies have shown that measuring the cervical length (CL) during transvaginal sonography between the 20th and 24th weeks of pregnancy can be effective in predicting PTL because of a higher likelihood of PTL as CL decreases. 3
Some medical practitioners also perform CL measurements during the later stages of pregnancy. However, limited information is available on how accurately CL measurements, after 24 weeks gestation can predict spontaneous preterm birth (sPTB). Some studies have suggested that CL measurements post-24 weeks of gestation may aid in predicting sPTB, and various risk estimates have been formulated using logistic regression analyses.4–6 Moreover, the correlation between the diagnostic signs of PTL and the CL measurement can enhance our understanding of sPTB prediction. Research has indicated that patient symptoms such as regular uterine contractions, pelvic pressure, and changes in vaginal discharge, paired with a CL <27.5 mm, increase the likelihood of delivery within a week. 7 Furthermore, a significant decrease in measured CL, of >10 mm, paired with a change from an asymptomatic to a symptomatic state, has been linked to a higher risk of sPTB. 7
Cervical length <25 mm during the mid-trimester gestational phase is also considered indicative of an increased risk of sPTB. 8 However, some studies have shown that only a small percentage of women with sPTB have shorter CL measurements.9,10 Instead, a substantial number of women with sPTB do not exhibit CL measurements <25 mm. This diagnostic finding suggests that although a shortened CL in the mid-trimester is a strong predictor of sPTB, it is not a universal indicator, highlighting the complexity of predicting PTB.9,10
Alterations in CL measurements throughout pregnancy can be considered progressive. 11 Moreover, repeated measurements have shown that natural modifications occur in the uterine cervix before spontaneous delivery. These alterations can occur suddenly or develop over time, often spanning two or more weeks before the onset of labor. 12 While serial CL measurements have been explored in twin and triplet pregnancies, its application in singleton pregnancies remains underreported.13 –15 Chiossi et al. examined serial CL measurements in singleton pregnancies, particularly in the context of threatened preterm labor (TPL). Their diagnostic findings highlighted the predictive value of CL measurement in such cases and emphasized its clinical relevance. 15
These insights inform the direction of the current research, emphasizing the evaluation of repeated CL measurements within the context of preterm labor symptoms in singleton pregnancies. Therefore, this study aimed to refine the prediction and management approaches for sPTB, thereby leveraging the observed correlations to enhance maternal-fetal outcomes.
Materials and Methods
This prospective cohort study included pregnant women aged ≥18 years, at 24 to 37 weeks of gestation, who were referred to the medical center between April 1, 2020 and August 1, 2021. The inclusion criteria were women with TPL presentations including abdominal pain, positive tocodynamometry, abdominal cramps, back pain, and feeling pressure in the pelvic area. The exclusion criteria were as follows: women <18 years of age, underlying diseases (e.g. gestational diabetes, pregnancy hypertension, multifetal pregnancy, preeclampsia, rupture of membranes, and polyhydramnios), intrauterine growth restriction (IUGR), uterine abnormalities, fetal abnormalities, history of cesarean section in a previous pregnancy, and other similar factors that may have caused PTL.
Informed consent was obtained from all patients who were assured that they could leave the study at any time, and patient confidentiality was maintained. The patient’s treatment regimen did not change. No additional expenses were incurred by the patients. The researchers complied with the tenets of the Declaration of Helsinki at all stages. This study was approved by the local hospital’s ethics committee (IRB.zums.rec.1398.383).
Pregnant women with TPL admitted to the labor and delivery areas were examined by a gynecologist and perinatologist for vaginal issues and underwent transvaginal sonography. The CL was measured as part of the sonogram. Patients with cervical dilatation >3 cm or effacement >80% were diagnosed with PTL and were prescribed tocolytics or corticosteroids. Tocolysis involves the use of medications (nifedipine or magnesium sulfate) to delay labor and provide additional time for fetal development in cases of TPL. Conversely, corticosteroids (betamethasone or dexamethasone) are administered to promote lung maturity, which is crucial for managing preterm labor and improving neonatal outcomes.
Patients with dilatation <3 cm and <80% effacement were likely to be diagnosed with TPL. These patients were re-examined 30 to 60 min after the initial examination. If the dilatation was found to have changed with an effacement >80%, tocolysis and corticosteroids were prescribed; otherwise, decisions were made based on the measured CL. Patients with CL <20 mm were prescribed tocolysis.
Patients with cervical dilatation <2 cm and effacement <80% were suspected to have PTL and were re-examined 2 hours later. If cervical dilatation changed by 1 cm, effacement increased by >80%, or the CL was <20 mm, tocolysis and corticosteroids could be prescribed (see Figure 1).
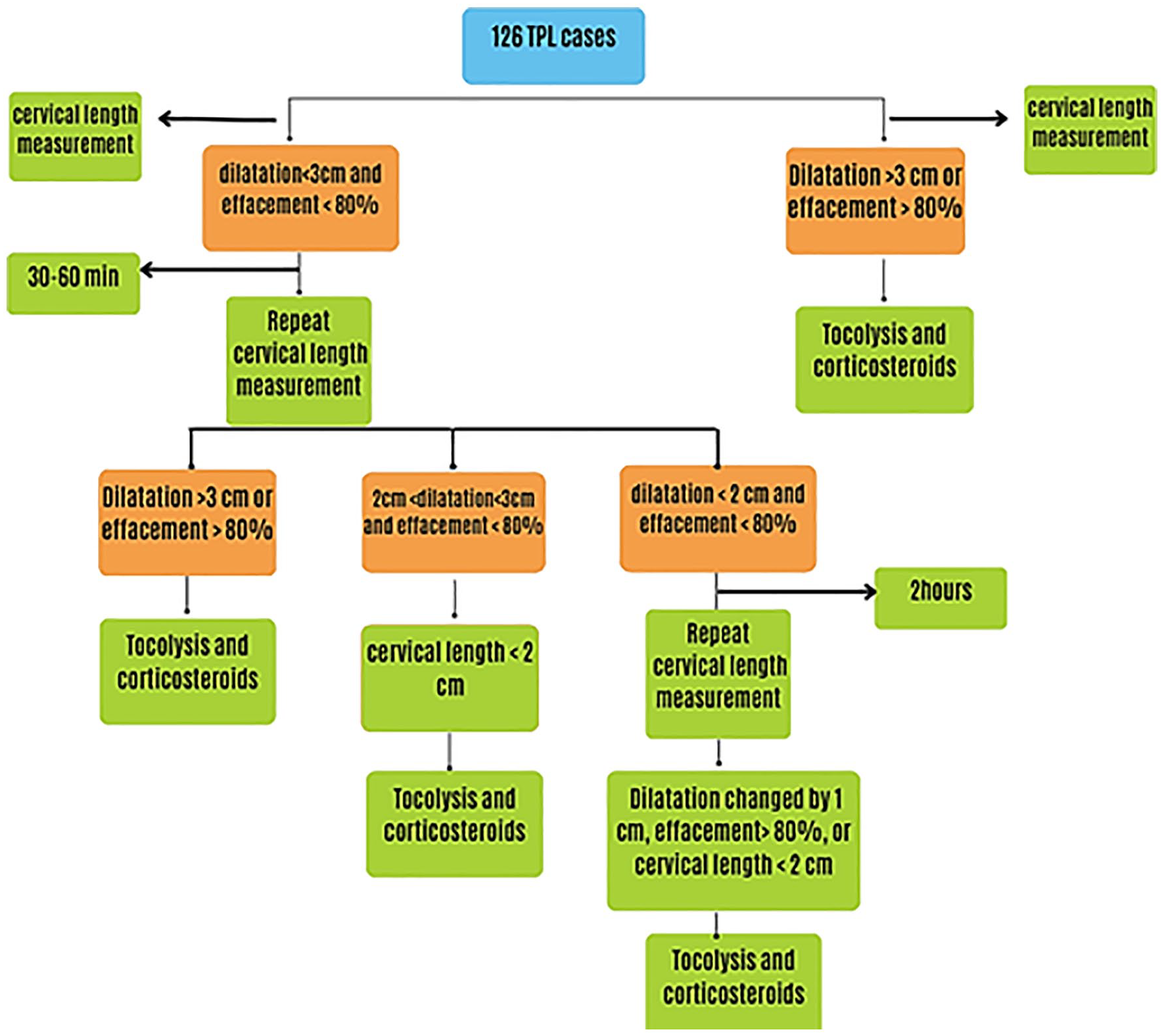
Diagnostic decision tree used in the clinical management of patients suspected with threatened pre-term labor (TPL).
Women at 26 to 32 week gestation and predicted to deliver their babies within 12 h were prescribed neuroprotective magnesium sulfate. After 24 hours of hospitalization, CL was measured. When these women failed to deliver, CL was measured one week later and then again two weeks later. The patients underwent follow-up interventions until delivery.
Transvaginal Sonography
Transvaginal sonography and CL measurements were performed using a standardized imaging approach. The assessment was performed in singleton pregnancies hospitalized between 24 and 37 weeks of gestation presenting with painful contractions and cervical changes. Sonographic evaluations were performed using a 7 to 9 MHz transvaginal transducer and were completed by trained obstetricians and gynecologists. Repeated sonography was performed in cases where the patients had a dilatation <3 cm and <80% effacement in the first examination. Similarly, sonography was repeated if the cervical dilatation was <2 cm and the effacement was <80% in the second examination (see Figure 1). During each visit, the physician performed transvaginal CL measurements. Patients were placed in the dorsal lithotomy position and instructed to empty their urinary bladder prior to imaging.
A precise set of criteria was considered to ensure the image quality and measurement accuracy. Each sagittal sonographic view was required to clearly display the entire cervical canal from the internal to the external os in a straight or minimally curved alignment. Special attention was given to the visualization of the endocervical canal, ensuring that both the internal and external os were distinctly visible for an accurate assessment of the CL. Sonograms were evaluated for clarity and focus, with adjustments made to the positioning of the transducer as necessary to achieve an optimal view, particularly in cases where the cervical canal appeared curved. The presence and extent of cervical funneling were carefully documented, with measurements taken during periods of uterine quiescence to avoid the potential shortening effect of the contractions. Multiple measurements (at least three) were performed to establish consistency, using the median or mean value for analysis. The duration of the sonogram was at least 3 minutes to allow dynamic changes such as funneling to be observed, especially in cases of a curved cervical canal. Cervical length measurements were avoided during uterine contractions to ensure accuracy (see Figure 2).
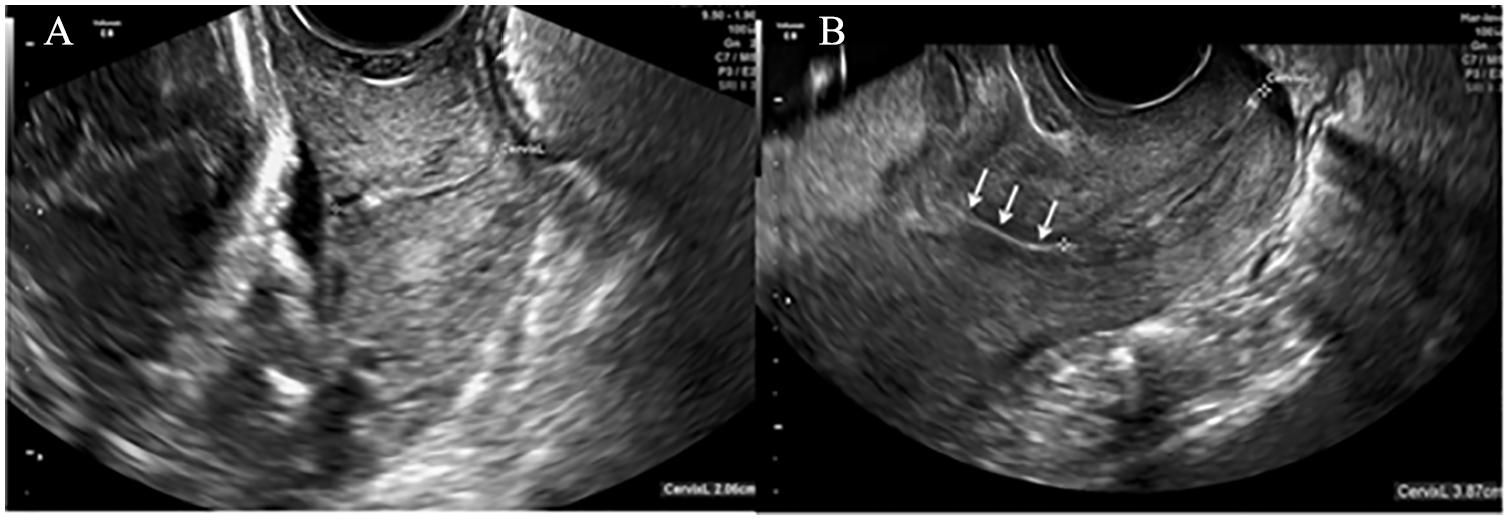
Sample sagittal transvaginal sonographic views of normal cervical length (A) and an example of shorten cervical length (B).
Statistical Analysis
Data were entered into IBM SPSS Statistics for Windows version 22 (IBM Corp, Armonk, New York). Continuous variables are reported as means and standard deviations (SDs), while discrete variables are reported as frequencies and percentages. All statistical tests were performed in pairs. The Kolmogorov-Smirnov test was performed to examine the normality distribution of the data. Non-parametric tests were used for non-normal distributions, whereas parametric tests were used for normal distributions. Normally distributed data are reported using means and standard deviations, whereas non-normally distributed data are reported using median values. The t-test and Mann-Whitney U-test were used to compare the two groups in parametric and nonparametric cases. Statistical significance was set at P < .05.
Descriptive statistics were used to characterize the demographic and obstetric characteristics of the patients. A multivariate logistic regression model was used to control for confounding variables. Using this statistical model, the association between CL <28 mm at the first week, CL <27.5 mm, and the time of delivery was described.
Results
The mean age of the 126 patients was 25.60 ± 6.48 years and ranged from 14 to 42 years old. The most frequent symptoms were abdominal pain (73.8%) and back pain (42.9%). The mean pregnancy age, at the time of the sonogram, was 33.54 ± 2.78 weeks. Of the 126 patients, 12 (9.5%) had no history of abortions, whereas others reported a history of one to four abortions. Overall, 18 (14.3%) patients had preterm delivery cases, with two patients experiencing premature rupture of membranes (PROMs). Contraction diversions were evaluated to be 34.10 ± 6.58, with one (40.5%) patient having severe contractions.
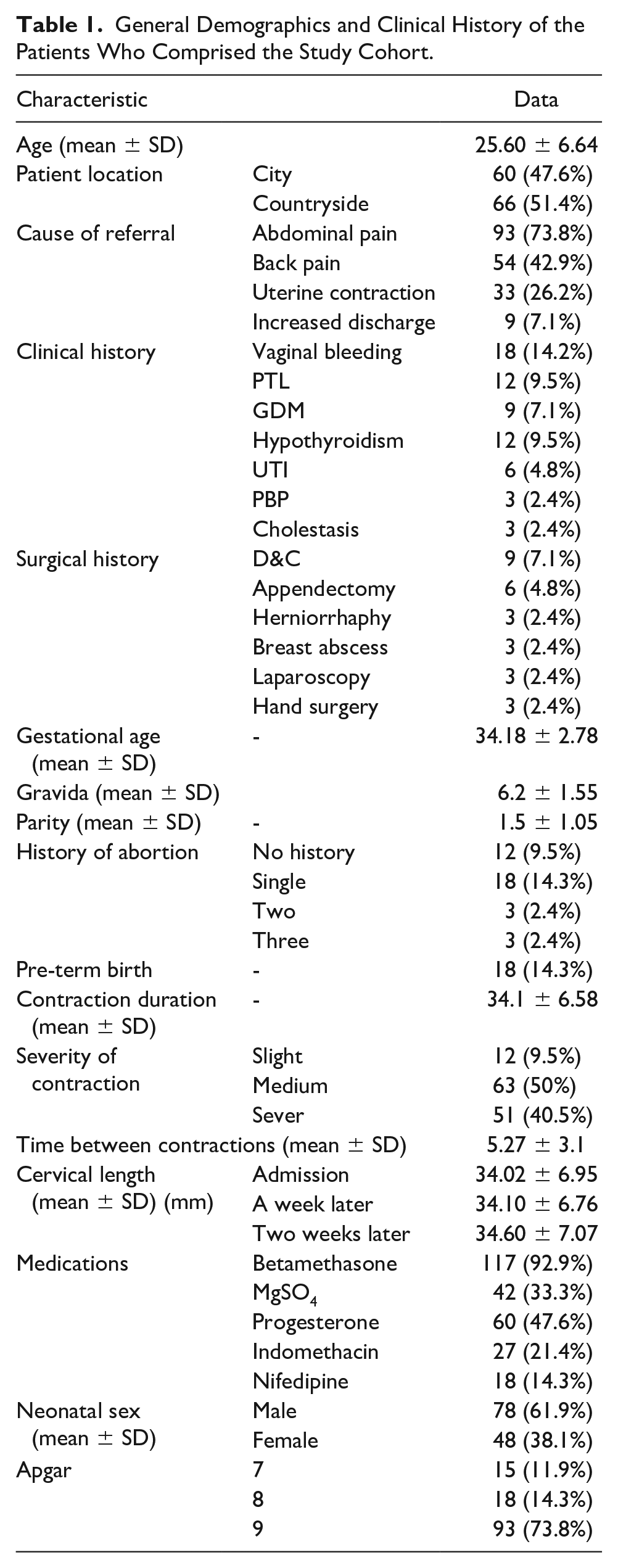
Of the 126 patients, 117 (92.9%) required betamethasone administration. Progesterone was administered to 60 (47.6 %) patients, magnesium sulfate to 42 (33.3%), indomethacin to 27 (21.4 %), and nifedipine to 18 (14.3 %). The mean age of pregnancy at the time of delivery was 36.83 ± 2.34 weeks. The mean newborn weight was 2951.19 ± 460.94 g. In addition, 78 (61.9%) infants were males, and 48 (38.1%) were females. In terms of Apgar score, 15 (11.9%) infants scored seven, 18 (14.3%) scored eight, and 93 (73.8%) scored nine. A significant difference in measured CL was noted between patients who had a history of abortions (24.25 ± 8.03 mm) versus those who did not (28.12 ± 6.76 mm). The frequencies of PTL in patients with and without a history of abortion were 30.0% and 15.6%, respectively, which were not statistically significant (P = .080) (see Table 1).
General Demographics and Clinical History of the Patients Who Comprised the Study Cohort.
In this study, preterm delivery refers to delivery before 37 weeks of gestation; if it occurred at 34 to 37 weeks, it was considered later preterm delivery. A premature preterm delivery was defined as delivery before 34 weeks of gestation. The minimum and maximum CL measurement in this cohort was 8 and 44 mm, respectively. At the initial sonographic examination, 67 patients had a CL <28.5 mm, of whom 52 (77.6%) had a timely delivery and 15 (22.4%) had a preterm delivery. However, out of the 57 patients with a measured CL ≥28.5 mm, 54 (94.73%) had timely delivery, and 3 (5.27%) had preterm delivery. Cervical length was significantly correlated with preterm delivery, with a measured CL of <28.5 mm, indicating a rate of 22.39% of preterm delivery (positive predictive value [PPV]). A CL of >28.5 mm had a 94.7% likelihood of timely delivery (negative predictive value [NPV]). If the CL was <28.5 mm, the chance of premature preterm delivery increased by 8.5 times (odds ratio [OR] = 8.5), whereas a CL < cut-off point could double the chance of late preterm delivery.
Receiver Operating Characteristic Curve Graph
Using the area under the receiver operating characteristic (ROC) curve analysis, the initial CL was area under the ROC curve = 0.854, the measured CL one week later yielded an area under the receiver operating characteristic curve (AUROC) curve = 0.868, and the CL recorded two weeks later provided an AUROC curve = 0.870. These were all capable of distinguishing and predicting preterm from full-term deliveries. Based on these data, the cut-off point of 28.5 mm was identified for the initial CL (with a sensitivity of 83.3 and specificity of 83.3%), the cut-off point of 28.5 mm was underscored for the following week’s measured CL (with the sensitivity of 86.1% and specificity of 83.3%), and the cut-off point of 27.5 mm for the subsequent two-week CL measurement (with the sensitivity of 86.1% and specificity of 83.3%) was capable of predicting preterm delivery. Using trend analysis, CL measurement changes within two weeks of examination did not indicate a significant difference between the two groups. Considering the changes in the CL, within two weeks of examination, no significant differences were noted between the two groups at the time intervals. The change in the measurement trend was not significant between the two groups, and the measurement trend did not predict preterm delivery (see Figure 1).
Predictive Values
The measured CL of the 72 patients in the first week was lower than the cut-off point of 28.5 mm and in the second week, 48 patients had a CL <27.5 mm, with the cut-off point of 27.5. There were 19.44% of patients whose CL was less than the cut-off point of 28.5 mm and were thus likely to be at risk of preterm delivery (PPV). In contrast, if their CL measured in the initial admission week was >28.5 mm, the likelihood of timely delivery was 92.22% (NPV). If the CL in the initial admission week was <28.5 mm, the chance of premature preterm delivery increased by 2.3 times (OR = 3.19), with a chance of late preterm birth being 1.77 times higher. Patients with a measured CL <27.5 mm in the second week were 18.75% more likely to have a preterm delivery (PPV). In contrast, if the CL was >27.5 mm, the probability of timely delivery was 89.7% (NPV), and if the measured CL was <27.5 mm, the risk of premature preterm delivery increased by two times (OR = 2.03), thus increasing preterm delivery likelihood by 62% (see Figure 3).
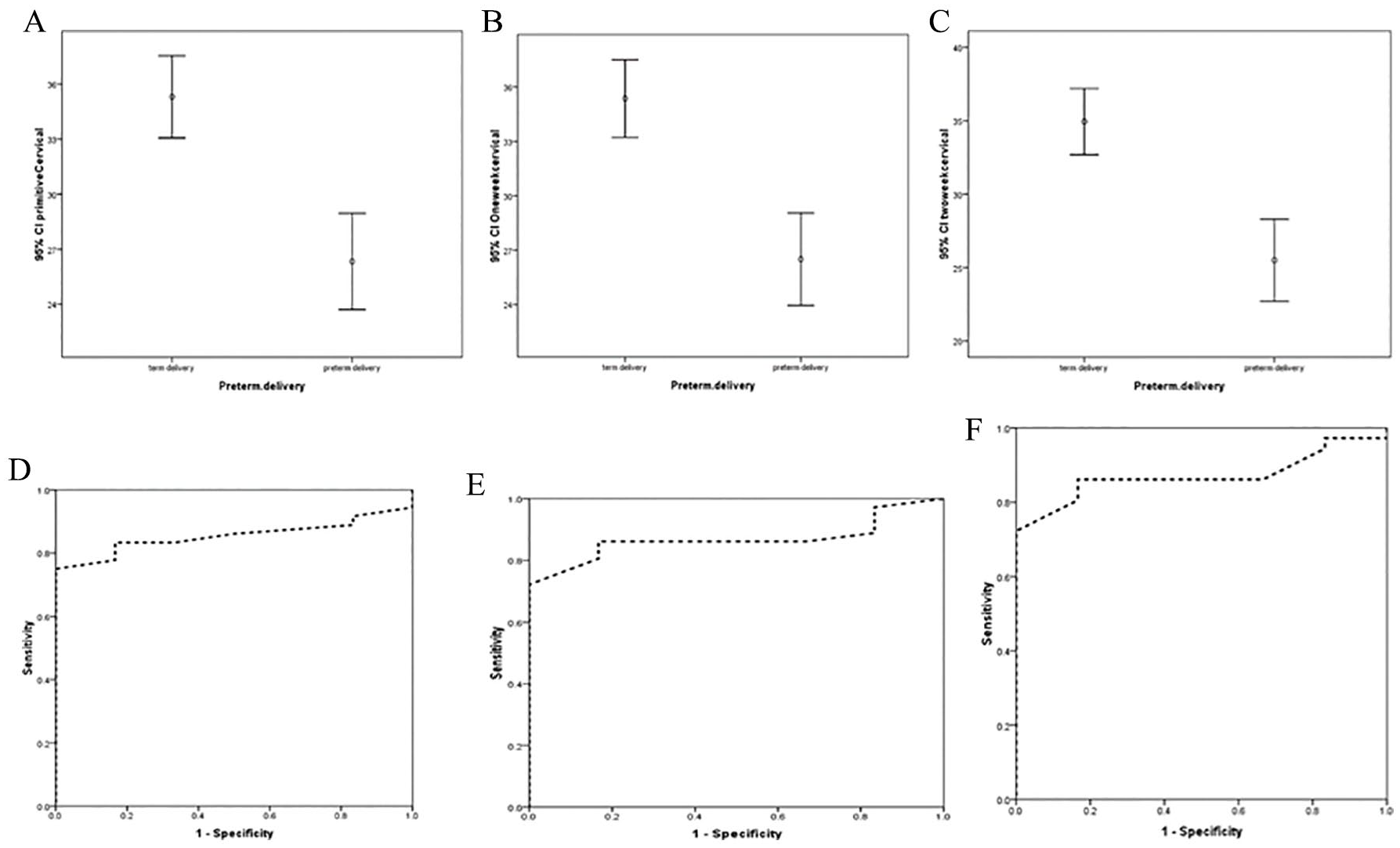
The cervical length (CL) of the patients at admission to the hospital (A), in the first week (B) and at the second week (C) compared to the prevalence of preterm labor. The receiver operating characteristic (ROC) curve of sensitivity and specificity of CL at admission (D), in the first week (E) and at the second week (F), to predict the risk of preterm labor.
Determining the Best Cervical Length Cut-Off Point for Discharging Patients and Reducing Hospital Stay in Cases of PTL
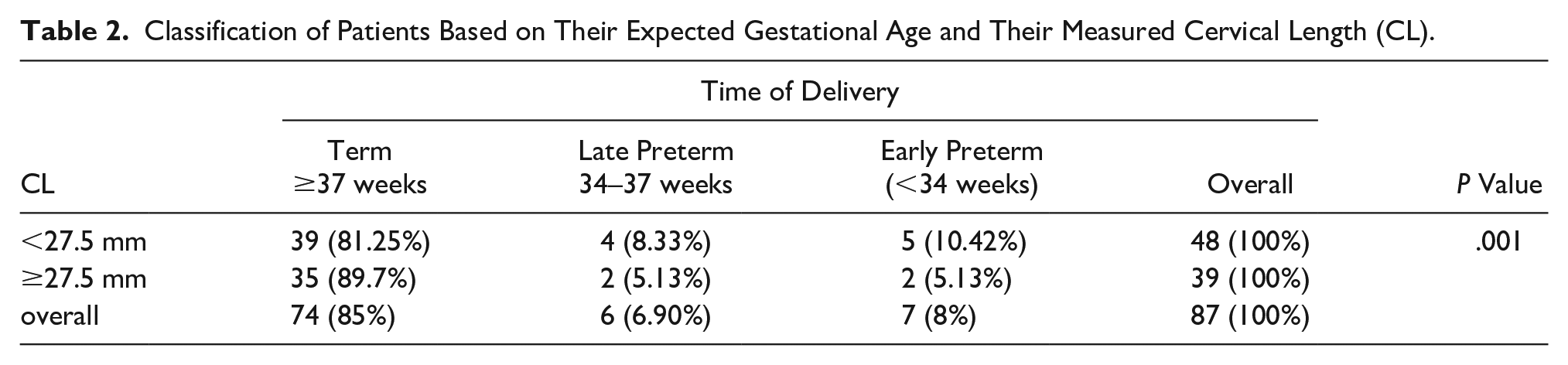
A total of 24 women were hospitalized for more than two days during pregnancy or after delivery. The ROC curve showed that if the measured CL was >25 mm at any of the measurement intervals, patients were less likely to develop complications. Complications included postpartum, premature, and late. Alternatively, these patients were more likely to be hospitalized for a shorter time (see Table 2).
Classification of Patients Based on Their Expected Gestational Age and Their Measured Cervical Length (CL).
Discussion
Cervical length measurement in women with painful uterine contractions prior to 34 weeks of gestation can predict those who gave birth within 1 to 2 weeks.8,16 Thus, CL measurements taken upon admission of patients with symptoms may be beneficial from a short-term management perspective; however, if pregnancy continues, additional CL measurements may be required to determine the risk of spontaneous preterm delivery. A previous study reported that pregnant women with a prior episode of TPL formed a subgroup that was at a high risk of spontaneous preterm delivery. 17 In this subgroup, 45% of patients were re-hospitalized, and a second episode of TPL demonstrated that 25% to 30% could give birth to a preterm infant. 18 Therefore, the identification of this subgroup is highly critical to optimize pregnancy outcomes and rationally justify their clinical management. Thus, this study aimed to determine whether serial measurements of CL among women who did not give birth following the first TPL episode helped identify those who might give birth prior to 37 weeks of gestation.
Our results indicated that sPTB can be predicted for patients who present with symptoms of sPTB and a CL <28.5 mm at their first visit (with a sensitivity of 83.3% and specificity of 83.3%). The corresponding rates of sensitivity and specificity for these patients with CL <27.5 mm at two weeks after their symptoms were 86.1% and 83.1%, respectively. Esplin et al. considered a measured CL of 25 mm as the diagnostic cut-off value and reported an area under the curve (AUC) of 0.67 (95% confidence interval [CI]: 0.64–0.70) and used this factor in predicting sPTB. 18 Furthermore, several prospective observations of 105 women with PROM between 23 and 33 weeks of gestation revealed that 40% of them had a vaginal CL <20 mm, similar to the PPV of delivery, with 62% occurring within seven days. 19 This study indicated that patients with a measured CL <28.5 mm at the time of presentation had a 19.44 PPV for developing PTL. In addition, Ghiossi et al. reported that if the measured CL was <10 mm, at least in a single case and four weeks following the cessation of regular uterine contractions, spontaneous preterm delivery would be three to seven times more likely compared to that in patients with a measured CL that remained stable at ≥10 mm. 15 In contrast, this study demonstrated a threefold higher risk of preterm birth among patients with a measured CL <28.5 mm. This difference in outcomes may be because of the gestational age at which the patients were measured and the variance in the patients enrolled in the two different studies.
A retrospective study by Wagner et al. assessed 310 singleton pregnancies that had preterm contractions, between 24 ± 0 to 33 ± 6 weeks and a measured CL, which was completed upon admission and re-measured approximately 3.6 days later. 20 The efficacy of delivery prediction within 14 days improved when either the initial or subsequent CL measurements were combined with their differences compared to a single evaluation. Sotiriadis et al. investigated 122 patients with premature contractions and evaluated their CL at presentation and 24 hours later. Their results indicated that the reliability of the initially measured CL in predicting delivery within a week was enhanced when considering the variance between the two measurements. 21 However, Rozenberg et al. analyzed 107 high-risk patients, measured CL at presentation and 48 hours later, and deduced that integrating the difference between the two CL measurements did not boost the prediction of PTL. 22 Similarly, this study did not confirm any notable augmentation in the prediction. The diminishing trend of CL, as documented during pregnancy advancement, may suggest that the predictive precision of CL, with sonography for those at risk of premature delivery, hinges on the gestational age at presentation, and that the predictive cut-off for preterm delivery is specifically related to the gestational age. 23 This is because a cut-off value of 28.5 mm effectively identified those at risk of preterm delivery before the 37th week.
Thus, serially measured CLs may increase the risk prediction of sPTB, which is crucial in high-risk patient groups with a history of TPL.11,15 These measurements can guide critical decisions regarding the administration of antenatal corticosteroids, necessity for bed rest, and use of tocolytic agents, thereby optimizing clinical outcomes. This approach aids in immediate clinical decision making and long-term management strategies for patients at risk of preterm delivery.11,15
Limitations
The major limitations of this study were the research design and convenient sampling of patients who pose a major threat to the internal and external validity of the results. In addition, only a few patients had pregnancies that lasted up to the second week, and that could have affected the reliability of the second week results and the PPV of the “difference of the two measurements.” In addition, fetal fibronectin levels were systematically examined after presentation. Identifying glycoprotein levels can enhance the prediction of preterm delivery risk in symptomatic individuals. Subsequently, patient treatment adhered to established national protocols encompassing tocolysis and antibiotic procedures, which might have influenced the universal applicability of the results of this study.
Conclusion
In this patient cohort, serial measurements of the CL completed during transvaginal sonography demonstrated promise as a technique for determining the risk of preterm delivery. Additional studies and replication of these results are necessary to confirm the effectiveness and safety of gauging risk using measured CL. Data from the measured CL may be a useful component of prenatal care for classifying preterm delivery risk in similar patient cohorts; however, this is subject to validation in larger and more diverse patient cohorts.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the local hospital’s ethics committee (IRB.zums.rec.1398.383).
Informed Consent
Verbal informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.