
Abstract
Objective:
The objective of this study is to demonstrate the sonographic and computed tomographic features of venous pseudoaneurysms and show the difference between true and false venous aneurysms and arterial pseudoaneurysms. Likewise, it was important to provide a historical context based on a literature review of vascular aneurysms and pseudoaneurysms, emphasizing venous pseudoaneurysms.
Materials and Methods:
Clinical cases are presented for context, and the vascular examinations were performed utilizing a General Electric (GE) Logiq Fortis or Logiq S8 scanners with a broad-band linear-array transducer (L2-9). Computed tomography (CT) with contrast was performed on a GE Revolution Maxima 64-slice CT scanner with 100 mL Omnipaque-350 as a contrast agent. The three-dimensional (3D) axial, sagittal, and coronal reconstructions were made with the Philips IntelliSpace software. Levels of evidence are provided based on a literature search of relevant publications using the National Library of Medicine, PubMed, and Google Books.
Results:
Different types of venous pseudoaneurysms, venous aneurysms, and arterial pseudoaneurysm diagnosed by duplex sonography and CT were presented. An extensive historical and literature review was conducted based on publications from the 18th to 21st centuries.
Conclusion:
Venous pseudoaneurysms are uncommon. Most of them are iatrogenic and are usually found as a complication of repetitive venipuncture in patients receiving hemodialysis with arteriovenous fistulas. In rare cases, venous pseudoaneurysms occur spontaneously.
Vascular pseudoaneurysms are abnormal dilations of the blood vessel wall when one or two of the triple layers (tunica intima, media, and adventitia) within the vascular wall ruptures and leads to focal outpouching. Rarely, a sudden tear of a vascular wall develops spontaneously (idiopathic, without identifiable causes) or, more commonly, due to underlying connective tissue disorder or autoimmune, multisystemic vasculitis.1 –3 The most common etiology of vascular pseudoaneurysms includes blunt and penetrating injuries (including iatrogenic injuries) to the vascular wall. A blunt trauma can cause vascular pseudoaneurysms because the acceleration-deceleration forces affect a vascular wall while penetrating vascular injuries (including iatrogenic) can lead to the incomplete closure/healing of the pierced site. 4
Pseudoaneurysms (also known as false aneurysms, spurious aneurysms, and pulsating hematomas) have necks and sacs that can be thrombosed partially or completely. False aneurysms affect both the arteries and veins. Arterial pseudoaneurysms are more common than venous ones. Deep and superficial false venous aneurysms (FVAs) develop in large and small vessels. Duplex sonography (DS) is currently a main diagnostic imaging technique for venous pseudoaneurysms. Occasionally, sonographers and radiologists discover FVAs incidentally, or when they mimic other pathologies. The purpose of this article was to review venous pseudoaneurysms and describes their differentiation from similar vascular abnormalities.
Prior to the introduction of modern radiologic diagnostic procedures such as DS, digital subtraction angiography (DSA), computed tomography (CT), computed tomography angiography (CTA), and magnetic resonance angiography (MRA), venous aneurysms and pseudoaneurysms (See Figure 1) were mostly diagnosed clinically and confirmed microscopically after they were surgically removed and their walls were analyzed under a microscope.5,6
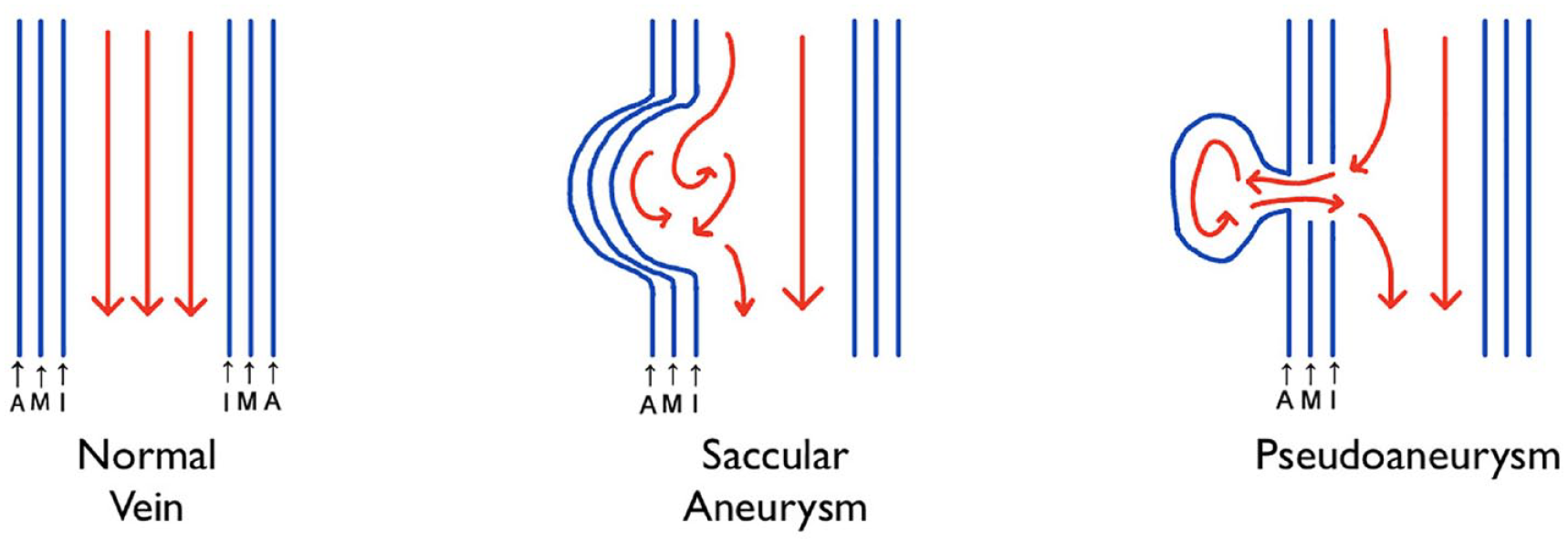
An illustration of the normal vein and changes that result in a saccular aneurysm and pseudoaneurysm. A, tunica Adventitia (the outer layer of the venous wall); M, tunica Media (the middle layer); I, tunica Intima (the innermost layer of the venous wall).
In contrast to false aneurysms, vascular aneurysms are focal mural dilatations that are twice the caliber of the regular adjacent segment with all three layers of the affected wall intact. Venous pseudoaneurysms can mimic masses, true aneurysms, and arterial false aneurysms. 5 Clinical history (penetrating or blunt traumas and connective tissue diseases such as Marfan syndrome, Ehlers-Danlos syndrome, Neurofibromatosis Type 1, and Loeys-Dietz syndrome) helps to consider the presence of a vascular pseudoaneurysm. 7 Although DS is usually the first diagnostic vascular imaging technique, it has certain limitations, which in some cases prevent the sonographer from obtaining clear diagnostic color and spectral Doppler images of false aneurysms. This may be because of their location (situated too deeply) and whether they were partially or completely thrombosed. Although DSA, CTA, and MRA are costly and invasive procedures, these are typically more accurate and frequently used to confirm and clarify DS findings.
Materials and Methods
This literature review was pursued to accomplish three main goals: (1) demonstrate the sonographic and CT features of FVAs; (2) show the difference between the true and FVAs and arterial pseudoaneurysms; and (3) provide a historical and literature review of vascular aneurysms and pseudoaneurysms, emphasizing venous pseudoaneurysms (section “Discussion” of this article).
Equipment Used as Part of Providing Clinical Context
The vascular sonographic examination, provided for clinical context, was performed by a lead vascular technologist, utilizing a General Electric (GE) Logiq Fortis or Logiq S8 (GE Medical, Waukesha, WI, USA). A broad-band linear-array transducer (L2-9) was used to visualize the veins and arteries. Computed tomography with contrast was performed on a GE Revolution Maxima 64-slice CT scanner (GE Medical). 100 mL Omnipaque-350 was used as a contrast. The three-dimensional (3D) axial, sagittal, and coronal reconstructions were made with the Philips IntelliSpace software.
Literature Review Methodology
A search was conducted for the relevant publications from the 20th and 21st centuries retrieving works from the National Library of Medicine (Bethesda, MD, USA) PubMed Central (PMC) and Google Scholar using the following keywords: “venous pseudoaneurysm,” “false venous pseudoaneurysm,” “venous aneurysm,” “duplex or Doppler venous pseudoaneurysm/or aneurysm,” and a grouping of keywords for x-ray, CT, MRA, and duplex of pseudoaneurysms. The full-text articles were accessed on the corresponding medical journals’ websites or in our local public library. Searches for the articles and manuscripts published prior to the 20th century were performed using Google Books, utilizing the keywords “pseudoaneurysm,” “false aneurysm,” “pulsating hematoma,” and “spurious aneurysm.” There were 7025 articles and textbooks found from the databases searched. After all screening and exclusion processes, 40 references were included for the historical and literature review (See Figure 2).
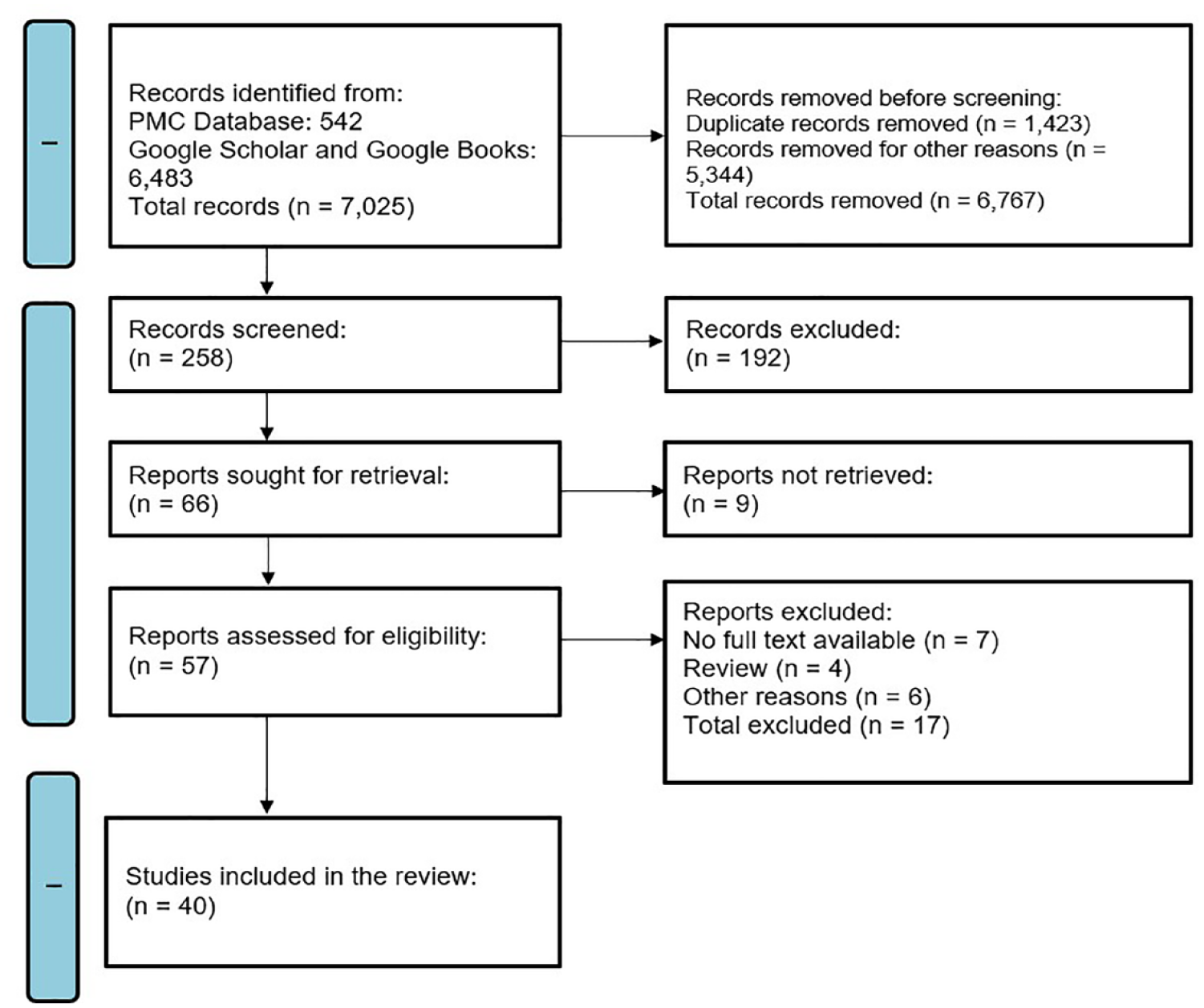
The preferred items for reporting for systemic review and meta-analysis articles (PRISMA) flow diagram that shows the algorithm used to provide a compatible literature review. PMC—PubMed Central (PMC) of National Library of Medicine.
Results
A clinical case is provided to highlight the diagnostic features of FVAs and to provide clinical context. Likewise, a compatible literature review is provided to underscore the levels of evidence that informs this diagnosis.
Sonographic Features and Correlation with CTA
A female patient in her 40s, identified a superficial, painless, non-pulsatile, soft, partially compressible “mass,” on her right lower neck (See Figures 3–7), a few months prior. During the physical examination, the patient’s primary care physician suspected possible lymphadenopathy, a superficial mass, or vascular abnormality. The patient reported she was a victim of domestic abuse; her partner had inflicted blunt injury to her neck 4 years before the appearance of the cervical mass. In addition to the prominent subcutaneous ecchymosis, the patient did not suffer any visible immediate injuries after the attack. The patient’s primary physician requested a unilateral right upper extremity venous duplex examination. The institutional protocol for this examination included the internal jugular, brachiocephalic (innominate), subclavian, axillary, brachial, radial, ulnar, median cubital, basilic, and cephalic veins. All the veins appeared normal during the sonographic examination. Extending the imaging protocol, it was important to perform a targeted scan over the questionable “mass,” to establish the nature of that lesion. The superficial mass corresponded to a partially thrombosed sac of the right external jugular vein (EJV) pseudoaneurysm (See Figures 3–5). The neck of the false aneurysm measured 0.13 cm in diameter (See Figure 3). Spectral Doppler identified a pulsatile with spectral broadening, low velocity, with a bidirectional component (above and below the baseline) waveform pattern in the neck of the false aneurysm (See Figure 5). The DS findings well correlated well with CTA of the cervical veins, which also demonstrated a pseudoaneurysm of the right EJV with similar measurements (See Figures 6 and 7).
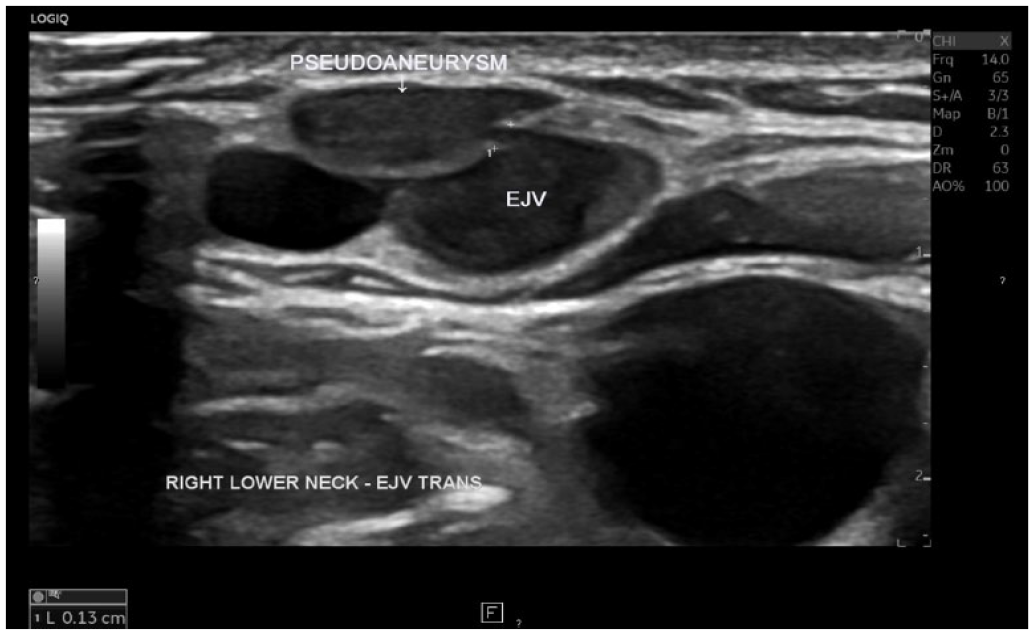
A grayscale transverse image of the right EJV. The sonogram shows the neck of the pseudoaneurysm (measuring 0.13 cm in diameter). The sac of the pseudoaneurysm is marked with an arrow. EJV, external jugular vein.
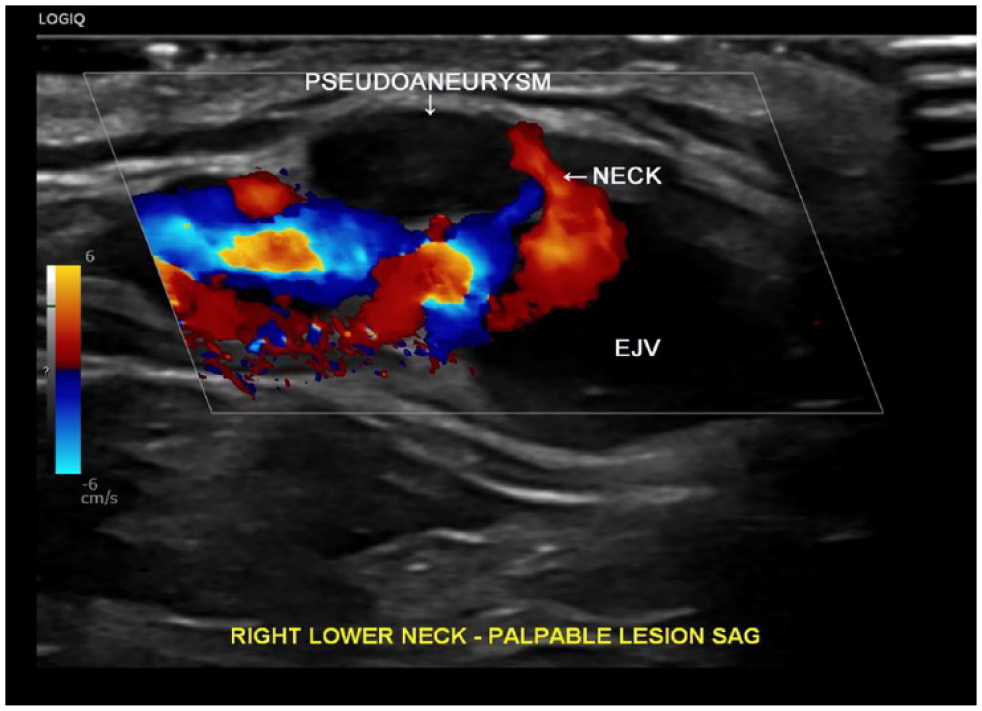
A color Doppler sagittal image demonstrates blood flow via the neck of the external jugular vein pseudoaneurysm. EJV, external jugular vein.
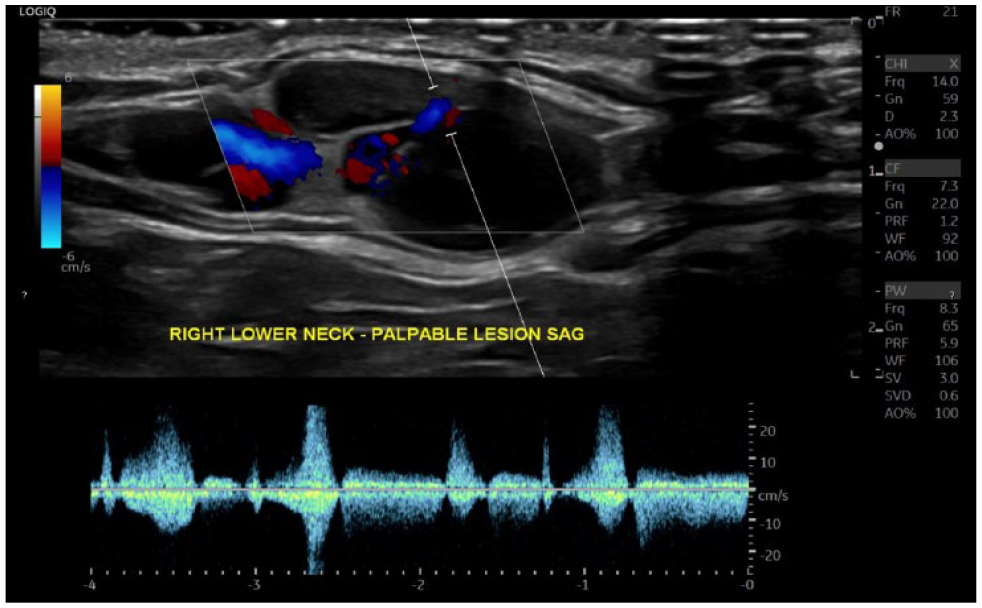
A sagittal duplex image of the external jugular vein demonstrated a pulsatile signal with spectral broadening, low velocity flow, with a bidirectional component spectral Doppler waveform pattern in the neck, of the false aneurysm.
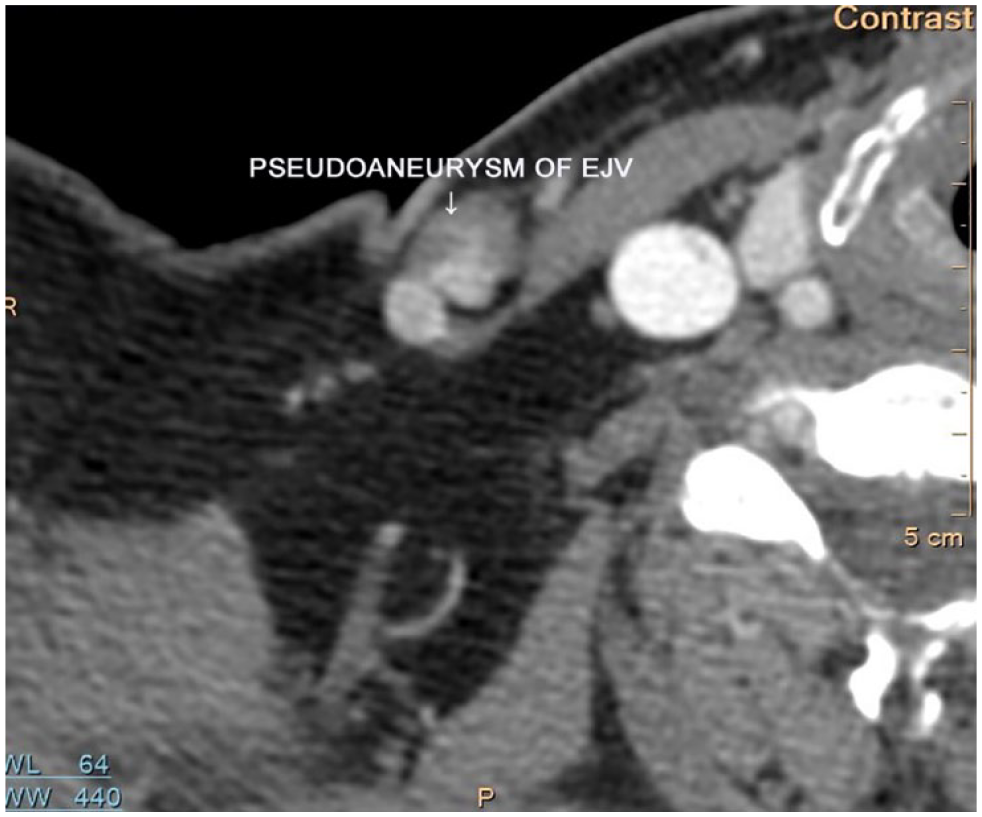
A selected image from the computed tomography angiography (CTA) of the right EJV that demonstrates a pseudoaneurysm. EJV, external jugular vein.
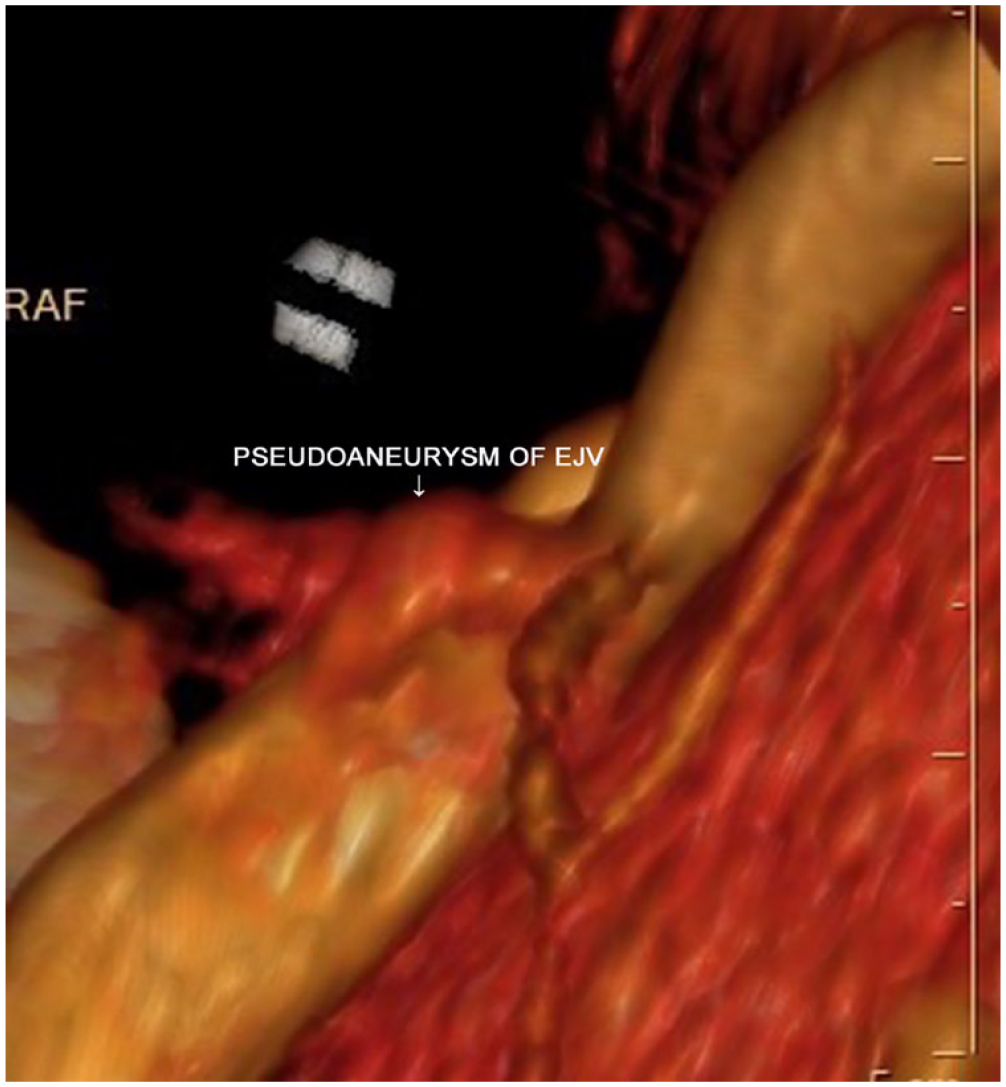
A 3D reconstruction of computed tomography angiography (CTA) confirmed the presence of a false aneurysm in the right EJV. EJV, external jugular vein.
Differentiation of True and False Venous Aneurysms and Arterial Pseudoaneurysms
False aneurysms of the EJV are clinically rare. However, pseudoaneurysms and aneurysms of the superficial veins of the upper extremities are well-known complications in patients receiving hemodialysis with peripheral arteriovenous fistulas (AVFs)8,9 (See Figures 8–10).
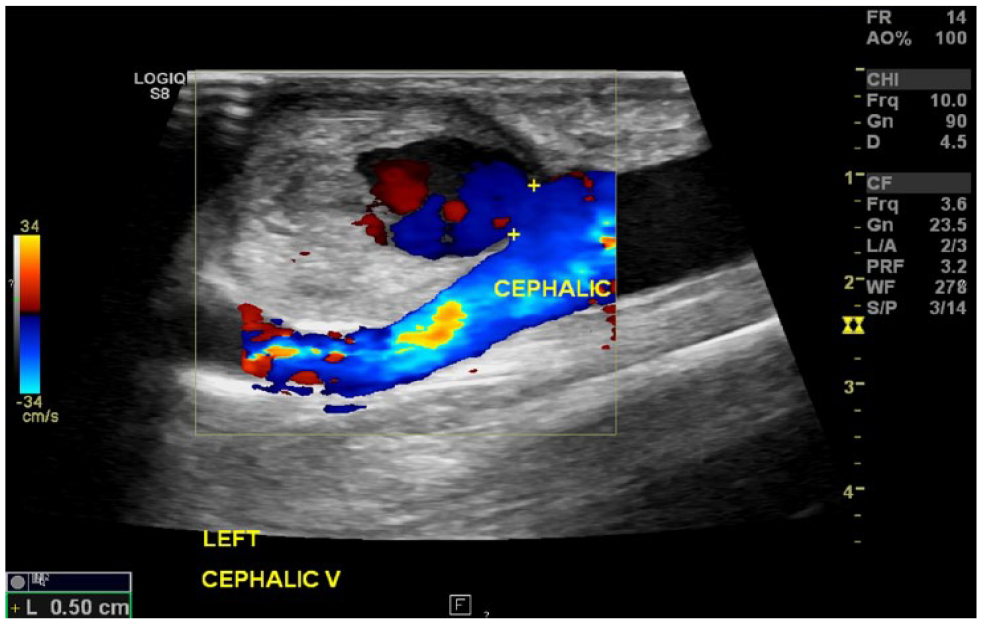
A sagittal color Doppler image demonstrated blood flow via the neck (its diameter measured with calipers) of a partially thrombosed left cephalic vein pseudoaneurysm (developed because of repetitive venipunctures in a patient on hemodialysis with an arteriovenous fistula).

A grayscale sagittal view of the left cephalic vein (in a patient receiving hemodialysis with an arteriovenous fistula) demonstrating a true aneurysm with a maximal anterior-posterior diameter of 3.8 cm (the normal adjacent proximal segment measured 1.7 cm in diameter).

A grayscale sagittal view of the left cephalic vein (in a patient receiving hemodialysis with an arteriovenous fistula) demonstrating a false aneurysm with a neck that measures 0.6 cm in diameter.
Like true aneurysms, FVAs occur in deep, superficial, visceral, and peripheral veins.10 –13 Radiologically, venous aneurysms are defined as focal dilatations that are twice the caliber of the proximal and normal adjacent vein. 14 Sonographically, arterial pseudoaneurysms appear very similar to FVAs, especially in grayscale. However, because of the arterial pulsatile flow pattern, high-amplitude bidirectional (“to-and-fro”) Doppler waveforms, and usually higher than venous flow peak systolic velocities, the disparity between the two is obvious with Doppler sonography. 15 The differentiation between the venous and arterial pseudoaneurysms becomes challenging when the sac of a pseudoaneurysm is thrombosed and if a venous pseudoaneurysm has arterialized blood flow, as in patients with an AVF for hemodialysis, which mimics arterial pseudoaneurysms (See Figures 5, 11, and 12). False venous aneurysms in hemodialysis patients with AVF or arterial-venous graft (AVG) show similar to the non–hemodialysis-related FVAs spectral Doppler waveforms: pulsatile with spectral broadening, with a bidirectional component, but with much higher velocities (amplitudes) because of their arterialized flow.
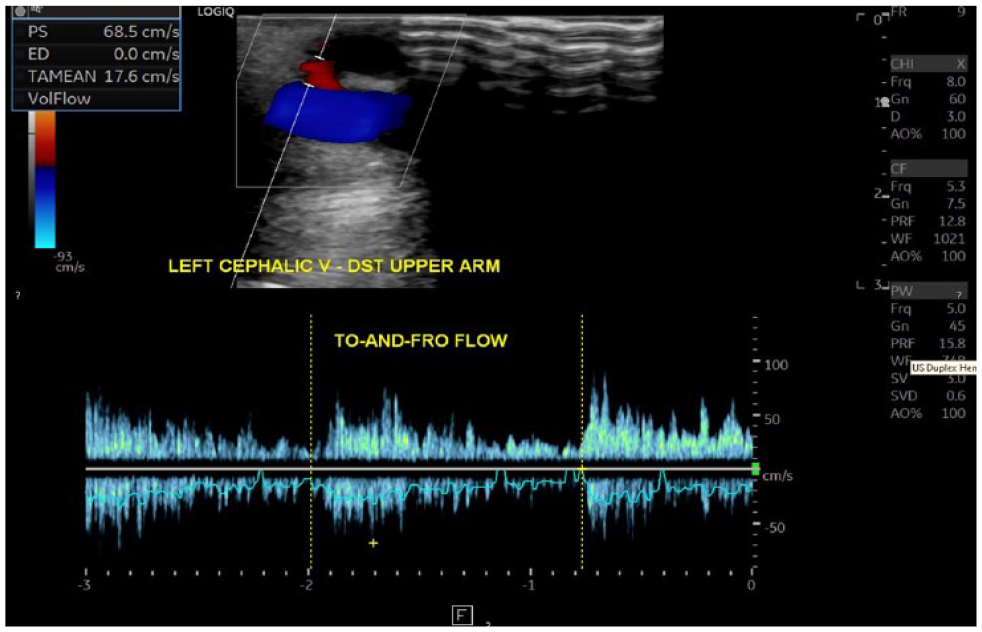
A duplex Doppler image of the left cephalic vein pseudoaneurysm demonstrating a pulsatile with spectral broadening, high velocity, with a bidirectional component spectral Doppler waveform pattern of the arterialized venous flow in the neck of the false aneurysm. This image was taken on a patient receiving hemodialysis with a brachial-cephalic arteriovenous fistula.
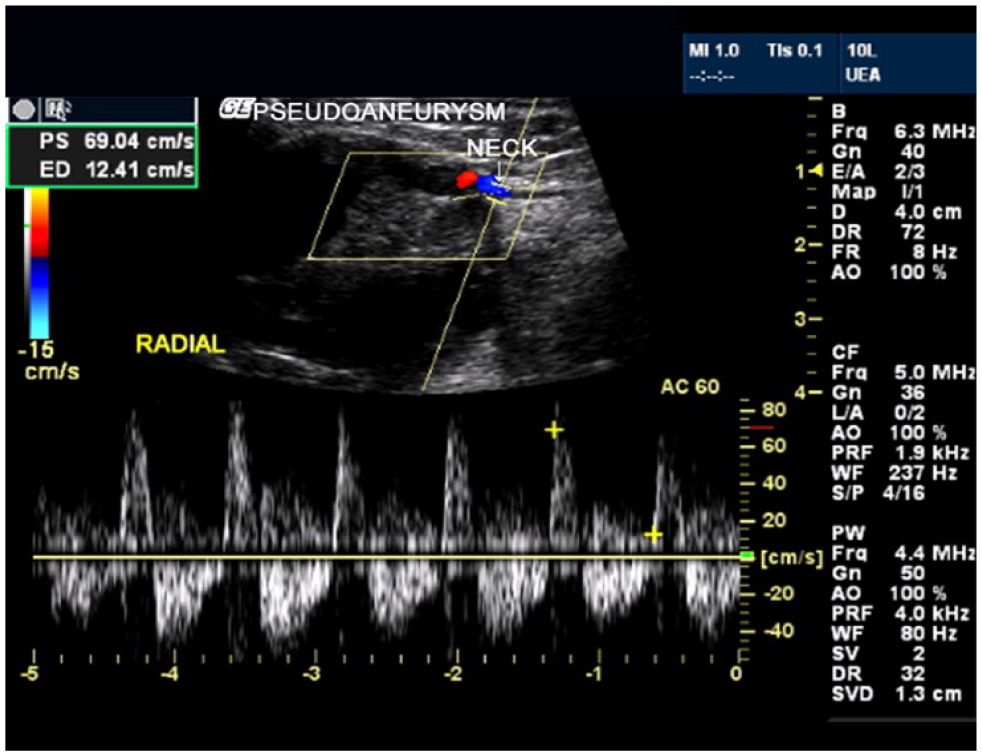
Duplex image of the right radial artery pseudoaneurysm (that developed after a python’s bite) demonstrating a typical bidirectional high velocity spectral Doppler waveform pattern of the arterial flow in the neck.
The Yin-Yang sign can also be detected using color Doppler in the pseudoaneurysm sac (See Figure 13). In vascular sonography, this ancient Chinese symbol corresponds to bidirectional blood flow within a sac of the pseudoaneurysm.16,17
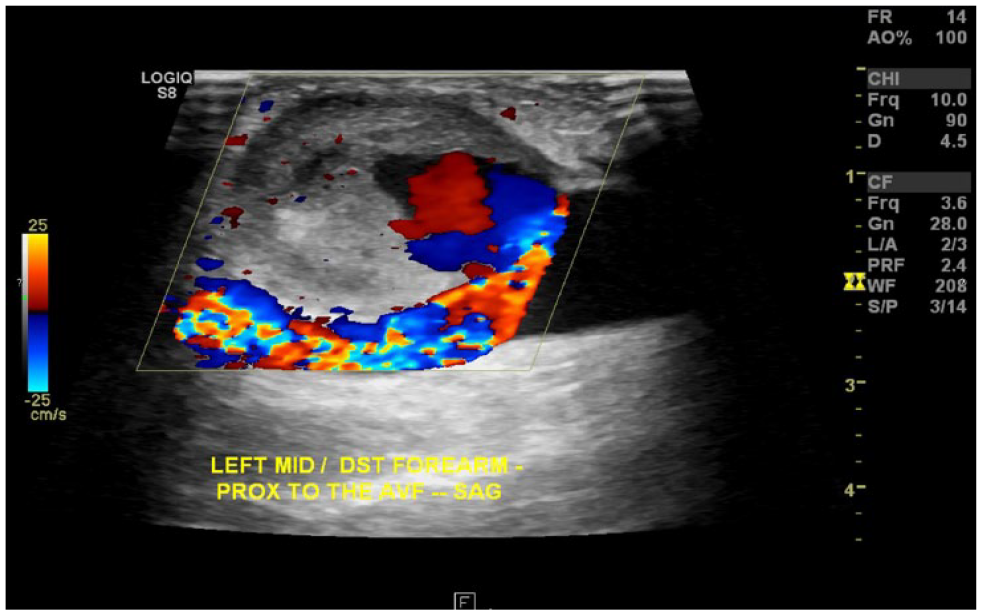
A color Doppler image is provided of a partially thrombosed left cephalic vein pseudoaneurysm (patient receiving hemodialysis with an arteriovenous fistula) demonstrating the Yin-Yang sign (also known as the “Pepsi sign”)—intermixed (turbulent/swirling) red and blue colors within the sac. The inflow appears in red (toward the transducer), while the outflow appears in blue (away from the transducer).
Discussion
One of the oldest references to vascular false aneurysms in the English language medical literature dates back to 1730, in which false aneurysms were reported to be caused by external factors, such as wounds and punctures in bloodletting.
18
As a result:
The coats [mural layers] of arterial pseudoaneurysms are being reduced to one and the tumor [the sac of a pseudoaneurysm] is formed by extravasated blood; while the true aneurysms form by a dilatation of the whole substance [with all mural layers intact] of the artery.
18
In 1758, false arterial aneurysms were first described as circumscribed and pulsating. A “false aneurysm beats under pressure, like the true aneurysm. It consists of one bag that communicates by an aperture with the cavity of the artery.” 19 More than 260 years later, this definition is still acceptable. There were a few other publications on false aneurysms in the 18th century, all of which involved the arteries. 20
In the 19th century, as part of aneurysm classification, aneurysma spurium was defined as follows:
Internal and middle membranes [of a vessel are being] destroyed, external membrane composing the aneurismal sac; in every instance, fibrinous coagula [thrombosis] form in concentric layers within the sac. The sac, at its origin, is contracted, and attached by a pedicle or neck, narrow where the aneurism proceeds from laceration,
21
which is compatible with a modern characterization of partially thrombosed false aneurysms. An investigation of how easily false aneurysms can be confused with other clinical entities, especially when they mimic abscesses, was published in 1847. Without any diagnostic radiologic methods available at the time, physicians, inevitably, had made some critical mistakes in diagnosing and surgically treating such patients. 22
From the first reported cases of false aneurysms in the first half of the 18th century until the first half of the 20th century, physicians have utilized physical examination as the only method to diagnose pseudoaneurysms and all other vascular pathologies in living patients. Only postmortem dissections or surgically removed affected segments of the vessel, followed by analysis of the specimen under a microscope, would establish the final diagnosis of false vascular aneurysms. As a result, the misdiagnosis of pulsating hematomas in clinical practice was quite common, sometimes causing catastrophic consequences, even in the second half of the 20th century. A false aneurysm mistaken for an abscess and subsequent drainage is a prime example of a deleterious error in medical diagnosis. 10
With the discovery of x-radiation, in 1895, by Roentgen in Germany, diagnostic medical radiology was established. 23 X-ray-based angiography was developed in the first half the 20th century, allowing premortem diagnosis of various vascular diseases. 24 In the 1940s, venography had already been used successfully to diagnose deep vein thrombosis in the lower extremities. 25 Computed tomography with following CTA, magnetic resonance imaging (MRI) with subsequent MRA, and DS had been discovered and introduced into clinical practice in the 1970–1980s.26 –30
Because both true venous aneurysms and pseudoaneurysms are rare and challenging to diagnose, they were not clearly differentiated until the 1990s. Some medical publications titled as “venous aneurysms” were in fact describing FVAs. One of the first published articles about venous pseudoaneurysm (titled as “aneurysm of a small vein in the cheek”) appeared in 1952, describing a false aneurysm of a small vein in the cheek, which presurgically was considered to be a lipoma vs a mucus retention cyst. Only the microscopic analysis of the surgically removed “nodule” in that case confirmed the presence of an FVA caused by a previous trauma. 31 Only 12 cases of both true and FVAs were reported by the year 1980. 32
By 2023, a few dozen cases of visceral (abdominal and thoracic) venous pseudoaneurysms had been described in the literature, most of which were caused by blunt traumas.11,33 –36 Non-iatrogenic FVAs are very rare. By 2016, only five such cases had been recorded. Significantly identifiable trauma was common in all those cases.12,13
Currently, pseudoaneurysms of various non-visceral veins including the subclavian, axillary, common femoral, greater saphenous, internal, and EJVs have been reported.1,4,32,37,38 Pseudoaneurysms of the external jugular vein are rare, with only three case reports published in the literature as of 2020.12,39,40
Conclusion
Venous pseudoaneurysms are clinically very uncommon. Morphologically and sonographically, these lesions are like arterial pseudoaneurysms. Hemodynamically, the main difference between the venous and arterial pseudoaneurysms is the spectral Doppler waveform pattern sampled from the pseudoaneurysms’ neck: pulsatile with spectral broadening, low velocity with a bidirectional component in the FVAs, whereas prominently bidirectional, high velocity in the arterial pseudoaneurysms. Venous pseudoaneurysms in hemodialysis AVF are more like the non-AVF venous than the arterial pseudoaneurysms but usually have higher velocities. Most FVAs are iatrogenic and are usually found as a complication of repetitive venipuncture in patients receiving hemodialysis with AVF. Non-iatrogenic FVAs can develop in either the visceral or the peripheral veins, often after a blunt trauma. In rare cases, venous pseudoaneurysms occur spontaneously.
Sonographers and radiologists should be aware that some superficial asymptomatic lesions might represent venous pseudoaneurysms in unexpected areas, such as the neck or upper and lower extremities. A detailed clinical history, especially a history of any prior trauma to the area of interest, and proper physical examination, in addition to vascular radiologic examinations, are paramount for the correct diagnosis of FVAs.
Key Takeaways
Pseudoaneurysms affect both the arteries and veins. Arterial pseudoaneurysms are more common.
Duplex sonography is usually the first diagnostic imaging technique for superficial and peripheral venous and arterial pseudoaneurysms.
Most venous pseudoaneurysms are iatrogenic and are usually found as a complication of repetitive venipuncture in patients receiving hemodialysis with arteriovenous fistula.
Some superficial asymptomatic lesions might represent venous pseudoaneurysms, especially in the patients who have had prior blunt injuries of the affected area.
A detailed clinical history and proper physical examination, in addition to duplex sonography, and other radiologic examinations, are paramount for the correct diagnosis of false venous aneurysms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because the adherence to all regulatory and ethical rules of the host diagnostic center.
Informed Consent
Informed consent was not sought for the present study because all case images and data were de-identified and followed IRB guidelines (also referred as the Honest Broker System).