
Abstract
Objectives
As welfare societies, Scandinavian countries share characteristics of equality related to healthcare access, gender, and social services. However, cultural and lifestyle variations create country-specific health differences. This meta-analysis assessed the prevalence of preterm birth (PTB) and its categories in Scandinavian countries.
Methods
A systematic search in key databases of literature published between 1990 and 2021 identified studies of the prevalence of PTB and its categories. Following the use of the Freeman–Tukey double arcsine transformation, a meta-analysis of weighted data was performed using the random-effects model and meta-prop method.
Results
We identified 109 observational studies that involved 86,420,188 live births. The overall pooled prevalence (PP) of PTB was 5.3% (PP = 5.3%, 95% confidence interval [CI] 5.1%, 5.5%). The highest prevalence was in Norway (PP = 6.2%, 95% CI 5.3%, 7.0%), followed by Sweden (PP = 5.3%, 95% CI 5.1%, 5.4%), Denmark (PP = 5.2%, 95% CI 4.9%, 5.3%), and Iceland (PP = 5.0%, 95% CI 4.4%, 5.7%). Finland had the lowest PTB rate (PP = 4.9%, 95% CI 4.7%, 5.1%).
Conclusions
The overall PP of PTB was 5.3%, with small variations among countries (4.9%–6.2%). The highest and lowest PPs of PTB were in Norway and Finland, respectively.
Keywords
Introduction
Preterm birth (PTB) is defined by the World Health Organization as live births before 37 completed weeks of gestation.1,2 PTB is a major risk factor for neonatal mortality and morbidity and is one of the most important health problems worldwide. Approximately one-third of neonatal deaths are related to PTB. In 2015, Delnord et al. reported that approximately 75% of all neonatal deaths and 60% of all infant deaths in Europe were directly attributed to PTB.3,4
PTB is the main hindrance to the achievement of the United Nations 2015 Millennium Development Goals, which aim to reduce child mortality by two-thirds. Surviving preterm-born infants are at an increased risk of long-term neurodevelopmental and cognitive impairment, chronic diseases, and mortality later in life.5–7 Additionally, PTB potentially influences health, welfare, and development during adulthood. 8
The rate of PTB varies from 5% to 18% worldwide according to geographic region and income level.8–13 During the last 20 years, the prevalence of PTB has increased worldwide and is expected to continue rising with the growth in other risk factors including advanced maternal age and the popularity of assisted reproduction among women. 9
Given their high human development indices and developed healthcare systems, Scandinavian countries have some of the lowest rates of PTB worldwide. 14 However, a similar growth trend in the aforementioned risk factors has been reported.15,16 Variations exist in the PTB rate between these studies; however, little is known about the rates of PTB categories in these countries. Importantly, the development of effective preventive measures to reduce the incidence of PTB requires a thorough understanding of the epidemiology of this condition.
Therefore, this systemic review and meta-analysis aimed to present the best available peer-reviewed published evidence of the prevalence of PTB and its categories in Scandinavian countries including Norway, Sweden, Denmark, Finland, and Iceland.
Materials and methods
A review protocol was predesigned based on Cochrane’s method for this systematic review and meta-analysis, which followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline.
17
The study protocol includes a detailed description of the study and has been registered on the PROSPERO database (CRD42023396628). The review objectives were as follows:
To study the overall pooled prevalence (PP) of PTB and its categories (including extremely, very, and moderate/late PTB) among the general population of pregnant women in Scandinavian countries, which consisted of Norway, Sweden, Denmark, Finland, and Iceland. To study the PP of PTB and its categories (including extremely, very, and moderate/late PTB) among the general population of pregnant women in each Scandinavian country.
The following Population, Intervention or Exposure, Comparison, Outcome elements were applied as inclusion criteria in this review:
Population: general population of pregnant women; Intervention: None; Comparator: pregnant women with PTB; Outcome: PTB rate; Study design: Observational.
Eligibility criteria
The inclusion/exclusion criteria were established before the literature search. Studies had to fulfill the following criteria for eligibility: peer-reviewed articles that were published in the English language and that included the general populations in each Scandinavian country (Norway, Sweden, Denmark, Finland, and Iceland); having a population-based study design; presenting the total population size and the number, percentage, incidence, or prevalence of PTBs; and accessible in full-text.
Gray literature and non-original studies including reviews, commentaries, editorials, letters, meeting abstracts, case reports, conference proceedings, governmental or organizational reports, dissertations, theses, books, unpublished data, presentations, or any studies that did not provide accurate and clear data were excluded. Moreover, studies were excluded if their definitions of the outcome differed from the pre-specified definition in our review.
Search strategy
A comprehensive computerized literature search was independently performed in the PubMed (including MEDLINE), Scopus, and Web of Science databases by two reviewers (SB-G and MV) and covered the period between 1 January 1990 and 1 February 2022. To maximize the sensitivity of the search, free-text and medical subject heading terms were pilot-tested and were used to search the electronic databases. Furthermore, a manual search of the reference lists of selected studies and other relevant reviews was conducted to maximize the identification of eligible studies. The following keywords were used alone or in combination during the search process: (premature birth OR preterm birth OR premature labor OR preterm labor OR premature labor preterm labor OR adverse pregnancy outcome OR adverse neonatal outcome OR pregnancy complication) AND (prevalence OR incidence OR epidemiology OR rate) AND (Scandinavia OR Nordic OR Denmark OR Norway OR Sweden OR Finland OR Iceland OR Finnish OR Danish OR Nordic OR Swedish). The search string that was used in the PubMed search is presented as an example in Supplementary Table 1.
Study selection and data extraction
Data were independently extracted by two review authors (SB-G and RB-Y) based on the eligibility criteria. When a study separately provided data for the various categories of PTB, the relevant datasets were used for subgroup analyses. Any disagreement between the two reviewers who were responsible for data extraction was resolved through discussion. In the case of missing data or ambiguities in the study design or trial conduct, the study authors were contacted via email and were asked for additional information; in case of no response, the study was excluded from the review. To ensure data collection accuracy before the meta-analysis and prevent bias in data extraction and entry, the data extraction process was double-checked by the two reviewers.
Outcome measures
The primary outcomes of interest were the PP of PTB overall and for the individual countries. The secondary outcome was the pooled risk by PTB category, which included extremely PTB, very PTB, and moderate/late PTB. PTB was defined as any live birth occurring between 22 to <37 weeks of gestation. PTB was further subcategorized into extremely PTB (22 weeks of gestation or birth weight below 500 g to <28 weeks), very PTB (28 to <32 weeks), and moderate/late PTB (32 to <37 weeks).2,18
Quality appraisal
The quality of the included studies was critically appraised for methodological structure and the presentation of results. The Newcastle–Ottawa scale was used to assess the quality of each study. This scale is suitable for the evaluation of non-randomized trials in meta-analyses and evaluates studies based on three criteria: participant selection, comparability of study groups, and assessment of outcome or exposure. A study can be awarded a maximum of four stars for the selection category, a maximum of two stars for the comparability category, and a maximum of three stars for the outcome/exposure category. 19 Studies with scores above 6, 4 to 6, and less than 4 are considered of high, moderate, and low quality, respectively. In addition, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to downgrade the certainty of evidence by considering study limitations, inconsistency, imprecision, publication bias, and indirectness. The GRADE approach categorizes the quality of evidence into four levels: high, moderate, low, and very low. In the GRADE rating system, the initial quality of evidence for observational studies is low. The quality of evidence can be downgraded from a higher to a lower level based on the risk of bias, inconsistency, indirectness, imprecision, and publication bias. Conversely, the quality of evidence can be upgraded from a lower to a higher level based on a large magnitude of effect, the evidence of a dose–response, and the assessment of all plausible residual confounding. 20
Statistical analysis
Heterogeneity was evaluated using the chi-square test, and a p-value >0.05 was interpreted as homogeneity. Heterogeneous and non-heterogeneous results were analyzed using the fixed effects and random-effects inverse variance models to calculate the pooled effect. Publication bias was assessed using the Begg’s and Egger’s tests. A p-value >0.05 was interpreted as indicating no significant publication bias in the meta-analysis. Funnel plots for each outcome were drawn to illustrate publication bias; an asymmetric plot was interpreted as indicating the presence of publication bias.
The trim and fill method was used for correction in case of significant publication results. The meta-prop method was used for the pooled estimation of PTB prevalence after the Freeman–Tukey Double Arcsine Transformation was used to stabilize variances. Forest plots for each outcome and subgroup of the country of origin were also performed. Sensitivity analyses were conducted to identify studies that influenced the estimation of the overall meta-analysis summary. A graph was drawn of the results of an influence analysis in which the meta-analysis was re-estimated by omitting one study at a time. A p-value <0.05 was considered significant, and all statistical analyses were performed using STATA software (version 14; StataCorp Inc., College Station, TX, USA).
Results
Identification of studies and quality appraisal
The literature search yielded 1136 studies, of which 329 studies were further evaluated by retrieving their full texts; 193 studies were subsequently excluded. Ultimately, 109 population-based eligible studies were included in the review. Together, the studies offered extractable data that encompassed 86,420,188 live births for the meta-analysis. A flow diagram of this process is presented in Figure 1.
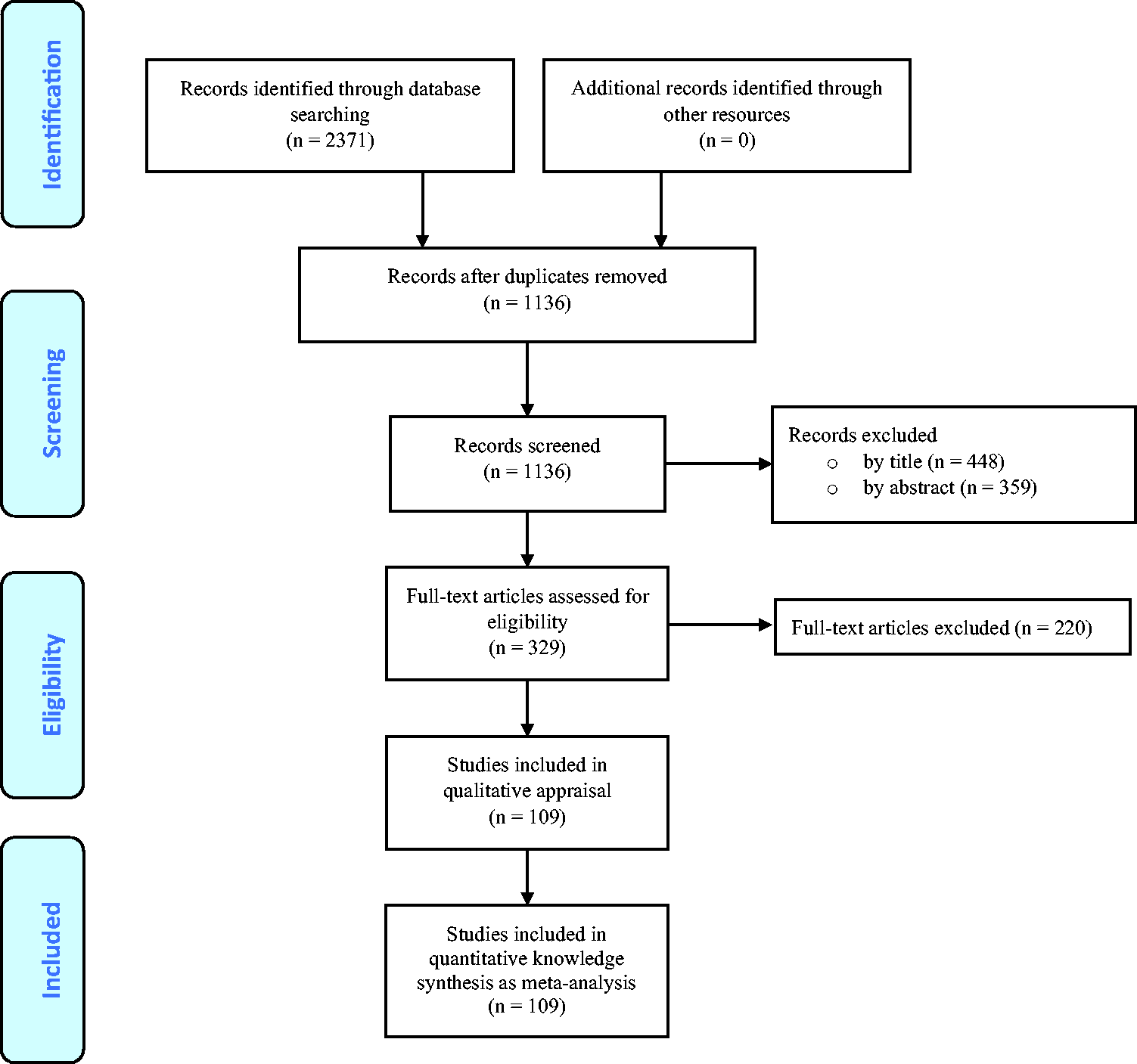
Flow diagram of the search strategy and study selection.
The characteristics and prevalences of PTB for each study are provided in Table 1. The studies were published between 1991 and 2021.
Summary of studies that assessed the prevalence of preterm births.
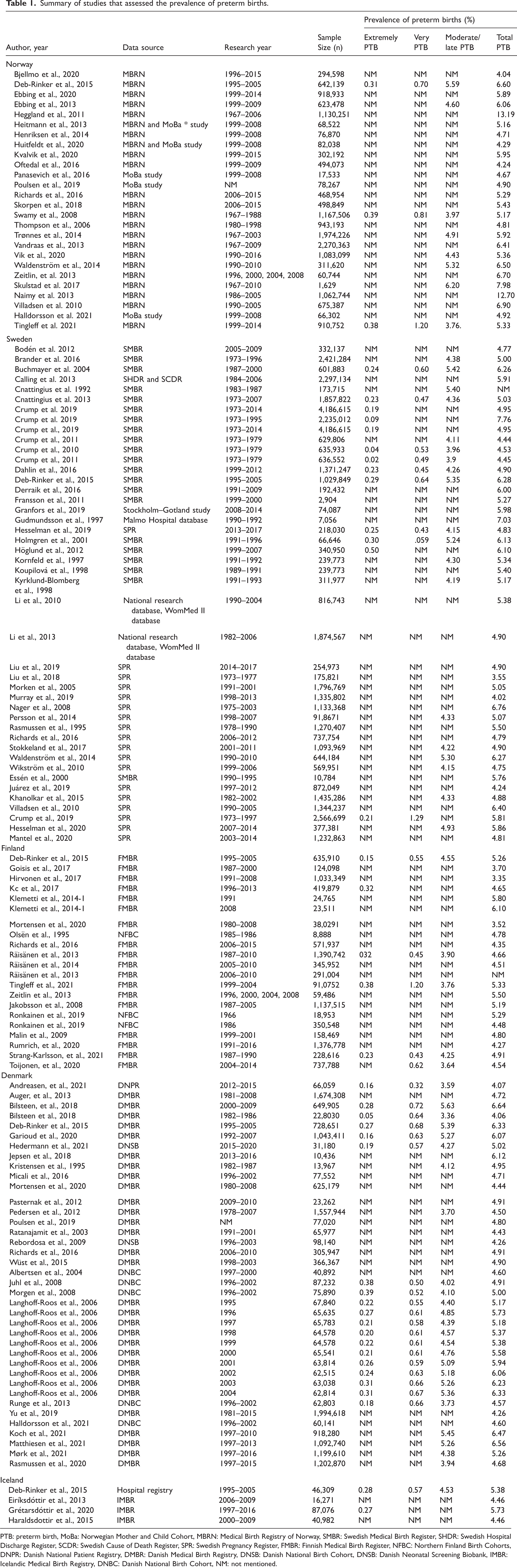
PTB: preterm birth, MoBa: Norwegian Mother and Child Cohort, MBRN: Medical Birth Registry of Norway, SMBR: Swedish Medical Birth Register, SHDR: Swedish Hospital Discharge Register, SCDR: Swedish Cause of Death Register, SPR: Swedish Pregnancy Register, FMBR: Finnish Medical Birth Register, NFBC: Northern Finland Birth Cohorts, DNPR: Danish National Patient Registry, DMBR: Danish Medical Birth Registry, DNSB: Danish National Birth Cohort, DNSB: Danish Neonatal Screening Biobank, IMBR: Icelandic Medical Birth Registry, DNBC: Danish National Birth Cohort, NM: not mentioned.
Sweden had the highest number of eligible studies (44 studies),14,21–63 followed by Denmark (29 studies),15,33,52,64–89 Norway (26 studies),16,33,52,54,59,74,84,90–108 Finland (19 studies),16,33,52,71,108–122 and Iceland (four studies).33,123–125 Given that some studies presented information on more than one country,16,33,52,54,71,74,84,108 the overall sum was greater than 109.Details of the quality assessment of the included studies are presented in Supplementary Tables 2 and 3. Given that narrow inclusion criteria were used in this review, all studies were of moderate or high quality (Supplementary Tables 2 and 3). The overall confidence in the body of evidence in this review was graded as ‘very low’ (Supplementary Table 4).
Meta-analysis
The PP, heterogeneity, and publication bias results are presented in Supplementary Table 5. The overall PP of PTB in the Scandinavian countries regardless of PTB category was 5.3% (95% confidence interval [CI] 5.1%, 5.5%; 4,737,106 events in 86,420,188 participants). However, in various sub-categories, the prevalences of PTB were 4.5% (95% CI 4.4%, 4.7%; 1,537,502 events in 34,517,389 participants) for moderate/late PTB, 0.6% (95% CI 0.5%, 0.7%; 140,806 events in 19,305,652 participants) for very PTB, and 0.2% (95% CI 0.2%, 0.3%; 67,509 events in 30,024,011 participants) for extremely PTB (Supplementary Table 5).
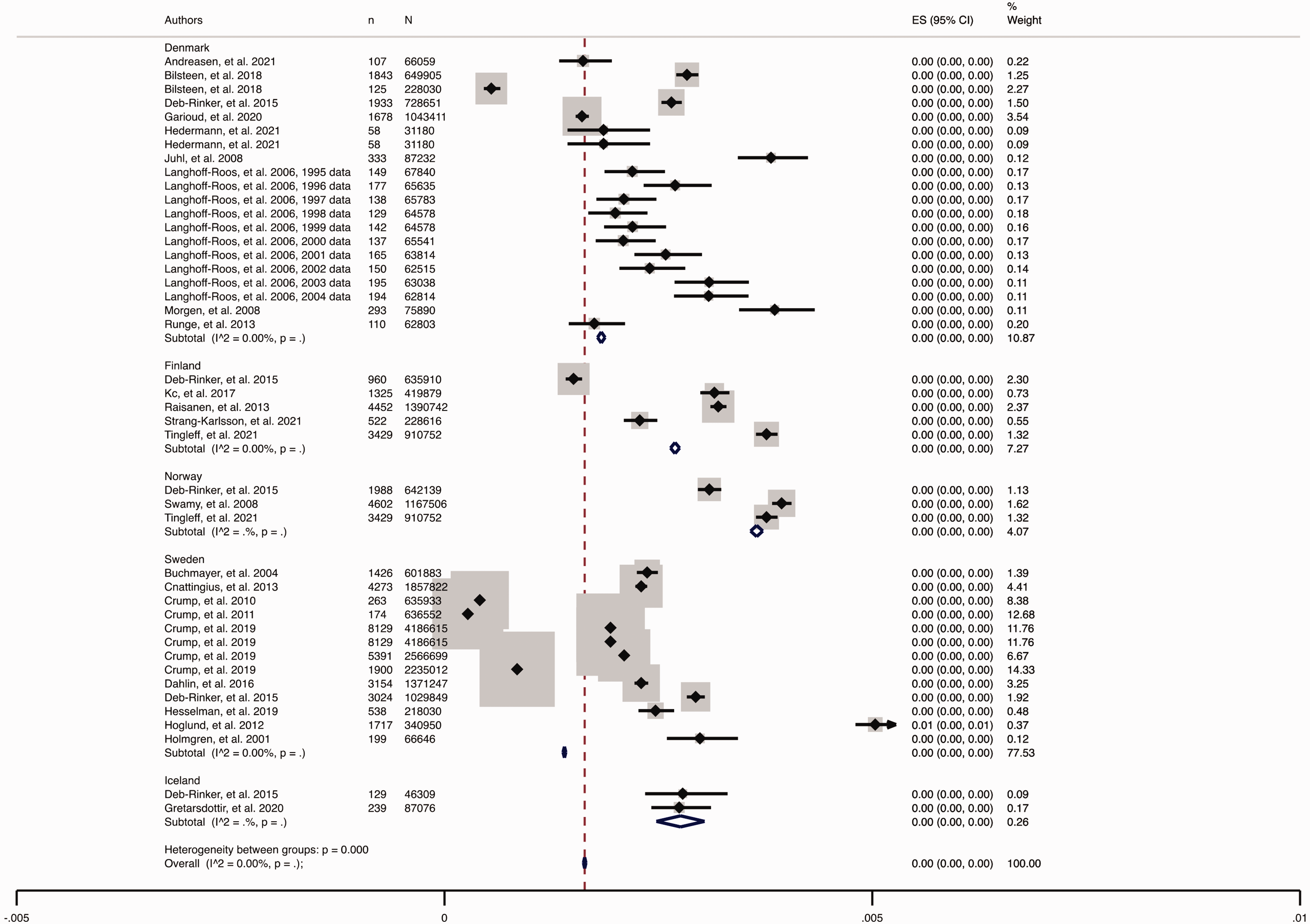
The results of the PP of PTB and its categories in each Scandinavian country are presented in Figures 2–6. The highest prevalence of PTB was observed in Norway (overall PP = 6.2%, 95% CI 5.3%, 7.0%), followed by Sweden (overall PP = 5.3%, 95% CI 5.1%, 5.4%), Denmark (overall PP = 5.2%, 95% CI 4.9%, 5.3%), and Iceland (overall PP = 5.0%, 95% CI 4.4%, 5.7%). The lowest prevalence was observed in Finland (overall PP = 4.9%, 95% CI 4.7%, 5.1%; Figures 2 and 3).

The prevalence of preterm birth (PTB) and its categories in Scandinavian countries.

Forest plot of pooled prevalence of preterm birth in each Scandinavian country (a. Norway, b. Sweden, c. Finland, d. Denmark, and e. Iceland).

Forest plot of pooled prevalence of moderate/late preterm birth in each Scandinavian country.

Forest plot of pooled prevalence of very preterm birth in each Scandinavian country.
Forest plot of pooled prevalence of extremely preterm birth in each Scandinavian country.
A subgroup analysis was performed by PTB category across the Scandinavian countries (Figures 4–6). The same approximate trend was observed in the prevalence of the PTB categories in these countries. The pooled estimates of moderate/late PTB were 4.9% (95% CI 4.6%, 5.2%) in Norway, 4.6% (95% CI 4.4%, 4.9%) in Sweden, 4.6% (95% CI 4.2%, 4.9%) in Denmark, 4.5% (95% CI 4.3%, 4.7%) in Iceland, and 4.1% (95% CI 3.7%, 4.3%) in Finland (Figure 4). The highest very PTB (0.9%, 95% CI 0.6%, 1.2%) and extremely PTB (0.4%, 95% CI 0.3%, 0.4%) prevalences were reported in Norway (Figures 5 and 6).
The publication bias results are presented in Figure 7 and Supplementary Table 5. The results of Begg’s test indicated no substantial publication bias among various outcomes (all P > 0.05). The funnel plot showed some scatter for the moderate/late PTB outcome that may have been caused by outliers; however, the results remained unchanged after correction using the trim and fill method (4.2%, 95% CI 4.0, 4.4). The scatter observed in the other funnel plot may have been caused by the observed heterogeneity of the included studies, fitting with the assumptions of the random‐effects model. Therefore, no evidence suggested that the analysis was affected by publication bias.

Funnel plot for the assessment of publication bias: a. Total preterm birth, b. Moderate/late preterm birth, c. Very preterm birth, and d. Extremely preterm birth.
The heterogeneity results indicated substantial heterogeneity between populations; most of the heterogeneity may be attributable to maternal age, body mass index, or ethnicity. Nevertheless, sensitivity analysis showed that no single study fundamentally changed the PP of any outcome (Supplementary Figure 1).
Discussion
This systematic review and meta-analysis of population-based studies provided data on the prevalence of PTB and its categories in Scandinavian countries. The overall PP of PTB in these countries was 5.3%, with small variations between countries that ranged from 4.9% to 6.2%. The highest and lowest PPs of PTB were observed in Norway and Finland, respectively.
Scandinavian countries have a strong tradition of collaboration and share features of policy and welfare systems and social security including free education at all levels, a social safety network for people with reduced health and work capacities, and a universal and predominantly publicly financed healthcare system. 126 In general, these countries are highly ranked on a range of sociodemographic and health-relevant measures such as the United Nations Human Development Indices and indicators, and gender equality, educational attainment, and labor force participation measures. 126
The issue of PTB is one of the major growing global health concerns. The United Nations Sustainable Development Goals aim to end all preventable deaths of newborns and children aged under 5 years by 2030. 127
The overall PTB rate was lower in the Scandinavian countries than in the global population, with the lowest rate in the Finnish population. Although the worldwide prevalence of PTB is unknown due to the lack of data in many countries, the estimated prevalence of PTB in 184 lower-income countries based on 2010 data indicated a PTB of 11%. 128 Additionally, major variations in PTB rates are observed by geographic region and income level. 10 Nearly 90% of all PTBs are reported to occur in low- and middle-income countries, particularly in sub-Saharan Africa. 1
Nevertheless, Scandinavian countries provide access to quality healthcare—particularly prenatal care—which leads to the improvement of maternal and neonatal outcomes and the prevention of premature mortality. 129 Moreover, it has been well documented that maternal omega-3 consumption during pregnancy, which is common in these countries, can significantly decrease the risk of PTB. 130
Although the general prevalence of PTB in Scandinavian countries is low, some variations exist across countries. For example, according to our review, Norway and Finland have the highest and lowest prevalence rates of PTB. Even though the Scandinavians share common characteristics that build on fundamental ideas of equality related to health care access, gender, and social services, notable differences exist between the countries concerning history, societal development, immigration population, culture, and lifestyle, which may affect the risk of PTB.8,126,131 These differences may also be responsible for variations in the rate of PTB among the countries.
This meta-analysis further provided details of PTB categories based on the gestational age subgroups. These details allow the identification of high-risk populations and the development and implementation of prevention strategies. In addition, PTB classification facilitates the surveillance of PTBs and allows standardized local and international data comparisons. According to our review, among all live births, the rate of moderate/late preterm births—the common form of PTB in Scandinavian countries—ranged from 4.1% to 4.9%. Only roughly 0.2% fall into the extremely PTB category and the other 0.6% were born at 28 to < 32 weeks of gestation. Our findings are supported by the common notion of PTB found in the international literature. 132
Notably, the etiopathogenesis of PTB is multifactorial and characterized by various clinical presentations. Women with singleton pregnancies without a history of a previous PTB have a low risk of PTB. However, previous PTB, a short cervix, or multiple gestation increase the risk of PTB. A recent study defined a generalized method for developing an evidence-based holistic risk assessment for PTB based on relevant and essential factors including maternal history and cervical length ultrasound measurement by the use of a machine learning statistical approach for use in clinical practice. 133 This screening approach can contribute to the worldwide reduction of the prevalence of PTB.
In summary, this study expands on previous single studies in Scandinavian countries by including the prevalence of PTB and its categories. Our review results are based on population-based data that were extracted from high-quality data registries, thus ensuring the coverage of all available literature. The standardized study selection and data extraction processes that employed narrow inclusion criteria led to the inclusion of high-quality papers, ensured the validity and reliability of the review results and meta-analysis, and added valuable information to the current international knowledge of PTB.
The main limitation of this review may be the lack of data about potential risk factors in the included studies, which are needed to improve our knowledge of PTB. We were unable to perform subgroup analyses based on the core outcomes of PTB because of the lack of data in the included studies. 134 In addition, the studies generally did not exclude twin or multiple pregnancies in their reports; therefore, the population prevalence of late PTB may have been impacted by the multiple birth rates. 3 However, given that multiple pregnancies constitute approximately 3% of births,135,136 multiple births may not have confounded our review results. Although gray literature may be an important source of data on PTBs, this type of literature was excluded from the review because it was not peer-reviewed. The lack of methodological details and accurate data on research variables in the gray literature hinders the quality appraisal of this literature.
Conclusion
The overall PP of PTB in Scandinavian countries was 5.3%, with small variations between countries ranging from 4.9% to 6.2%. The highest and lowest PP rates of PTB in this group of countries were observed in Norway and Finland, respectively. Moderate/late PTB, which occurred between 32 to <37 weeks of gestation, was the most common category of PTB and represented 4.5% of all live births. The review findings reflect the burden of diseases on certain populations and can support policymakers who are responsible for the allocation of resources in identifying healthcare priorities and developing preventive strategies.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231203843 - Supplemental material for Prevalence of preterm birth in Scandinavian countries: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231203843 for Prevalence of preterm birth in Scandinavian countries: a systematic review and meta-analysis by Samira Behboudi-Gandevani, Razieh Bidhendi-Yarandi, Mohammad Hossein Panahi, Abbas Mardani, Christina Prinds, Mojtaba Vaismoradi and Manela Glarcher in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231203843 - Supplemental material for Prevalence of preterm birth in Scandinavian countries: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605231203843 for Prevalence of preterm birth in Scandinavian countries: a systematic review and meta-analysis by Samira Behboudi-Gandevani, Razieh Bidhendi-Yarandi, Mohammad Hossein Panahi, Abbas Mardani, Christina Prinds, Mojtaba Vaismoradi and Manela Glarcher in Journal of International Medical Research
Footnotes
Data availability statement
Access to the raw data is possible upon reasonable request to the corresponding author.
Declaration of conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
Nord University, Bodø, Norway funded the publishing costs of this article. This research received no other grants from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.