
Abstract
Thyroid cancer is the common malignancy of the endocrine system. Thyroid neoplasms are usually asymptomatic and slow growing. Uncommonly, aggressive thyroid neoplasms may invade adjacent blood vessels. Internal jugular vein invasion is a rare complication of an aggressive thyroid malignancy. Careful sonographic examination of a thrombus-like structure inside a blood vessel adjacent to the affected thyroid could reveal that the “thrombus” is part of the thyroid mass. The continuity of a thyroid neoplasm into the vascular lumen and inner-“thrombus” vascularity confirms the cancerous invasion. Ultrasound-guided fine-needle aspiration biopsy is standard for differentiating benign versus malignant thyroid nodules. Genetic testing of thyroid nodules provides valuable clinical information in addition to the routine cytological analysis.
Keywords
Thyroid cancer is the most common malignancy of the endocrine system, of which papillary is the most prevalent, comprising up to 90% of all thyroid malignancies. 1 Typically, asymptomatic, thyroid cancer is detected as a nodule during physical examinations (if sizeable enough) and confirmed by sonographic examination with a subsequent ultrasound-guided fine-needle aspiration biopsy (US-G-FNA bx). Thyroid Imaging Reporting and Data Systems (TI-RADS) assess thyroid nodules for their malignancy risk and decide whether the US-G-FNA is indicated. Thyroid Imaging Reporting and Data Systems analyze different characteristics of thyroid nodules and assign points for each of the five parameters:
Composition (Cystic = 0 Points, Mixed Cystic/Solid = 1 Point, Solid = 2 Points).
Echogenicity (Anechoic = 0 Points, Iso- or Hyperechoic = 1 Point, Hypoechoic = 2 Points, Very Hypoechoic = 3 Points).
Shape (Wider-than-Tall = 0 Points, Taller-than-Wide = 3 Points).
Margin (Smooth or Ill-defined = 0 Points, Lobular or irregular = 2 Points, Extra-thyroidal extension = 3 Points).
Echogenic foci (None or large comet-tail-artifacts = 0 Points, Macrocalcifications = 1 Point, Peripheral rim calcifications = 2 Points, Punctate echogenic foci = 3 Points).
The sum of all points classifies thyroid nodules from TR-1 (0 Points, benign—no biopsy needed) to TR-4 (4–6 Points, moderately suspicious for cancer—FNA bx is recommended if a nodule measures more than 1.5 cm in diameter) and TR-5 (7 Points or more, highly suspicious for cancer—FNA bx is recommended if a nodule measures more than 1 cm in diameter). 2
The final diagnosis of thyroid cancer is usually made when enough malignant cells is detected in a specimen collected during either FNA or core biopsy from a suspicious thyroid nodule. Modern molecular/genetic analysis of thyroid nodules helps to differentiate benign versus malignant neoplasms.
Case Report
A 56-year-old male was referred for thyroid sonography and, if recommended, US-G-FNA biopsy of the right thyroid mass that was detected by his primary care physician, during a routine physical exam. The patient had no family history of thyroid cancer. He reported no prior malignancies and no radiation exposure (i.e., radiation being one of the main risk factors for thyroid cancer). 1 The patient was examined with a Logiq Fortis ultrasound equipment system (GE HealthCare, Waukesha, Wisconsin) and a matrix linear array ML6-15 transducer. A sonographer, registered with the American Registry of Diagnostic Medical Sonography and 28 years of experience, performed the thyroid sonogram. The right thyroid nodule was detected and assessed with TI-RADS; it was solid (2 points), isoechoic (1 point), wider-than-tall (0 points), extending into the ipsilateral internal jugular vein (IJV) (3 points), without echogenic foci (0 points), and measured 4.3 × 3.2 × 3.6 cm. There was prominent internal vascularity of the thyroid mass that extended into the ipsilateral IJV. With six points, the lesion was classified as a TR-4 (moderately suspicious). Because it measured larger than 1.5 cm, the US-G-FNA bx was recommended (See Figures 1–5).
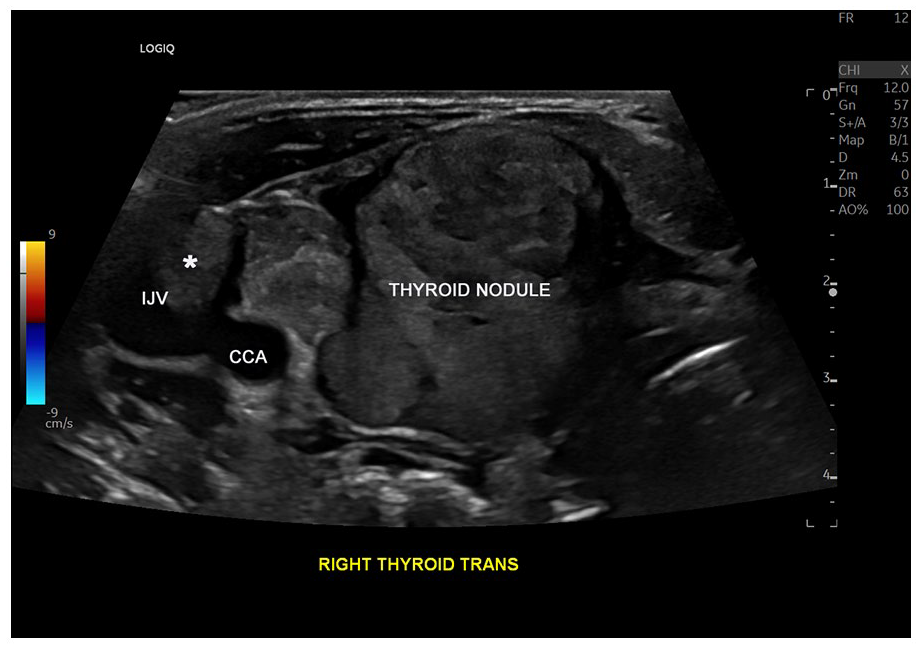
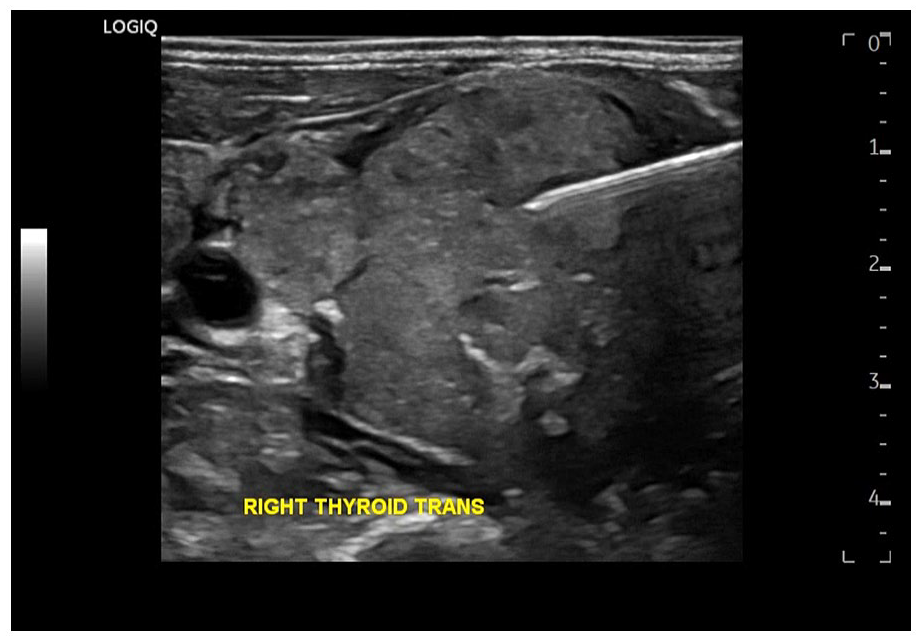
A grayscale transverse view of the right thyroid mass and adjacent ipsilateral internal jugular vein (IJV) and common carotid artery (CCA) demonstrated a tumor-thrombus, within the IJV (marked with asterisk symbol*).
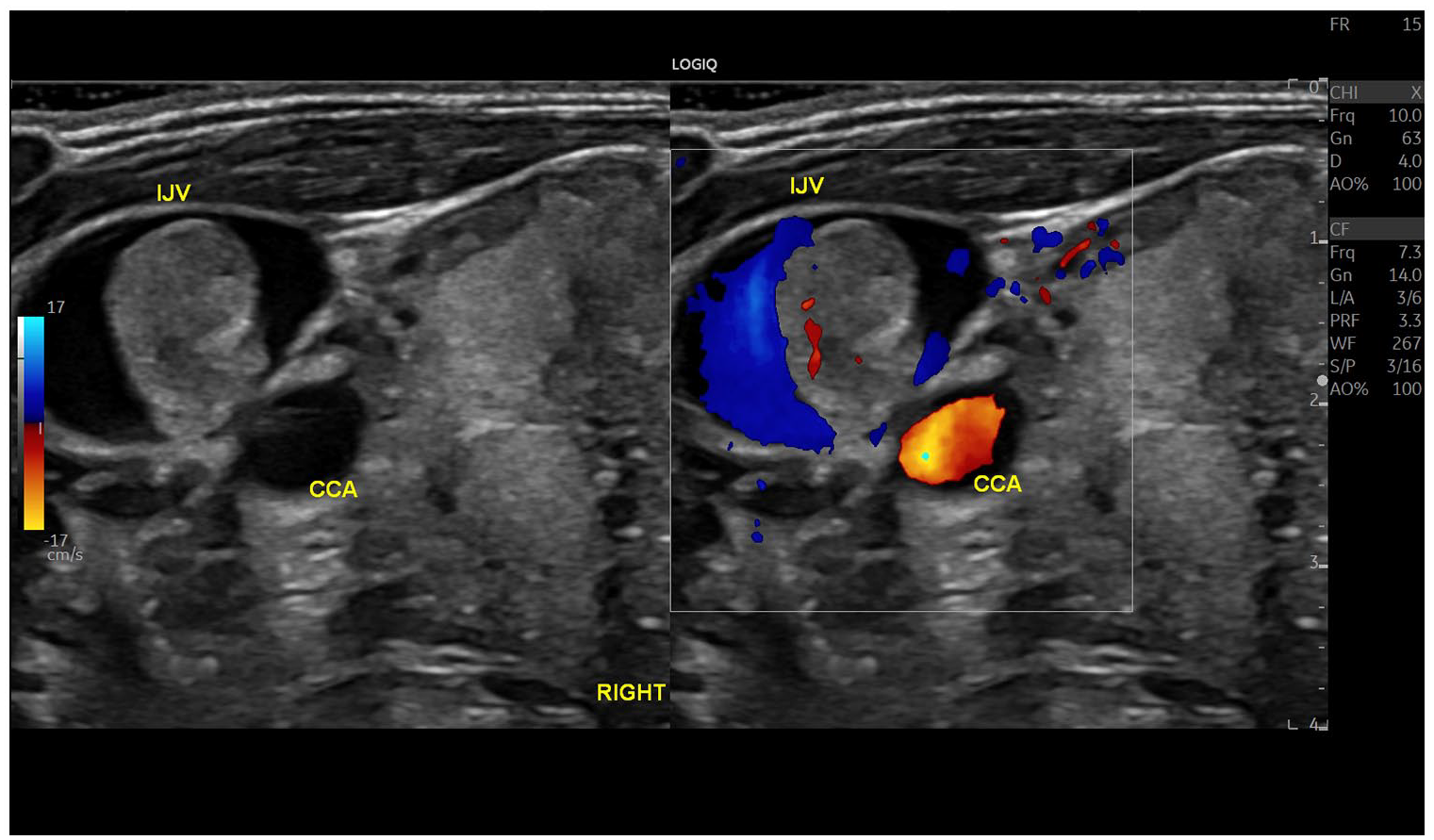
A dual-screen with both grayscale and color Doppler transverse views of the right thyroid mass are provided. These examples show the adjacent ipsilateral internal jugular vein (IJV) and common carotid artery (CCA) and a tumor-thrombus, with internal vascularity inside the IJV.
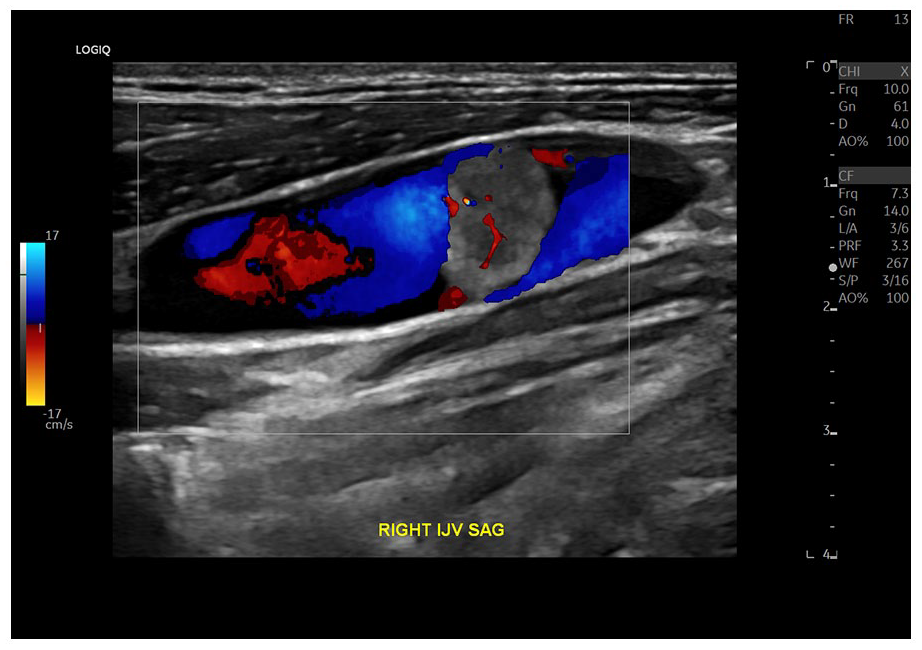
A color Doppler sagittal view is provided of a tumor-thrombus with internal vascularity inside the internal jugular vein (IJV).
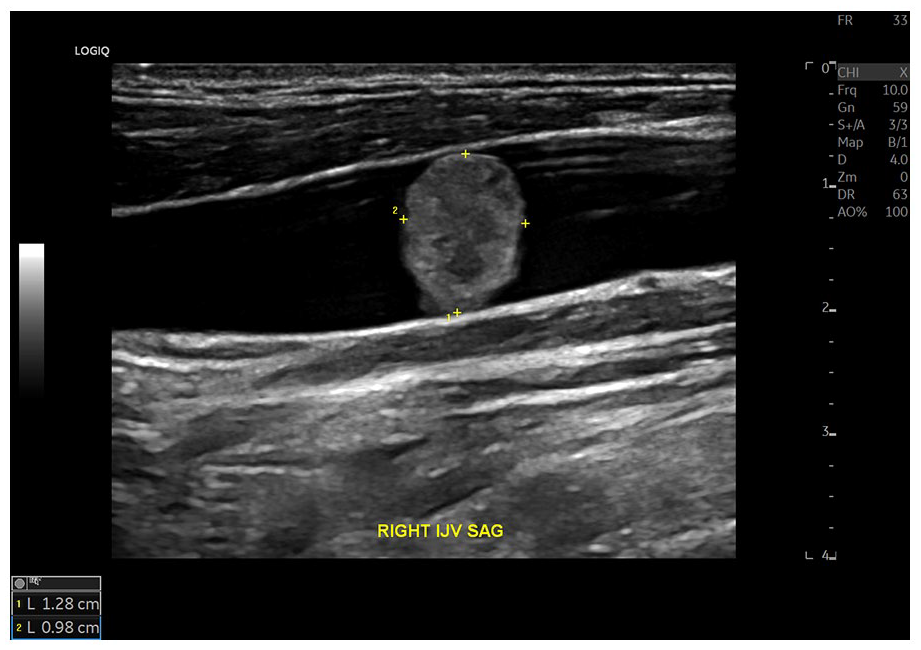
A grayscale sagittal view of a tumor-thrombus measuring 1.3 cm, inside the internal jugular vein (IJV).
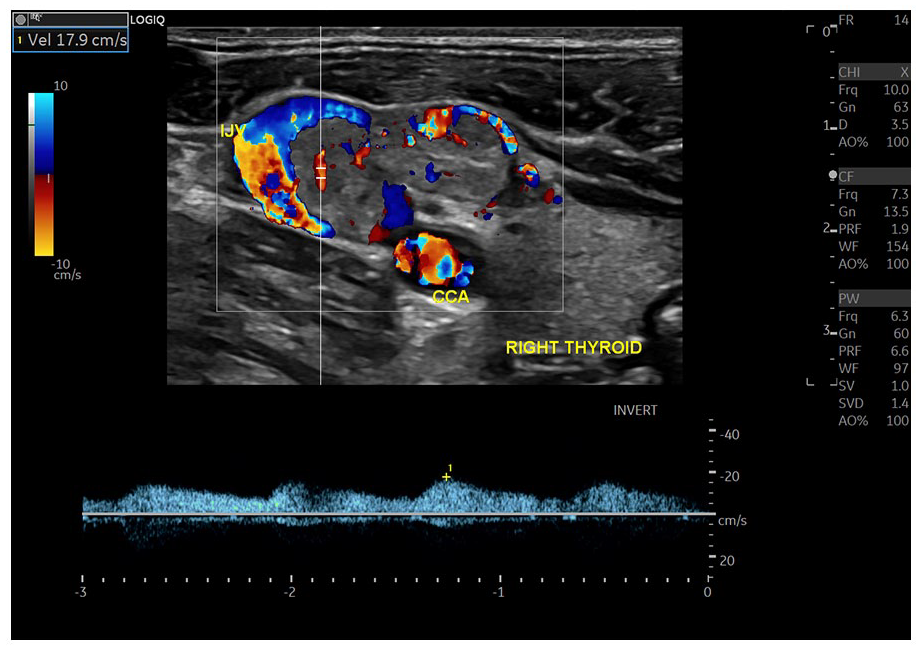
A color and spectral Doppler (oblique view) image demonstrated prominent blood flow inside the mass, invading the internal jugular vein (IJV).
The US-G-FNA biopsy was performed utilizing a free-hand technique (See Figure 6). Four samplings of the right thyroid lesion were obtained with the 23-gauge 1.5-inch needles, attached to the 3 mL syringes. The aspirated material from the two syringes was smeared on four glass slides and immersed into a container with 95% reagent alcohol. Two more aspirates were placed into a CytoLyt solution and a vial with molecular testing buffer, respectively. The collected specimens were sent to external medical laboratory for analysis (LabCorp, San Diego, California).
A grayscale image demonstrated that the 23-gauge biopsy needle (e.g., bright linear structure) inside the thyroid mass, during ultrasound-guided fine-needle aspiration biopsy.
The cytology report described the specimen as suspicious for papillary carcinoma (e.g., Bethesda category V). The molecular testing (ThyGeNext w/Rfx to ThyraMir) of the specimen utilizing ThyGeNext oncogene panel NCOA4-RET_4* revealed RET/PTC3 (NCOA4-RET) translocation mutation that corresponded to over 95% likelihood of malignancy.
Two weeks after the sonogram and US-G-FNA bx, computed tomography (CT) with contrast was performed to confirm the invasion of the IJV, using a Revolution Maxima 64-slice CT scanner (GE HealthCare). The patient was also injected with100 mL Omnipaque-350, for contrast enhancement (See Figures 7 and 8).
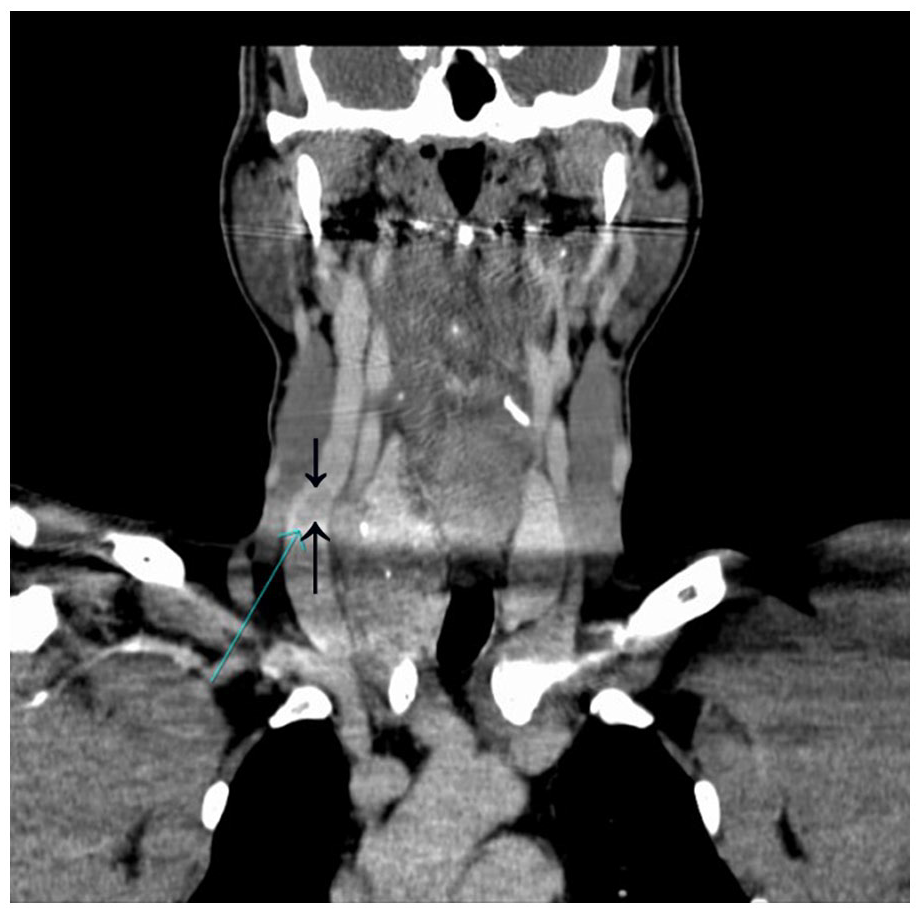
Coronal view of contrast-enhanced computed tomogram of the right internal jugular vein showing a tumor-thrombus (indicated by the arrows).
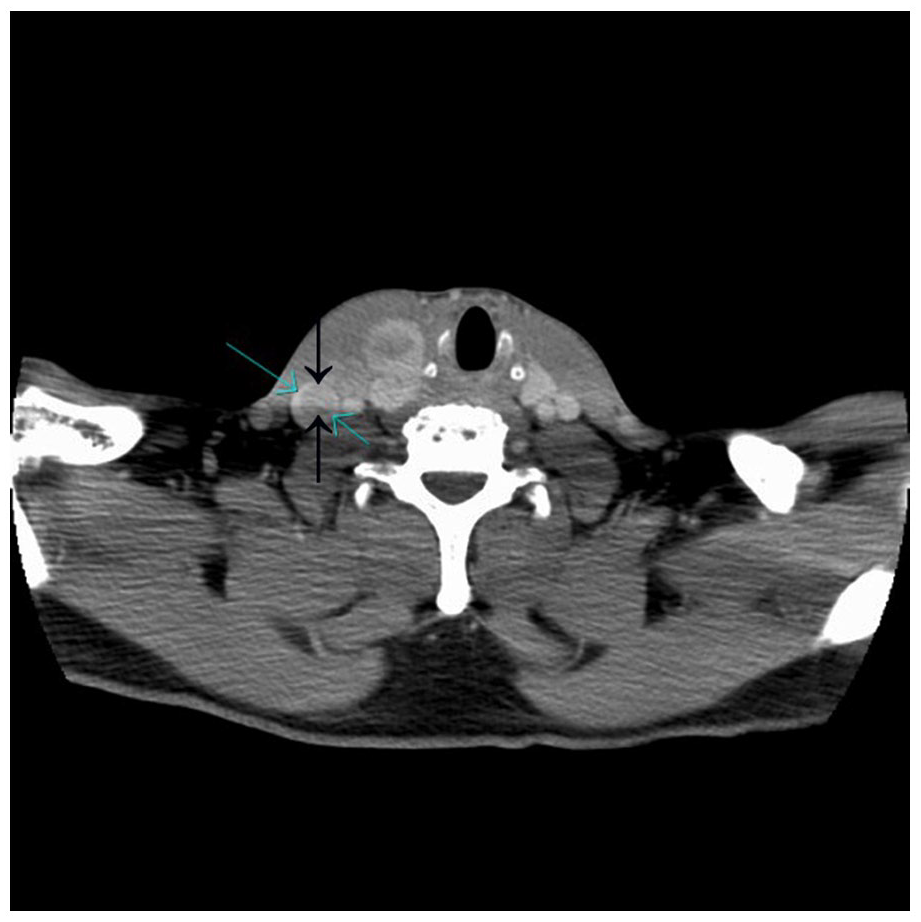
Axial view of contrast-enhanced computed tomogram of the right internal jugular vein showing a tumor-thrombus (indicated by the arrows).
After receiving a pathology report of the US-G-FNA bx and CT, the patient was scheduled for positron emission tomography (PET)-CT; however, he did not attend his appointment. This patient was lost to follow-up; therefore, no further information about his treatment and recovery was available. In a similar case published previously, the surgical treatment included total thyroidectomy with the removal of the infiltrated portion of the IJV (after its inferior and superior ligation). 3
Discussion
A literature search was conducted with the National Library of Medicine (Bethesda, Maryland), PubMed Central (PMC), and Google Scholar and were based on the following keywords: “locally invasive thyroid cancer,” “invasive thyroid neoplasm,” “thyroid sonography,” “thyroid fine-needle aspiration biopsy,” “molecular tumor testing,” “genetic tumor analysis,” and also a grouping of keywords for invasive thyroid neoplasm, thyroid malignancy, tumor invasion into blood vessels, thyroid ultrasound, thyroid biopsies, and molecular/genetic testing of thyroid tumors. The full-text articles were accessed on the corresponding journals’ websites or in local public libraries. Searches for the articles and manuscripts published before the 20th century were performed using Google Books (https://books.google.com/), utilizing the same exact keywords.
One of the main risk factors for thyroid cancer is ionizing radiation, which would include radiography and CT, especially in children. 1 Numerous cases of thyroid cancer related to childhood radiation exposure were well-documented after the Chornobyl accident when approximately Bq of 131I was released into the atmosphere. 4 The thyroid of the affected population received a dose 500 to 1000 times higher than the rest of the body, leading to approximately 4000 thyroid cancers. 4
During the previous decades, the individual radiation dose has doubled in the United States, from approximately 3 to 6 mSv/year, primarily because of medical radiation procedures. 5 Approximately one third of all CT examinations are performed in the head/neck region, radiating the thyroid, whereas iodinated contrast agents add more radiation saturation of the thyroid. 6
Thyroid cancer has been documented for hundreds of years. In the 18th century, it was reported that thyroid enlargement (known as a struma) could be cancerous, endangering a patient’s life by injuring (invading) the adjacent large veins, arteries, nerves, or trachea. 7 In 1824, a detailed description of thyroid cancer invasion of the adjacent IJV was published. 8 At that time and until the second half of the 20th century, no diagnostic imaging was available to assist physicians with detecting thyroid tumors. All clinical findings were made by physical examinations and confirmed either surgically or postmortem (during autopsies).
In 1962, the first diagnostic sonogram of the thyroid gland was performed in Japan. 9 The first successful biopsies of the thyroid, in 1930, were completed with a large (18-gauge, corresponding to an outer diameter of 1.27 mm) needle, which were “guided by palpation with the disengaged hand.” 10 Fine-needle (the gauge ≥22, corresponding to an outer diameter of ≤0.72 mm) aspiration (FNA) biopsy technique of the thyroid, without the imaging guidance, was developed in Europe in the 1950s and adopted in North America in the 1970s.11 –13
Sonographic guidance for various percutaneous needle biopsies has been used since the 1960s. 14 One of the first reports of thyroid FNA biopsies (using the 22- or 23-gauge needles) under ultrasound guidance was published in 1979. 15 At that time, sonography was mainly used to find a target nodule and determine the optimal depth and angle of the needles’ penetration. 14
The limited image resolution and slow processing power of older ultrasound equipment systems have not allowed for an effective real-time tracing of the biopsy needles, which is available today. With modern, real-time equipment systems, ultrasound-guided FNAs of thyroid nodules have become more efficient, accurate, and widely used.16,17
Clinical genetic testing of thyroid malignancies was developed in the 1980s with a discovery of the oncogene in a patient with papillary thyroid carcinoma (PTC). 18 Both internationally and in the United States, the incidence of thyroid cancer has increased significantly over the past decades. Currently, thyroid cancer ranks as the 13th most common malignancy in the United States overall and the most common in the endocrine system.1,19 Approximately 90% of all thyroid malignancies are PTC, 4% follicular thyroid carcinoma, 2% Hürthle cell carcinoma, 2% medullary thyroid carcinoma, 1% anaplastic thyroid carcinoma, and 1% other malignancies (including primary thyroid sarcomas and primary thyroid lymphomas).19 –23
Sonographically, PTC is typically hypoechoic, with internal microcalcifications, relatively well-defined margins, taller-than-wide, has internal hypervascularity, and affects cervical lymph nodes. Less commonly, it could be hyperechoic or isoechoic, with macro or peripheral calcifications, irregular margins, wider-than-tall, hypovascular, without cervical lymphadenopathy.24 –26
According to the current guidelines for thyroid cancer staging, the presented case corresponds to stage T4b (very advanced): “The cancer is any size and has grown extensively beyond the thyroid gland back toward the spine or into nearby large blood vessels.” 27
Thyroid cancers rarely produce macroscopic tumor-thrombi. There have been only a few dozen cases published in the English literature. Among those, the following affected sites were reported: the internal and external jugular veins, subclavian vein, brachiocephalic vein, axillary vein, superior vena cava, middle cerebral artery, pulmonary vein, pulmonary artery, and the heart.28 –43 There are two main pathways of a macro-thyroid cancer invasion into the IJV: direct IJV invasion, when the growing neoplasm destroys the venous wall, propagating into the venous lumen, and indirect invasion, when the tumor spreads into a small intra-thyroid vein, extending via the median thyroid vein into the IJV lumen, leaving the IJV wall intact. 28
Differentiated thyroid cancer (such as papillary carcinoma) has a worse prognosis in patients older than 55 years of age. 44 Moreover, older patients have a higher frequency of extra-thyroidal cancer extension and larger size of their primary tumors. 44
Not only thyroid cancers could invade adjacent blood vessels, causing tumor-thrombosis. The invasion of malignant neoplasms of the internal organs (hepatocellular carcinoma, renal cell carcinoma, pancreatic cancer, etc.) into the abdominal or pelvic vascular systems is very difficult to diagnose.45 –48
Extremely rarely, a blood vessel itself could develop primary cancer when a tumor originates in the vascular wall, filling the lumen and mimicking thrombosis or embolism. 45 Color and spectral Doppler, contrast-enhanced ultrasonography, fluorodeoxyglucose (FDG)-PET, T2-weighted magnetic resonance imaging (MRI) and angioscopy (direct visualization of the blood vessel’s lumen with the angioscope) are utilized to differentiate ordinary thrombi from tumor-thrombi.49 –52
In contrast to ordinary thrombi, tumor-thrombi represent the continuity of aggressive tumors into the adjacent blood vessels or cardiac chambers. In addition, tumor-thrombi are immobile, have internal vascularity, and could cause irregular expansion of the affected blood vessel. Whereas ordinary blood clots could be mobile, do not have internal vascularity, and do not cause irregular deformity of the affected vessels.49 –52
The presence of tumor-thrombus worsens the prognosis of patients with various types of cancer and significantly affects their treatment. 53 In patients with PTC, the extra-thyroidal spread (such as the invasion of the adjacent major blood vessels) is the most relevant prognostic risk factor for mortality: a specific tumor-related mortality of 38% in tumors with extra-thyroid spread and 0.65% in those without. 54 Another important parameter that worsens the prognosis, in those patients, is the size of the neoplasm larger than 4 cm. 54
Conclusion
Rarely, thyroid carcinomas invade major blood vessels. Therefore, sonographers and radiologists should always examine the thyroid gland and the adjacent anatomic structures, including the major arteries and veins.
The significant risk factors that worsen the prognosis of patients with papillary thyroid carcinoma include the extra-thyroidal extension of the tumor (including the invasion of the major cervical blood vessels), age older than 50–55 years, and the size of the tumor larger than 4 cm. Grayscale, color, and spectral Doppler sonography are among the diagnostic techniques that allow the differentiation of ordinary thrombi from tumor-thrombi.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because of the adherence to all regulatory and ethical rules of the host diagnostic center.
Informed Consent
Informed consent was not sought for the present study because all case images and data were de-identified and followed ethics committee or IRB guidelines (also referred as the Honest Broker System).