
Abstract
Papillary thyroid carcinoma is a differentiated thyroid cancer that arises from thyroid follicular epithelial cells. Sarcoidosis is a multisystem disease of unknown cause, characterized by monocytic infiltration and granuloma formation. We herein report a case of thyroid carcinoma complicated by sarcoidosis. When thyroid nodules and lymph node lesions are suspected, it is essential to avoid fixed thinking, conduct a comprehensive preoperative evaluation, and select the appropriate surgical approach. This can help reduce the likelihood of postoperative complications and improve the patient’s quality of life. Therefore, comprehensive diagnosis of the coexistence of papillary thyroid carcinoma and sarcoidosis is crucial.
Keywords
Introduction
Papillary thyroid carcinoma is a differentiated thyroid cancer that originates from thyroid follicular epithelial cells. Sarcoidosis is a multisystem disease of unknown cause, characterized by monocyte infiltration and granuloma formation. It can affect almost any organ, with the lymph nodes and lungs being the most commonly involved. Although few cases of the coexistence of papillary thyroid carcinoma and sarcoidosis have been reported, both conditions can involve the thyroid gland and lymph nodes. This overlap in clinical manifestations and imaging features poses a diagnostic challenge. 1
Case report
A woman in her early 50s was admitted to the hospital 1 week after discovering thyroid nodules. The patient had no symptoms such as hoarseness or coughing after drinking water, no medical history of neck radiation, and no family history of thyroid disease.
During the disease course, relevant examinations were completed. Color ultrasound of the neck revealed a hypoechoic area in the lower part of the left thyroid lobe measuring 0.9 × 1.29 cm and exhibiting an aspect ratio of >1, an unclear boundary, and multiple strong echoes inside (Figure 1). The inferior lobe of the right thyroid lobe appeared to have a first-order echo and exhibited a size of 0.75 × 0.47 cm, a clear boundary, and no strong focal echoes. Hypoechoic lymph nodes measuring 1.34 × 1.0 cm and showing poorly defined structure were seen in area IV of the right neck (Figure 2).

Color ultrasound of the neck showing a hypoechoic area in the lower part of the left thyroid lobe, measuring 0.9 × 1.29 cm and exhibiting an aspect ratio of >1, an unclear boundary, and multiple strong echoes inside.
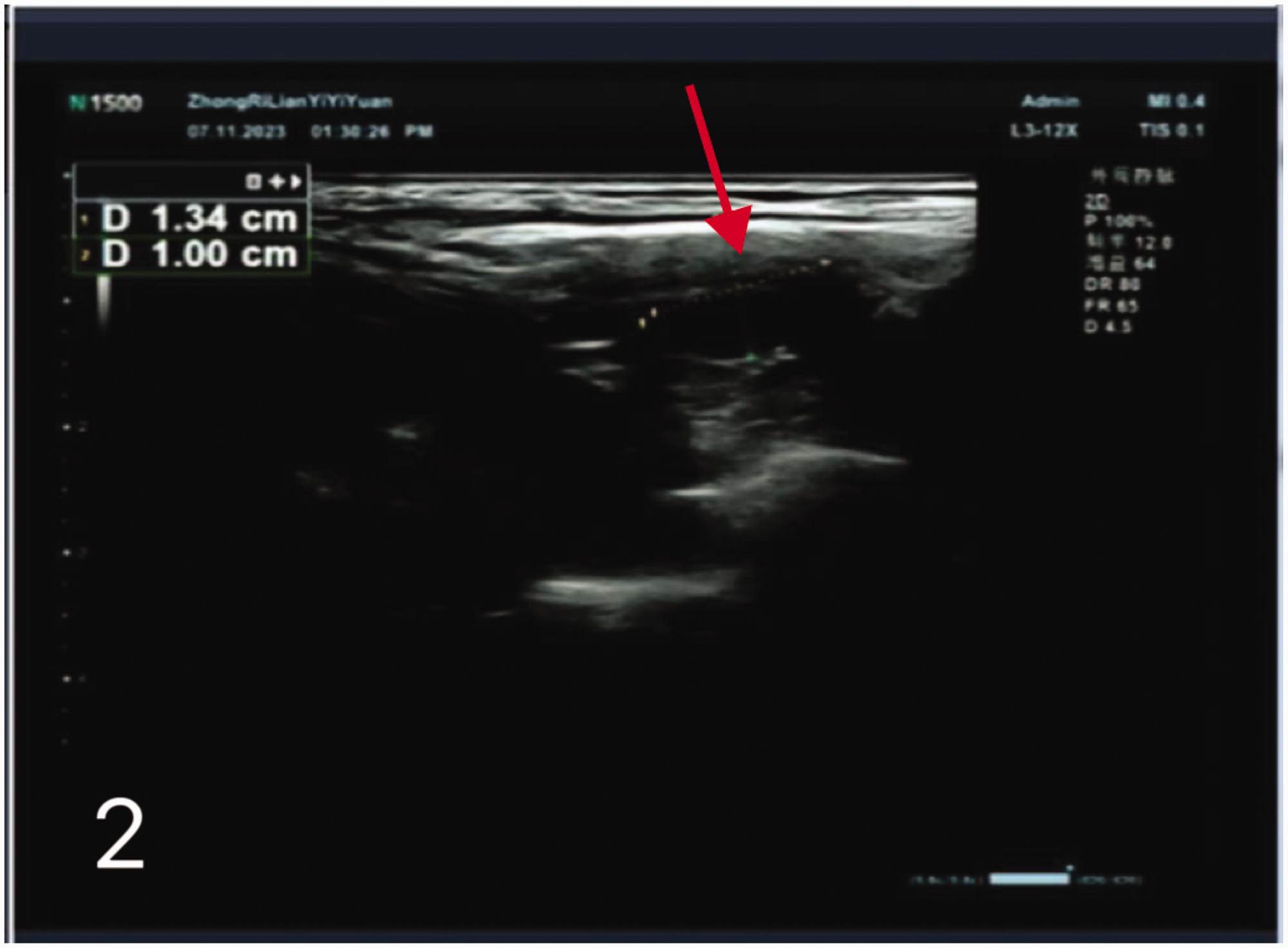
Color ultrasound of the neck showing hypoechoic lymph nodes, 1.34 × 1.0 cm in size, with poorly defined structure in area IV of the right neck.
To further clarify the nature of the lesion, ultrasound-guided fine-needle aspiration cytology (FNAc) of the left inferior polar nodules of the thyroid gland was performed. The results indicated a propensity for papillary thyroid carcinoma with a BRAF V600E (+) mutation. (The specimens for BRAF V600E gene mutation testing were obtained from the FNAc samples and analyzed by our pathology department, which is qualified to perform the test.) The FNAc results from area IV of the right neck showed epithelioid cells and lymphocytes.
Chest computed tomography (CT) revealed lesions in the upper tip segment of the right lung. Enlarged lymph nodes were observed in the mediastinum and right hilum of the lung. Metastasis could not be ruled out, and further examination was recommended. Based on the consultation from thoracic surgery, positron emission tomography (PET)/CT was performed, which showed increased glucose metabolism in the right clavicular region, mediastinum, and bilateral hilar lymph nodes. These findings were consistent with benign disease, specifically sarcoidosis (Figures 3 and 4). The combination of the FNAc results and fluorodeoxyglucose PET findings confirmed that the lymph node involvement was due to sarcoidosis. Thyroid function was normal.

PET/CT showing increased glucose metabolism in the right clavicular region, mediastinum, and bilateral hilar lymph nodes, consistent with benign disease (sarcoidosis).
The patient and her family voluntarily chose to proceed with radical surgery for left lobe thyroid carcinoma with central group lymph node dissection. The patient provided written informed consent for treatment. The diagnosis of coexisting papillary thyroid carcinoma and sarcoidosis was confirmed based on preoperative examinations and postoperative histopathological results.
After the surgery, the patient had no significant respiratory symptoms. Follow-up with chest CT and neck ultrasound was arranged. One month postoperatively, the patient’s thyroid function remained normal, and neck ultrasound showed no abnormalities or respiratory symptoms.
Ethical approval for this case was granted by the Ethics Review Committee of the China-Japan Union Hospital of Jilin University (No. 20240506010), and the case has been reported in accordance with the CARE guidelines. 2 In the process of obtaining written informed consent for treatment, it was agreed that the information could be used for scientific research; therefore, no specific consent for the publication of the case report was obtained. We collected information about the patient during the course of the clinical diagnosis and treatment, which did not involve the extraction of biospecimens or additional research procedures. As a result, the requirement for informed consent for publication was waived by the Ethics Review Committee of the China-Japan Union Hospital of Jilin University.
Discussion
Malignancy has been associated with sarcoidosis, and a linkage analysis provides evidence that the coexistence of both may be etiologically related in at least a quarter of cases. 3 A meta-analysis showed a significant increase in the incidence of thyroid disease in patients with sarcoidosis. 4 In addition to the association with papillary thyroid cancer in this case, other thyroid-related diseases, such as thyroid adenoma, Hashimoto’s thyroiditis, 5 and Graves’ disease, 6 can also coexist with sarcoidosis.
Both sarcoidosis and papillary thyroid carcinoma can present in thyroid nodules and cervical lymph nodes, making differential diagnosis essential. According to the Chinese expert consensus, 7 the diagnosis of sarcoidosis requires a comprehensive approach, while papillary thyroid carcinoma and metastatic cervical lymph nodes can be diagnosed with FNAc. In our patient, malignant nodules were detected in the left thyroid lobe as the initial diagnosis, while suspicious lymph nodes were observed in the right neck (area IV), despite no suspicion of nodules in the right lobe. This presented a challenge in determining the appropriate surgical approach, particularly the extent of cervical lymph node dissection.
Fortunately, we performed lymph node aspiration, chest CT, and PET/CT to further investigate the nature of the lymph node in the right neck, allowing us to limit the surgery to the left lesion. In contrast to our case, Katsamakas et al. 5 reported a misdiagnosis of papillary thyroid cancer with lymph node metastasis based solely on FNAc, leading to unnecessary surgery. Histopathological analysis later excluded malignancy and identified sarcoidosis.
Comparing the two cases, our patient benefited from a comprehensive preoperative diagnosis, which helped avoid misdiagnosis and unnecessary surgery. This highlights the importance of distinguishing sarcoidosis from malignant thyroid nodules and enlarged cervical lymph nodes prior to surgery. Accurate diagnosis influences the choice of surgical method, particularly the extent of cervical lymph node dissection, and affects the risk of postoperative complications and the patient’s quality of life.
For patients with newly diagnosed thyroid disease, we use cervical ultrasound as the preferred examination method. Shen et al. 8 suggested that various types of cervical Doppler color ultrasound under color Doppler flow imaging mode can help distinguish benign lymph nodes (such as those affected by sarcoidosis) from malignant lymph nodes. For lymph nodes and thyroid nodules suspected on cervical ultrasound, FNAc is commonly chosen as the next diagnostic step. However, as reported by Katsamakas et al., 5 FNAc has limitations in diagnosing thyroid sarcoidosis. This is because reactive follicular cells can form proliferative papillary structures together with giant cells caused by sarcoidosis, which resemble those of papillary thyroid carcinoma. Additionally, colloid condensation within the papillary structure may be misinterpreted as psammoma bodies.
As an alternative, core needle biopsy (CNB) appears to provide better diagnostic accuracy than FNAc while being less invasive than surgical biopsy,1,9 making it a valuable diagnostic method for obtaining a pathological diagnosis. 9 However, other studies have shown that FNAc and CNB are complementary in the diagnosis of thyroid nodules and cannot fully replace each other. 10 To better follow the principle of comprehensive diagnosis, patients with suspected pulmonary nodules and mediastinal lymph node enlargement can undergo whole-body PET/CT examination supplemented by fluordeoxyglucose PET/CT for monitoring disease progression. 1
Conclusion
When malignant thyroid nodules are accompanied by swollen cervical lymph nodes, FNAc or CNB can be used to determine the nature of the thyroid nodule and lymph nodes when preoperative ultrasonography is inconclusive. PET/CT can help diagnose systemic conditions to support a comprehensive diagnosis. As specialists, we must avoid fixed thinking. In cases of suspicious thyroid nodules and cervical lymph nodes, it is essential to differentiate between malignant and benign findings, communicate promptly with patients and their families, and conduct further examinations to achieve a clear diagnosis. This helps avoid misdiagnosis and unnecessary surgery, leading to treatment plans that improve patient outcomes. Although our patient has undergone thyroid surgery, sarcoidosis has not been treated. Given the association between malignancy and sarcoidosis, regular follow-up is necessary to monitor disease progression.
Footnotes
Acknowledgements
We would like to express our gratitude to the corresponding author for their critical review of this manuscript. We also thank the other authors for their contributions to this article.
Authors’ contributions
Chengcheng Duan was responsible for reviewing the literature and writing the paper. Ping Yu, Xianji Wu, and Siqi Xiao were in charge of collecting information. Wenxi Yu, Jingyue Zhong, and Xinran Wei summarized the data. Guang Zhang reviewed the manuscript and proposed revisions.
Availability of data and materials
The data and materials used in this study are available upon request from the corresponding author.
Declaration
Patient identifying information has been removed from this article. This study does not involve human subjects, human tissues, or animals.
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82072184).