
Abstract
Objective:
Occupational burnout has been documented among health care workers; however, there has been limited research investigating burnout among sonographers. The aim of this study was to measure burnout among a cohort of sonographers within New York City.
Materials and Methods:
70 participants completed a questionnaire online. The questionnaire comprised 2 sections: demographic questions and the Oldenburg Burnout Inventory (OLBI). The OLBI was used to assess 2 core dimensions of burnout: exhaustion and disengagement. The data were analyzed descriptively with frequencies, percentages, mean values, and standard deviations.
Results:
The majority (84.3%) of the participants worked in a hospital setting. A moderate to high burnout score was found for 81.4% of the participants. In the separate dimensions of burnout, 84.3% scored moderate to high on exhaustion, and 76.6% scored moderate to high on disengagement.
Conclusion:
Occupational burnout in health care settings is a serious problem with detrimental consequences. Most of this cohort of 70 sonographers working in New York City were experiencing a moderate to high level of burnout. Development of educational programs and interventions can be considered a potential solution for addressing prevention of sonographer burnout.
Research has shown that occupational burnout can affect a variety of working employees who experience an imbalance between their job demands and resources. 1 With regard to health care professionals, occupational burnout is a problem that can affect workers’ mental and physical health and have an impact on their job performance. 1
Occupational burnout is defined as a chronic response to prolonged stress on the job and has been recognized as an occupational hazard for various professions.1 –3 Burnout has been conceptualized as having 3 key dimensions: exhaustion, cynicism, and inefficacy. 1 Exhaustion is a loss of energy and feelings of fatigue. Cynicism is having negative attitudes toward clients, feelings of irritability, and withdrawal behaviors. Inefficacy is a sense of reduced personal accomplishment, lower productivity, and inability to cope. 1 Occupational burnout comes with a great cost to the individual, organization, and quality of patient care. In the United States, burnout is estimated to cost $125–$190 billion a year in health care spending, and correlates with negative feelings about patients and poor quality care.1,4 In a study conducted by Daughtery, 3 the Maslach Burnout Inventory (MBI) was used to determine the level of occupational burnout experienced by sonographers and vascular technologists, and to investigate whether there was a relationship between demographic characteristics or job-related variables and level of burnout. The study demonstrated that sonographers and vascular technologists experienced a moderate level of burnout, and a linear relationship existed between number of sonographic examinations performed per week and emotional exhaustion. 3 In a study of 107,122 health care workers who were surveyed over the course of 3 years (including during the coronavirus disease 2019 [COVID-19] pandemic), the researchers assessed the effect of the participants’ work on feelings of emotional exhaustion. 5 The Safety, Communication, Operational Reliability, and Engagement survey was used to assess emotional exhaustion. Participants included hospital-based health care workers in clinical and nonclinical (administrative support) roles at 76 community hospitals within 2 large United States health care systems. 5 Nursing was the most frequently reported occupational role (n = 43,918 [40.9%]). 5 Health care workers emotional exhaustion increased from 32% in 2019 to 40% in 2021. 5 The study demonstrated that emotional exhaustion among health care workers had increased since the pandemic, which could negatively affect the quality of patient care.
During the pandemic, sonography was increasingly used for patients presenting with a possible SARS-CoV-2 viral infection, and this diagnostic choice was made because sonography is noninvasive, cost-effective, and nonionizing.6 –8 Due to the increased incidence of patients developing deep vein thrombosis, pneumonia, and/or adult respiratory distress syndrome due to SARS-CoV-2 infections, venous sonography, echocardiograms, and lung sonograms were increasingly requested.6 –9 This increased sonographer workload was an added stressor to the stress from the high risk of viral exposure due to the close proximity of exams with infected patients. 8 While there are no available studies on sonographer’s occupational burnout for prepandemic comparison, one can assume that burnout would have increased postpandemic.
A review article explored sonographer’s occupational burnout and identified workload, training students and long hours, exposure and delivery of adverse news with no or ambiguous protocols of news delivery, and managing patient encounters as causes of burnout. 10 To date, most occupational burnout studies have focused on specific health care subgroups, including physicians, nurses, psychiatrists, and psychologists. However, few studies have investigated occupational burnout among clinical sonographers. The aim of this study was to ascertain the prevalence of burnout among sonographers working in the New York City (NYC) metropolitan area and propose possible interventions to reduce the risk of burnout.
Materials and Methods
This was a descriptive cross-sectional study in which data were collected using an online questionnaire that was developed with Qualtrics software (Qualtrics, Provo, UT). The questionnaire was designed to assess occupational burnout among sonographers in NYC. The sample included sonographers of different specialty areas. Institutional review board approval was obtained through the State University of New York (SUNY) Downstate Health Sciences University (IRB number: 1979566).
The Oldenburg Burnout Inventory (OLBI) was used to assess occupational burnout. The OLBI has been widely used and validated in different countries.11 –17 There are other tools to measure burnout, such as the Shirom-Melamed Burnout Scale, Copenhagen Burnout Inventory, and Maslach Burnout Inventory-General Survey (MBI-GS). 14 The first 2 instruments focus solely on exhaustion. The MBI-GS measures 3 dimensions of burnout, and the OLBI measures 2 dimensions. In a cross-sectional study of Romanian psychiatric residents, the OLBI provided a high scale of reliability pointing out a value of Cronbach’s alpha coefficient 0.814. 16 In another study of 232 Greek employees from different occupational groups, the factorial and convergent validity of the MBI-GS and OLBI were examined. 11 Confirmatory factor analysis supported the factor structure for both instruments, and convergent and discriminant validity was supported by the results of a multi-trait multi-method analysis. 11 The Cronbach’s alphas for the MBI-GS subscales were 0.80 for Exhaustion, 0.71 for Cynicism, and 0.79 for Professional Efficacy. The Cronbach’s alphas for the OLBI subscales were 0.73 for Exhaustion and 0.83 for Disengagement. 11 The MBI-GS is considered a 1-sided scale where all items are framed in 1 direction, whereas the OLBI includes both positively and negatively framed items. It has been suggested that the psychometric properties of the MBI-GS could be improved by adding positively phrased items. 11 Therefore, the OLBI was selected for use in this study. The measure consists of 16 items that assess the 2 core dimensions of burnout.
To broaden the reach of the survey, 2 methods of distribution were used: email and in-person distribution via a flyer with a Quick Response code. An email was sent to the clinical coordinators of workplaces that conducted diagnostic medical imaging. The research team also visited clinical sites and asked the supervisors for permission to distribute the flyers describing the study. To maintain confidentiality, no identifying information was required and an option of “prefer not to say” was provided for those who preferred not to disclose or answer certain demographic questions. The survey was conducted for 2 months. A brief introduction of the study and its purpose was included in the email and in the first page of the questionnaire. Voluntary participation in the study was emphasized in the introduction, and the completion of the questionnaire constituted consent. The questionnaires were evaluated for completeness, and invalid questionnaires were excluded from the analysis.
The questionnaire consisted of 2 sections. The first section included questions on demographic characteristics, including age, gender, place of employment (hospital, private practice, travel agency, etc.), type of employment (full-time, part-time, per diem, other-specify), number of years in sonography, work hours per week, type of registries held, and number of exams per shift. The demographic questions were for the purpose of describing the study sample; however, we were also interested in exploring whether any job-related characteristics were suggestive of burnout. The second section included the OLBI, which consists of 2 subscales: Exhaustion (8 items) and Disengagement (8 items). Items are responded to using a 4-point Likert scale where 1 = strongly agree, 2 = agree, 3 = disagree, and 4 = strongly disagree. Some items are reverse scored, and higher scores indicate a higher degree of burnout. Participants were categorized as having low, medium, or high burnout based on cutoff scores.
Statistical Analysis
The data were analyzed by calculating frequencies, percentages, means, and standard deviations. The Shapiro-Wilk test was used to test for normality.
Results
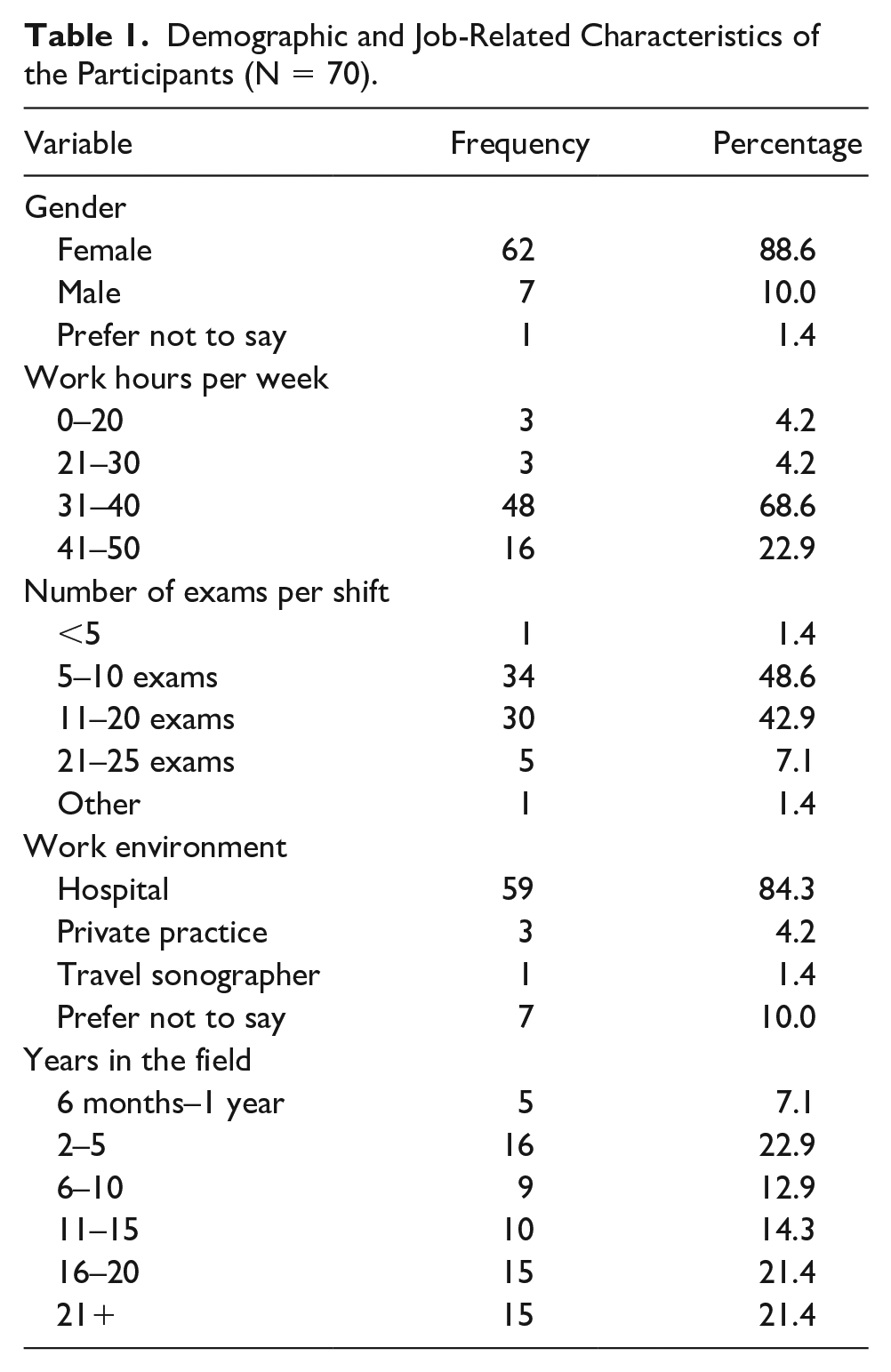
Ninety-two sonographers participated in the survey. However, there were only 70 participants who provided complete data on the questionnaire. Descriptive characteristics of those who completed the questionnaire are provided in Table 1. The majority of the participants were female (88.6%), worked in a hospital setting (84.3%), and worked more than 30 hours per week (91.5%). Half of the participants (50.0%) performed up to 10 sonographic examinations per work shift.
Demographic and Job-Related Characteristics of the Participants (N = 70).
The Shapiro-Wilk test using R programming (R v.4.0.4) indicated that the data distribution was not significantly different from a normal distribution (P = .31).
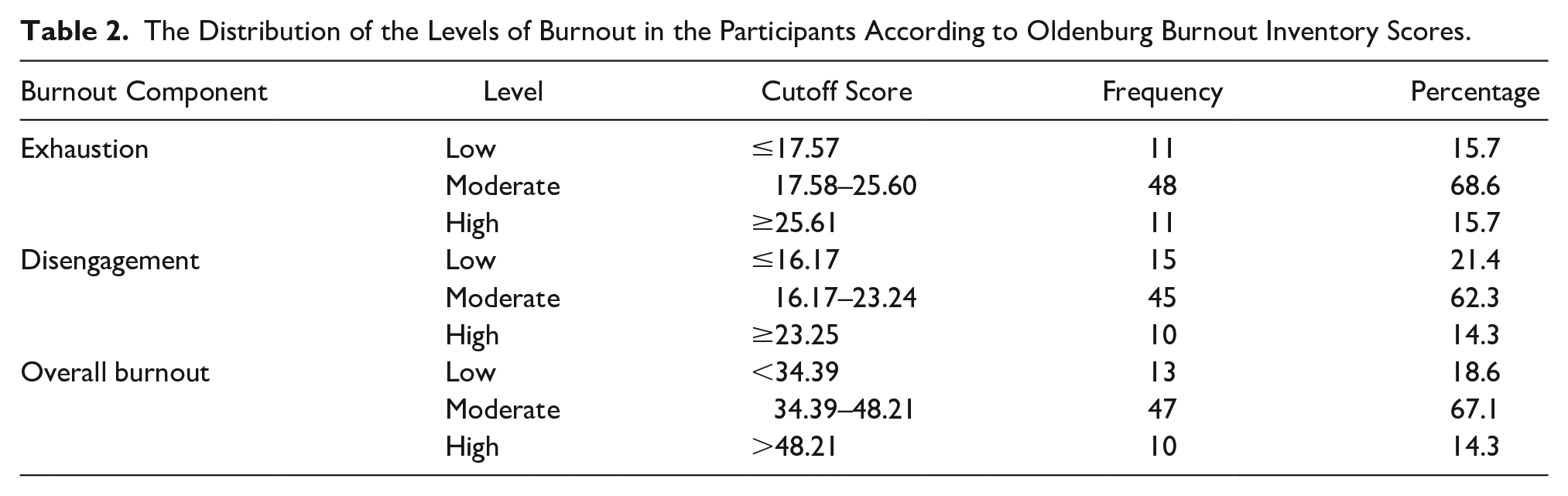
The mean score on the OLBI was 41.3 (SD = 6.9), which indicated the participants were experiencing a moderate level of occupational burnout. The mean scores for exhaustion (21.6, SD = 4.0) and disengagement (19.7, SD = 3.5) were also within the moderate range. Table 2 provides the distribution of the participants classified as experiencing a high, moderate, or low level of burnout based on the published cutoff scores for the total scale and 2 subscales. Although the occupational burnout scores were normally distributed, the scores indicated that more than 76% of the participants were experiencing moderate to high levels of overall burnout, exhaustion, or disengagement.
The Distribution of the Levels of Burnout in the Participants According to Oldenburg Burnout Inventory Scores.
Considering the impact of the recent pandemic, the participants were asked about the provision and use of mental health services. Fifty-two participants (74%) indicated that their employer offered mental health services (See Figure 1). However, among these 52 participants, only 3 individuals (5%) reported using mental health services.
The pie chart illustrates the percentage of participants who indicated that mental health services were provided by their employer.
Discussion
The COVID-19 pandemic has affected the physical and mental health of many individuals globally. The National Institutes of Health reported mental health during the recent pandemic as an urgent issue. 18 A systematic review revealed that hospital-based health care workers had declining mental health outcomes and identified work exposure to COVID-19 patients as a common contributor. 19 However, no studies have focused on the mental health of sonographers. Numerous factors contribute to the stress experienced among sonographers, including a heavy workload, long working hours, uncertainty around patient interactions, and physical and psychological safety, which only increased during the pandemic.6 –9,20 All of these factors could contribute to feelings of distress and occupational burnout, which could lead to poor job performance, medical errors, and poor patient care delivery.1 –4 Therefore, an evaluation of sonographers’ occupational burnout could be the first step toward reducing the risk of occupational burnout and improving their mental health and well-being.
The current study revealed that 81.4% of this cohort of NYC sonographers experienced a moderate to high level of occupational burnout. The high number of sonography examinations and long working hours (22.9% reported working more than 40 hours/week) could contribute to experiencing burnout, which has been reported in previous research linking an increased workload (high number of scans, long hours/overtime, small appointment times per exam) to sonographers’ occupational burnout.3,9
Regardless of the increased overall stress of health care workers during the COVID pandemic, 95% of the sonographers in the present study did not seek professional psychological help. In a poll conducted by the American College of Emergency Physicians (ACEP), 21 73% of emergency physicians felt there was a workplace stigma regarding seeking mental health services, and 27% reported avoiding mental health treatment for fear of professional repercussions. 21 It is unclear why the participants in the present study did not access mental health services; however, given the ACEP findings, it may be due to mental health stigma and a lack of awareness regarding how mental health services can mitigate stress and occupational burnout. Future research is needed to investigate these possibilities and to determine whether employees prefer to use mental health services outside the workplace.
For the prevention of burnout, mindfulness training is a program that could be implemented in classrooms and clinical settings for sonographers. In one study, 22 a 3-minute instructor-led mindful pause practice was introduced in sonography programs at 4 universities over the course of 2 semesters. The study reported a statistically significant increase in mindfulness and decrease in stress, and the majority of students reported having a positive experience and improved classroom attention and awareness. In another study, 23 a mindfulness and compassion-oriented meditation training program was designed to reduce stress and foster resilience. The program was evaluated for feasibility and effectiveness with a palliative care team. Twenty-eight staff members of an interdisciplinary palliative care team participated in a 10-week training program conducted at their workplace. Participants completed the Perceived Stress Questionnaire, Maslach Burnout Inventory, Somatization subscale of the Hopkins Symptoms Checklist–90-Revised, Emotion Regulation Skills Questionnaire, Hospital Anxiety and Depression Scale, and goal attainment scaling. Significant improvements were found in burnout related to emotional exhaustion and personal accomplishment. 23 In addition, overall perceived stress, as well as the worries, tension, and demands dimensions of stress, decreased after the intervention. Similarly, creating an education program that raises awareness of sonographers’ occupational burnout and designing it with interventions could be beneficial in coping with occupational burnout, as well as making a difference in their professional and personal lives. Skills learned in such programs can be used beyond work settings and ultimately improve overall well-being by reducing stress and tension and increasing mindfulness and resilience. The recent pandemic has highlighted the importance of building and improving health care workers’ resilience and well-being.
Limitations
A major limitation of this study is the descriptive cross-sectional research design. As such, the correlational and causal relationships between the variables were undetermined. A second limitation is the small sample size that included only sonographers in NYC. Therefore, there are limits to the generalizability of the findings to other populations of sonographers. Third, we were unable to calculate a response rate due to the use of both emails and flyers. Consequently, there is the possibility of a nonresponse bias. Lastly, because there were no national data available on sonographers’ occupational burnout postpandemic, it was not possible to determine if the sample in the present study were experiencing similar, higher, or lower levels of burnout experienced by sonographers in the United States.
Future Research Challenges
While the OLBI assesses self-reported occupational burnout, in a specific to work context, this remains a complex phenomenon that includes situational and individual factors. 17 Important situational factors that would need to be assessed are job, occupational, and organizational characteristics. Health care occupations have been shown to be more affected by occupational burnout. The organizational context is shaped by larger social, cultural, and economic forces, which, in this case, the pandemic acts as a major factor that needs to be considered. 17 In future studies, increasing the sample size, addressing the reasons behind long hours/overtime, and the lack of utilizing mental health services may further our understanding of sonographers’ occupational burnout, as well as inform solutions for sonographers’ well-being and work performance.
Conclusion
The results of this study demonstrated that there was a considerable amount of occupational burnout among this cohort of NYC sonographers, with 81.4% reporting a moderate to high level of burnout. Based on the responses of 70 participants, 22.9% worked overtime and 7.1% were performing 21 to 25 sonography examinations per work shift. These results underscore this cohort’s high workload and likely is linked to the 84.3% of the participants experiencing a moderate to high level of burnout due to exhaustion. These data are important because it suggests several factors that may contribute to sonographers’ occupational burnout and has implications for workplace interventions. Interventions such as resilience training, improving coping strategies, and mindfulness training could be incorporated in both academic and clinical settings.
Footnotes
Acknowledgements
The authors acknowledge SUNY Downstate Health Sciences University faculty member Rena Orman, PhD, Research Associate Professor for her invaluable contributions to this study. Also, authors acknowledge George Georgiev, PhD, for his contribution with data analysis. The authors thank Editage (![]() ) for English language editing.
) for English language editing.
Ethics Approval
Institutional review board approval was obtained through the State University of New York (SUNY) Downstate Health Sciences University (IRB number: 1979566).
Informed Consent
Voluntary participation in the study was emphasized in the introduction, and the completion of the questionnaire constituted consent.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.