
Abstract
Active bleeding from a small branch of the femoral artery can occur after catheterisation and may be difficult to treat. Stent-graft placement or embolisation after catheterisation can be a useful solution. However, stent-graft placement is often challenging for the treatment of bleeding around bifurcations, and it may be limited by available stent-graft sizes during emergencies. Embolisation can also be difficult if the vessel diameter is too small to catheterise or if the branching angle is too acute. Thrombin injection is accepted as a safe and effective treatment for iatrogenic or traumatic pseudoaneurysm. However, large haematomas can deter ultrasonographic guidance. We herein report the successful treatment of active bleeding from a small branch of the superficial femoral artery after femoral access by percutaneous direct puncture under angiographic guidance and thrombin injection at the bleeding focus.
Introduction
Active bleeding or pseudoaneurysms can be treated by endovascular or percutaneous thrombin injection.1–3 Endovascular stent-graft placement is often limited by the bleeding site location and the availability of appropriately sized stent-grafts. Furthermore, stent-grafts do not guarantee long-term patency. 1 The endovascular use of embolic material is not possible when the arterial bleeding site is too small or the branching angle is too acute. Percutaneous direct puncture of a pseudoaneurysm is effective and safe; however, it is commonly applied to aneurysmal sac-forming bleeding under the guidance of ultrasonography (US). 1 We herein report the successful treatment of bleeding from a superficial femoral artery (SFA) branch after femoral access that was too small for endovascular catheterisation and detection by US. Instead, thrombin was used via direct percutaneous puncture under angiographic guidance.
Case description
Our institutional review board approved this case report. The images in this study were fully anonymous; therefore, informed consent was not required.
A 91-year-old woman was referred for painful right thigh swelling and skin colour change 11 days after coronary artery catheterisation. Computed tomography revealed active bleeding at the right SFA and an associated large haematoma (Figure 1). Although the bleeding had occurred after catheterisation, the focus was far from the puncture site. Anticoagulation after coronary stent implantation and the mass effect from the haematoma that had formed after catheterisation were considered as the causes of the bleeding. Transcatheter angiography via the left common femoral artery showed arterial bleeding from a small branch of the right SFA (Figure 2). Catheterisation with a 1.9-Fr microcatheter (Carnelian; Tokai Medical Products, Aichi, Japan) failed because of the small diameter of the bleeding artery. Two attempts to perform temporal balloon tamponade, approximately 60 s each, also failed to achieve haemostasis. Direct compression over the bleeding focus was also ineffective because of the large overlying haematoma. Direct percutaneous puncture of the distal bleeding artery was attempted under angiographic roadmapping and fluoroscopic guidance with a 21-G Chiba needle (Figure 3). Upon gradual withdrawal of the needle, blood flowed out from the needle hub, indicating contact with the bleeding focus. A 2000-IU injection of diluted thrombin effectively embolised the bleeding on the second attempt (Figure 4). A 14-Fr pigtail catheter was placed to drain the haematoma serum. The patient recovered from haemodynamic instability and underwent escharectomy due to pressure-associated ischaemic skin necrosis. After additional surgeries for wound care, she was discharged in healthy condition.

A 91-year-old woman who underwent coronary angiography 11 days earlier presented with painful right thigh swelling. Computed tomography shows volcano-like bleeding (solid arrow) underneath a large haematoma (arrows).

A right superficial femoral arteriogram via microcatheter shows active bleeding from a small branch of the superficial femoral artery (black arrows).
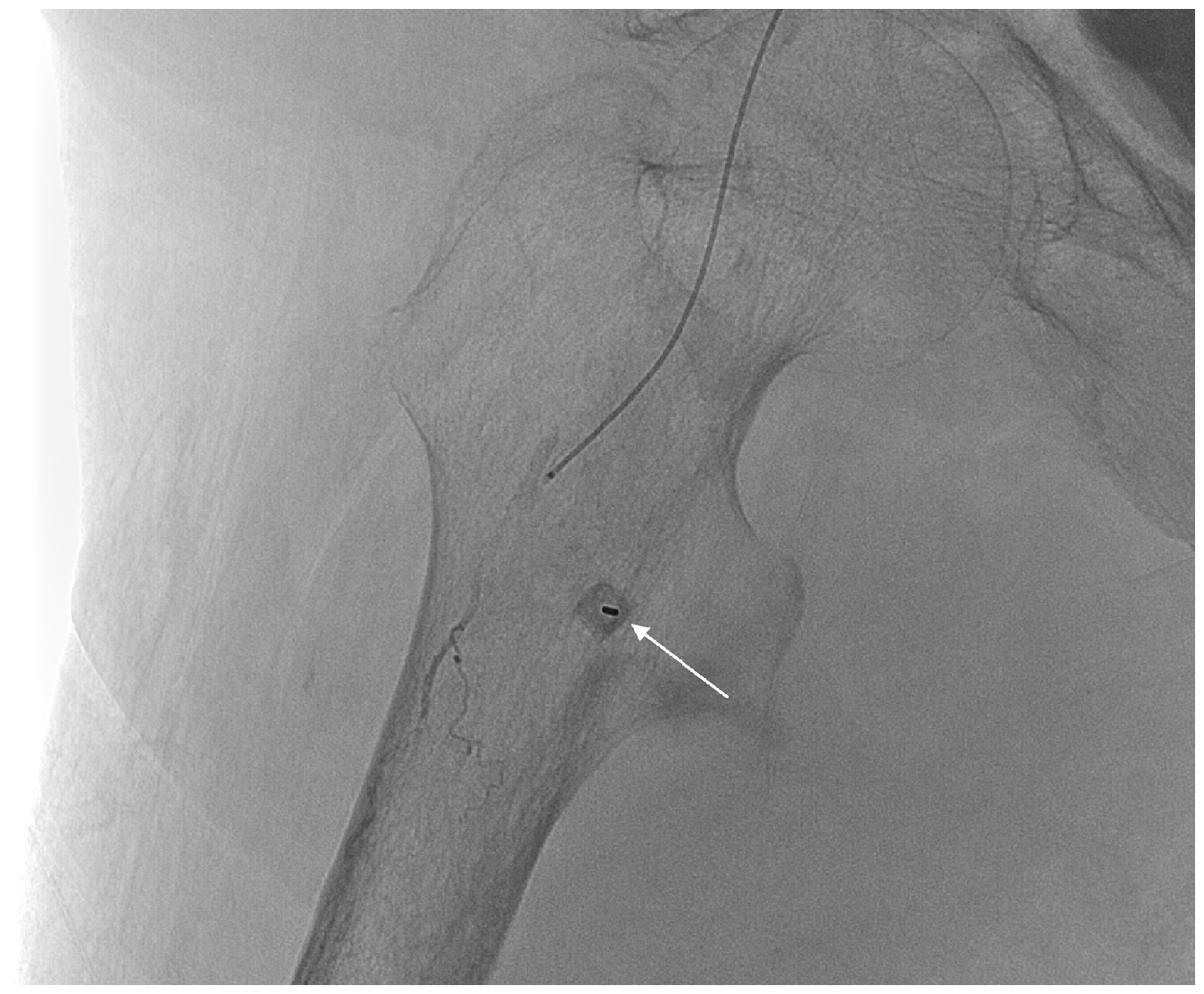
A 21-gauge Chiba needle (arrow, en face view) inserted percutaneously at the bleeding artery under the guidance of a pre-acquired road map image. Thrombin was injected as blood flowed out during slow withdrawal of the needle.
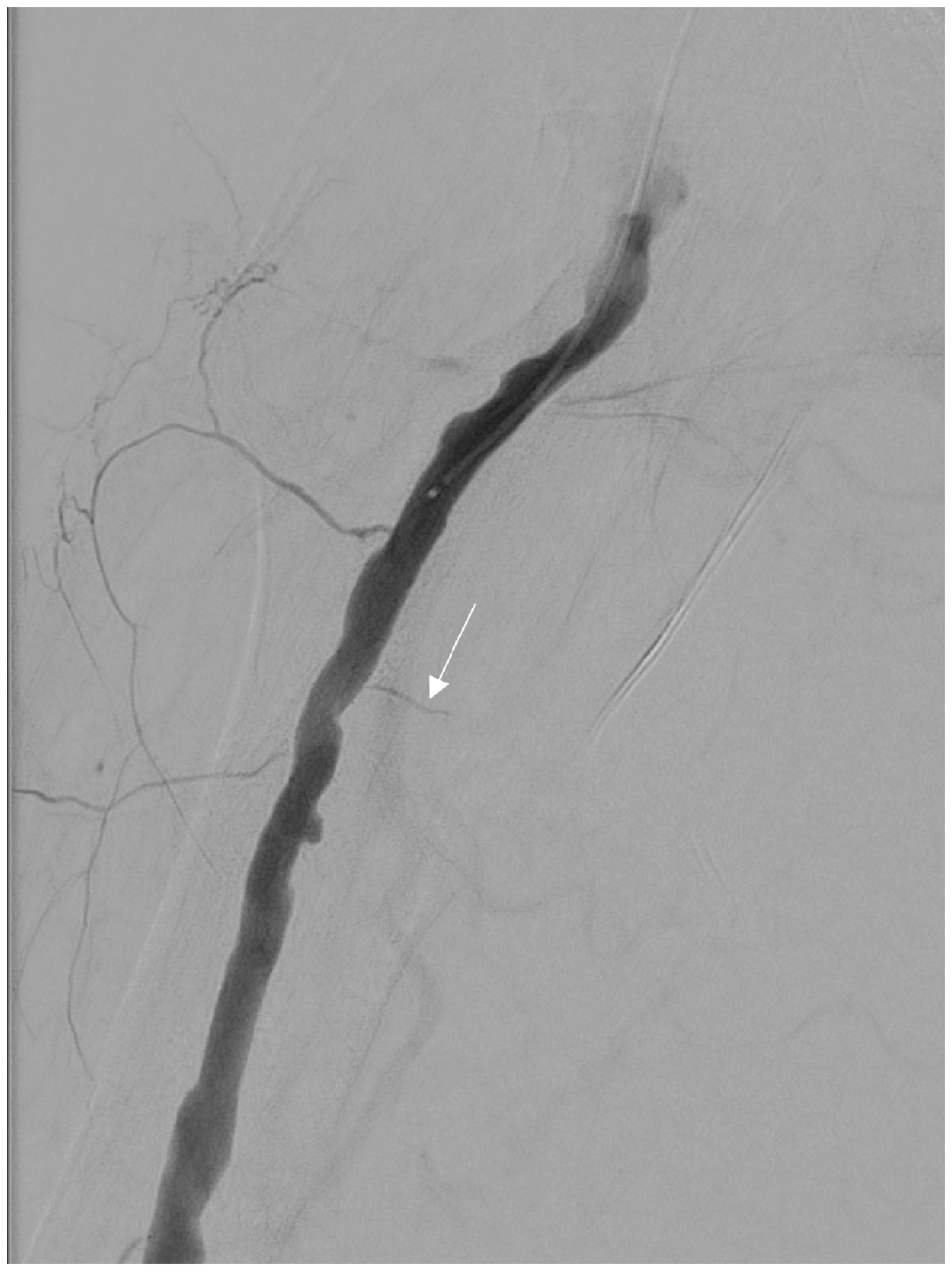
The final angiogram shows no further contrast media leakage at the previous bleeding focus (white arrow).
Discussion
We have herein described a case of thrombin injection into a small bleeding artery under angiographic guidance. Although the first attempt was unsuccessful, immediate haemostasis was achieved during the second attempt, and no serious complications followed. Several methods are available to achieve haemostasis in patients with active bleeding from femoral arteries. Manual or US-guided probe compression at the bleeding focus is an easy and readily available method. 1 However, this compression method often fails in patients who have a deep bleeding focus (e.g., deep femoral artery bleeding), have a large overlying haematoma, or are undergoing anticoagulation treatment.1,3 Thrombin injection into a pseudoaneurysm after direct percutaneous puncture under US guidance can be a safe and effective method.3,4 Samal et al. 5 reported four cases of femoral artery pseudoaneurysms treated by angiography-guided thrombin injection and balloon occlusion. In the present case, we injected thrombin directly into a small branching artery; this differs from the study by Samal et al., 5 in which thrombin was injected into the pseudoaneurysm. Intravascular balloon tamponade is worth attempting, although longstanding flow occlusion can cause distal artery embolism. 6 Another method is the injection of embolic materials into the pseudoaneurysm after catheterisation or direct puncture.1,7 However, considering that pseudoaneurysms have no solid outer wall, the use of embolic materials such as coils may lead to rupture of the pseudoaneurysm and potential future infection. 1 Placement of a stent-graft is safe and effective, although long-term patency is not guaranteed and the availability of appropriate stent sizes is limited in emergencies.1,2 Stent placement would be better reserved as a last resort.
Conclusions
In the present case, a large haematoma hindered our ability to locate the bleeding focus by US. We injected thrombin directly into the bleeding artery under angiographic guidance. Although the bleeding focus was not precisely accessed, dissemination of thrombin around the site embolised the bleeding, facilitating treatment. To prevent further iatrogenic injury and precisely target the bleeding focus, meticulous computed tomography review and confirmation of the needle tip location by dynamic contrast-enhanced cone-beam computed tomography may be helpful. The procedure described herein is a relatively safe and attainable method of managing active bleeding from a small branching artery. However, it should be performed with caution because it depends on two-dimensional imaging for targeting, and inadvertent non-target injection could cause serious adverse events. The information provided in this case report might be of use for clinicians working in suboptimal conditions or in small angiography suites without a readily available selection of stent-grafts.
Footnotes
Author contributions
J.J. wrote the first draft of the manuscript. K.Y.L. contributed to the original concept of the study and provided the figures. S.K.K. and J.H.L. revised the manuscript. D.J.S. contributed to the original concept and conduction of the study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by our institutional review board (Institutional Review Board of Incheon St. Mary’s Hospital; OC19ZASI0147). Written informed consent for the procedure was obtained from the patient and her legal guardian.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.