
Abstract
Objective:
A short cervix during pregnancy indicates a higher risk of preterm delivery. Transvaginal sonography is widely used for the detection of a short cervix. The literature indicates that 21–24 weeks is the most sensitive gestational age to assess transvaginal cervical length (TV CL) of ≤2.5 cm for potential preterm delivery. Pregnancies between 18 and 20 weeks’ gestation are generally performed transabdominally; thus, it could be beneficial to have a recognized correlation between the transabdominal cervical length (TA CL) measurement and the TV CL measurement at this earlier time period.
Materials and Methods:
An online database search produced 13 research articles to be reviewed. Inclusion criteria consisted of TA CL and TV CL assessment of singleton pregnancies with intact membranes.
Results:
Findings indicate high diagnostic yield when a TA CL of <2.9 cm or TV CL of <2.5 cm is used for defining a shortened cervix when measured between 18 and 20 weeks’ gestation.
Conclusion:
This review of the literature indicates a correlation between average TA CL and average TV CL measurements, although the relationship widens as CLs become shorter.
Preterm birth (PTB) or premature birth is delivery of a baby before 37 weeks’ gestation. PTB has a worldwide incidence of 15 million annually and accounts for 10% of pregnancies in the United States.1–3 Premature infants are at greater risk of developing respiratory distress, cerebral palsy, intracranial hemorrhage, and other neuropathologies.4,5 The cervical length (CL) measurement is significant since a CL of <2.5 cm during pregnancy has a strong correlation in predicting PTB.4,6,7 A CL screening by transvaginal (TV) sonography between 16 and 24 weeks’ gestation is recommended to identify women at risk of PTB.8,9 Research indicates there is improved outcomes when women at low risk and high risk of PTB participate in TV CL screening programs during their mid-second trimester when routine fetal and maternal pelvic anatomy is imaged.10–13
These mid-trimester sonograms are customarily performed using the transabdominal (TA) approach. Acceptance of the TA method for screening includes opportunity for strategic CL assessment. A review of the literature regarding the comparability between transabdominal cervical length (TA CL) and transvaginal cervical length (TV CL), in the mid-second trimester, helps to identify trends regarding TV and TA sonographic assessment of the CL. The aim was to compare TA CL and TV CL measurements to determine whether TA CL is comparable to TV CL as an initial screening method, during the specific gestational ages (GAs;18–20 weeks) for CL during this window of routine imaging.
Materials and Methods
An online database search was performed using PubMed, Google Scholar, Elsevier, and Wiley Online Library from 2001 to 2019. Key words searched were sonography, cervical length, short cervix, transabdominal, transvaginal, preterm delivery, and preterm birth. A total of 29 articles were reviewed, and 13 full-text original research articles were selected for inclusion in this literature review. Inclusion criteria consisted of original research articles discussing TA CL and/or TV CL assessment for singleton pregnancies with intact membranes.
Cervical Incompetency
During pregnancy, the cervix is responsible for maintaining an intact fetal environment and should remain competent until term. Cervical incompetence is a progressive pathology that results in shortening of the CL (Figure 1). Cervical remodeling, which involves the breakdown of the structural collagen fibers, is a process that allows the cervix to soften to permit delivery. If cervical softening or cervical effacement occurs too early in gestation, PTB is a risk. 14 The etiology of cervical incompetence may result from consequences of inflammation, premature contractions, uterine overdistention, previous pelvic surgeries, prior preterm delivery, or congenital causes. 15 Congenital cervical incompetence may be from exposure to diethylstilbestrol (DES) or Müllerian duct abnormalities.15,16
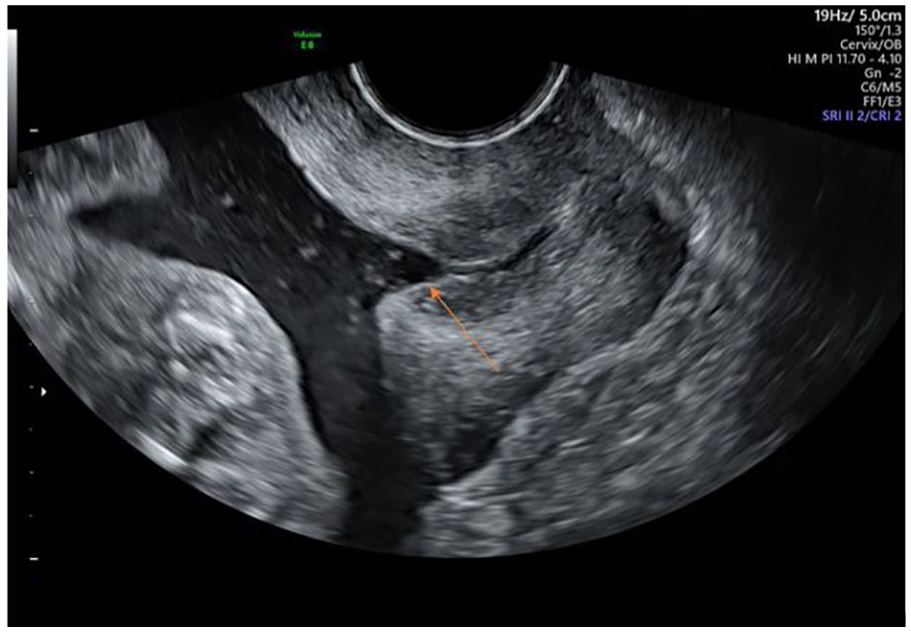
Transvaginal image demonstrating a “Y”-shaped incompetent cervix. An arrow points to the top of the “Y.”
Sonographic Features of the Cervix
The normal sonographic appearance of the cervical wall is a low-level gray echogenicity with a homogeneous smooth echo texture. The cervical canal is the hyperechoic line that equally divides the anterior cervical wall and the posterior cervical wall. The CL is measured in the sagittal plane extending from the internal os to the external os.17,18 The vaginal wall is more visible by the rounded protrusions of the cervix into the vagina. It is important to not mistake the vaginal wall as a boundary for the external os. During pregnancy, it is normal for a small amount of cervical mucus to be visualized, which may appear anechoic to hypoechoic within the cervical canal (Figure 2). 19 Optimally, the cervix should take up two-thirds of the image for proper assessment of the cervix and for visualization of the cervical mucosa.9,17
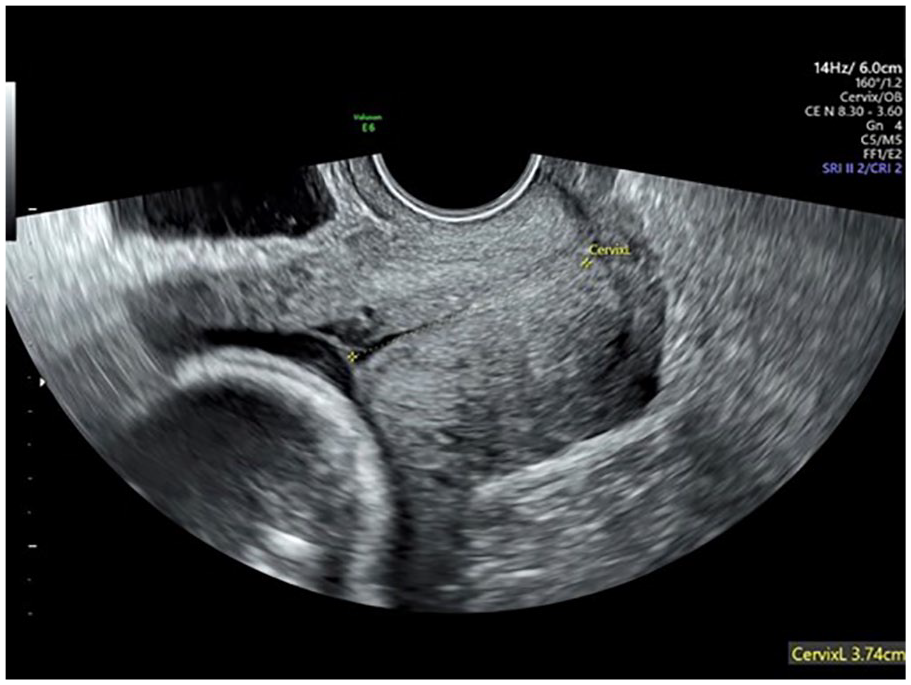
Anechoic mucus near the internal os is demonstrated in this transvaginal image with cervical length measured.
When cervical funneling of the internal os is present, calipers are placed at the apex of the funnel to the external os. 17 Sludge may accompany a funneling cervix, which appears as a conglomeration of echogenic material within the apex of the funnel, and in non-funneling cervices, the sludge may also accumulate near the internal os (Figure 3).6,17 A higher risk of preterm delivery has been noted with a short CL and the presence of sludge. 6 At least three measurements should be obtained, and the shortest, technically best measurement should be used for clinical management. 6 The normal CL measures greater than 2.5–3.0 cm.6,19

Sludge accumulating near the cervical internal os is demonstrated.
TA CL technique
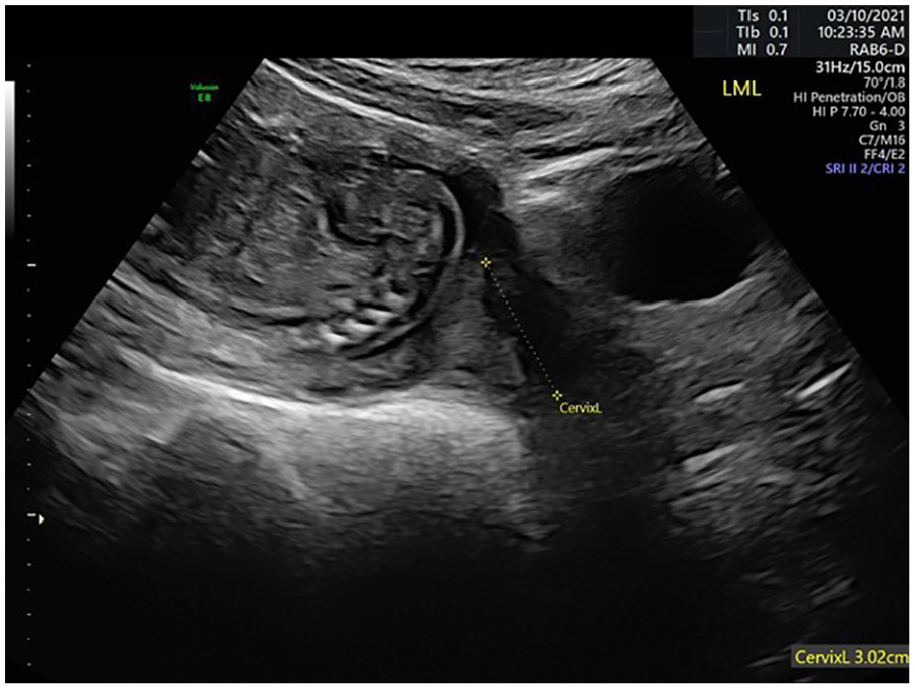
The TA approach uses a curvilinear transducer with a typical frequency range of 2–5 MHz. A major TA landmark is the bladder, which provides an acoustic window for imaging, but an excessively distended bladder may falsely lengthen the cervix.18,20 When scanning, it may be helpful to tilt the patient into a Trendelenburg position, to shift the weight of the baby from the cervix or to aid in visualization. There are two methods for obtaining a TA CL: a prevoid technique or a postvoid technique. When using the postvoid technique, the transducer can be moved superiorly and then angled inferiorly to allow the amniotic fluid to serve as an acoustic window. It may be more common to visualize a curved cervical canal when using the postvoid method (Figure 4). 18
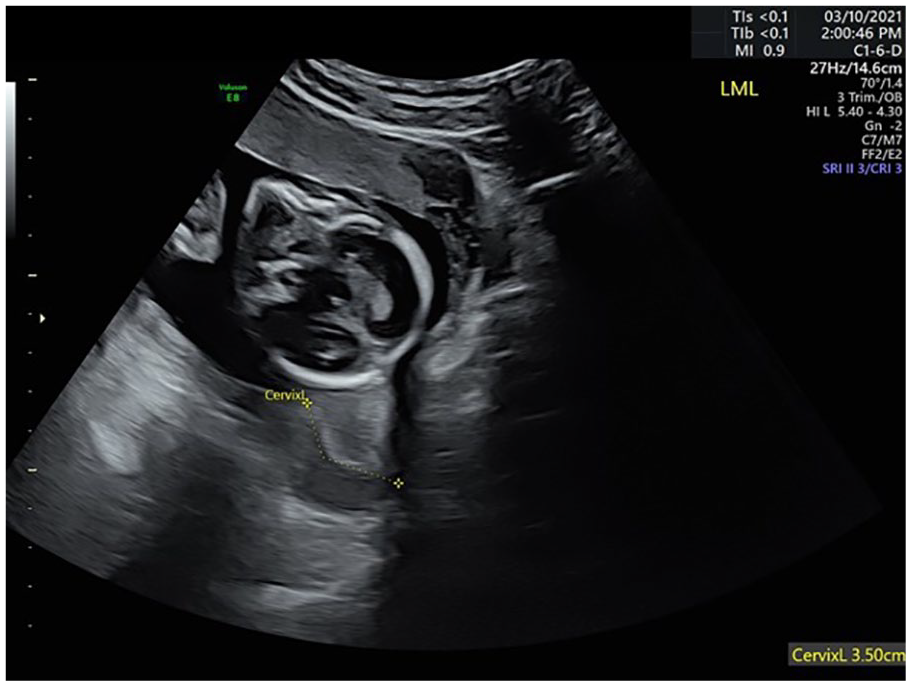
A postvoid transabdominal cervical length image demonstrating a curved cervical canal.
TV CL technique
The TV approach uses frequency ranges from 5 to 7.5 MHz, which provides a higher resolution for clearer assessment (Figure 2). Excessive pressure applied by the transducer may cause artifactual lengthening; thus, care should be taken when acquiring the measurement. 18 To verify appropriate pressure, the transducer can be inserted until the cervix is seen, then withdrawn until the image slightly blurs, and then moved toward the cervix just enough to visualize the cervix clearly. 9 As part of an assessment for cervical shortening, the sonographer can use their hand to apply pelvic pressure to the lower uterine segment while imaging the cervix and remeasuring the length, noting “slight pressure” on the annotation.17,21 This applied pressure may stimulate how the cervix reacts to pressure when the patient stands.
Comparing TA to TV Method for CL in Mid-second Trimester
Cho et al 22 compared TA CL and TV CL measurements to identify women who needed a TV sonogram for best outcome. Women between 20 and 29 weeks were included regardless of being at high or low risk. 22 The TA CL measurement was obtained in 81% of the cases. 22 When the CL could not be measured, it was due to poor visualization of the internal and external os from the TA approach. TA and TV measurements for the average CL were not significantly different. The average TA CL was 3.78 cm, while the average TV CL was 3.82 cm. 22 With a short cervix threshold of <2 cm, TA CL produced a sensitivity of 100% and a specificity of 99.67%. 22 When the threshold was raised to ≤2.5 cm, the correlation produced a sensitivity of 75% and a specificity of 99%. 22
Friedman et al 23 theorized that unless the short CL was at a low threshold, it would be unlikely that an additional TV measurement would add value. Both prevoid and postvoid techniques were used to take TA CL measurements for women between 18 and 23 weeks. 23 The TA screening was 100% sensitive when compared to a TV CL of ≤2 cm and 95% sensitive when the TV CL of ≤2.5 cm was used. 23 Using a TA CL threshold of >3.5 cm resulted in 40% of the patients not requiring a TV sonogram. 23 Images were unobtainable in 6% of patients prevoid and 18% of patients postvoid. 23
Nambiar et al 24 assessed the CL between 18 and 20 weeks’ gestation in participants who agreed to undergo both TA and TV sonograms. The TA CL measurement was obtained with participants’ bladders half full. A short CL was defined as <2.5 cm by TV. 24 The average TA CL between 18 and 20 weeks for term pregnancies was 3.46 cm, while the average TA CL for preterm pregnancies was 2.58 cm. 24 The average TV CL for term pregnancies was 3.15 cm and the average TV CL for preterm pregnancies was 2.1 cm. 24 A receiver operating characteristic curve estimated that a TA CL of ≤2.9 cm would predict a short TV CL of ≤2.5 cm. 24 The ≤2.9 cm threshold for TA CL produced a sensitivity of 100% and specificity of 92%. 24
Rhoades et al 8 assessed CL between 17 and 23 weeks’ gestation. TA CL measurements were obtained with an empty bladder and were unmeasurable in 21% of the cases due to poor visualization of the internal and external os. 8 The average TA CL was 3.85 cm and the average TV CL was 4.23 cm. 8 When comparing a TA CL threshold of <3.5 cm to a TV CL threshold of <3.0 cm, a sensitivity of 93% and a specificity of 70% were found. 8 This correlation produced a 95% confidence interval for the TA measurement to predict a short cervix. 8
Discussion
A validated dominant trend is the declining rate of preterm delivery when women enroll in a CL screening program.10,11,25 Screening programs using the TV CL threshold of ≤2.5 cm predicted preterm delivery.10,11 Table 1 shows participants in TV CL screening programs who consistently had lower occurrences of preterm delivery when compared to nonscreened participants.
Selected Published Transvaginal Short Cervical Length Demographics.
Abbreviations: CL, cervical length; GA, gestational age; PTB, Preterm birth; TV, transvaginal.
When evaluating women at risk of preterm delivery, a TV CL threshold of 2.5 cm was found to have a sensitivity rate as high as 100%. 13 When the threshold was raised, the sensitivity decreased. 12 In comparison, data support that having a TV CL of ≤2.5 cm in the mid-trimester may be a contributing factor to improved sensitivity (Tables 2 and 3).8,12,13,22,23,24,26 When assessing TA CL, it appears that keeping the threshold between 2.5 and 3.0 cm provides comparable sensitivities to TV with rates ranging from 92% to 100%.8,22,23,24 The average TA CL measurements were consistently shorter than the average TV CL measurements, which may be due to the difficulty in visualizing key landmarks such as the internal or external os (Table 3). When the TA CL threshold was changed from <2.0 cm and ≤2.5 cm, sensitivities decreased, respectively. 22 When the short cervix thresholds were raised, the specificities lowered, requiring more follow-up TV sonograms to verify accurate CL even when the sensitivities remained high. 23
Selected Published Diagnostic Yields for TV CL and a Threshold for High-Risk Women.
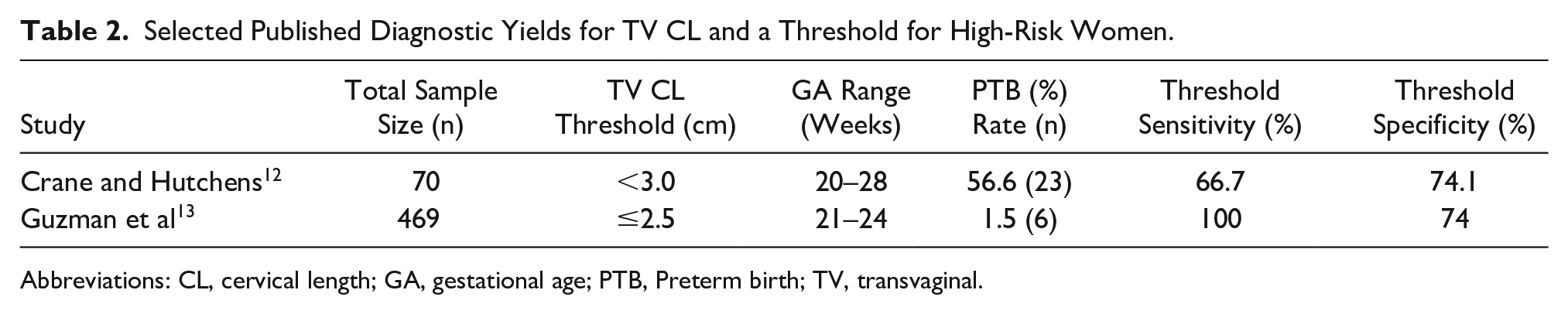
Abbreviations: CL, cervical length; GA, gestational age; PTB, Preterm birth; TV, transvaginal.
Selected Published Results of Transabdominal and Transvaginal Measures for Comparisons.
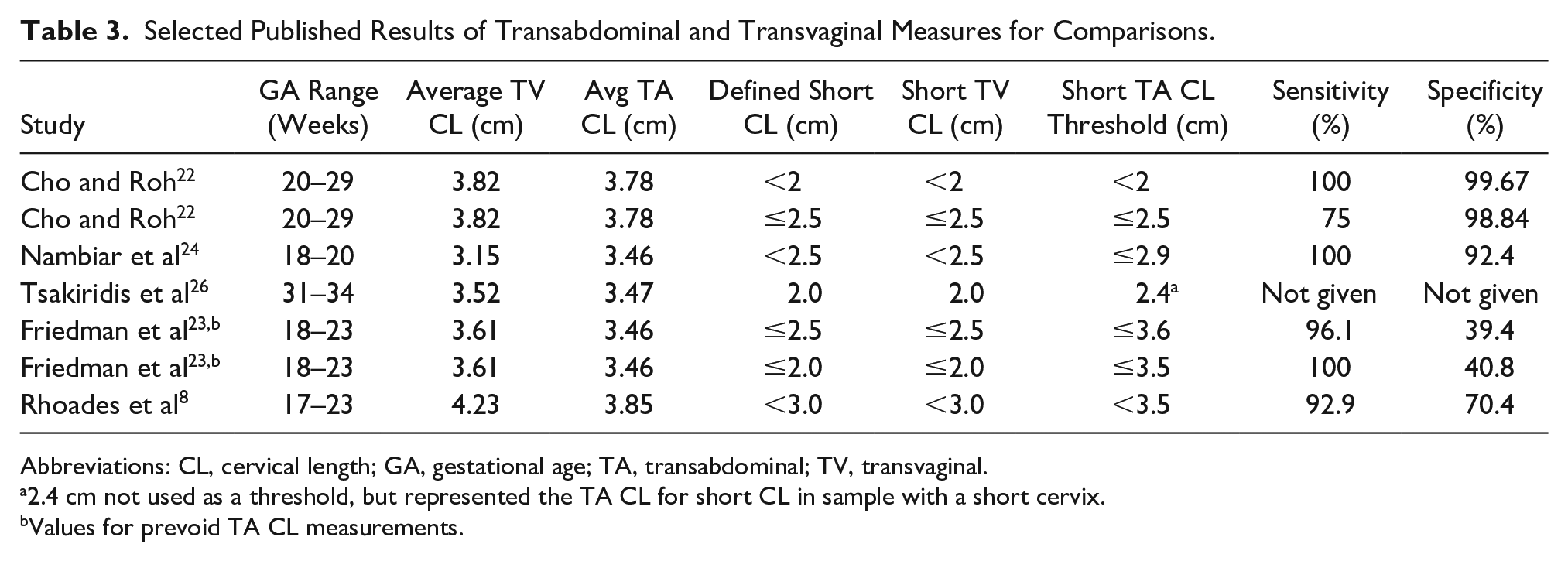
Abbreviations: CL, cervical length; GA, gestational age; TA, transabdominal; TV, transvaginal.
2.4 cm not used as a threshold, but represented the TA CL for short CL in sample with a short cervix.
Values for prevoid TA CL measurements.
In general, the average TV CL measurements are shorter than the average TA CL measurements. When compared, the TA CL was 0.04–0.43 mm different than the measured TV CL (Table 3).8,22,23,26 The TA ultrasound indicates that it underestimates CL, which may actually be better for identifying a short CL as a first-line screening method. Another observation is that as the cervix shortens, the difference between the two techniques becomes greater and more significant. When the cervix is short, the TA CL measures longer than the TV CL measurements. This difference highlights the accuracy of TV CL when measuring a short cervix.
When imaging transabdominally, the question of a prevoid verses postvoid bladder often arises. In the research reviewed, there were discrepancies between the average prevoid TA CL measurements and the average postvoid TA CL measurements. 23 Therefore, the results in context of bladder status indicates that additional research focusing specifically on comparing prevoid and postvoid bladder status of the TA CL measurements should be performed.
An important point to note is that the cervix is not always well visualized in the TA approach (Figure 5). Cho et al 22 could only measure the CL in 81% of mid-second trimester gestations, needing the additional TV scan for proper assessment. When the GA is increased, proper visualization becomes of greater concern. Additional assessment between late GA and mid-second trimester GA should be performed.
Transabdominal image demonstrating an ill-defined cervical internal os and external os due to shadowing.
Conclusion
A short CL is a recognized factor in predicting preterm delivery. TV sonography is used to predict preterm delivery with high accuracy in the mid-second trimester using a threshold of ≤2.5 cm but is not routinely used during obstetric sonograms performed between 18 and 22 weeks. A comparison of the research shows that TA CL is a sufficient approach as an initial screening for identification of a short cervix during pregnancy when a threshold of ≤2.9 cm is used. 24 If a cervix measures ≤2.9 cm or is not well visualized, then a TV CL should be performed. Any time a cervix is not clearly visualized, then a follow-up TV CL should be obtained to measure the accurate CL.
Footnotes
Peer Reviewer Guarantee Statement
The Editor/Associate Editor of JDMS is an author of this paper; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor/Board member had no involvement in the decision-making process.
Ethics Approval
Ethical approval was not sought for the present study. This is a literature review so ethics approval was not needed.
Informed Consent
Informed consent was not sought for the present study. This is a literature review so informed consent was not needed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.