
Abstract
A hemoventricle is a rare and life-threatening condition, characterized by blood accumulating in the brain ventricles. Computed tomography (CT) is commonly used in the diagnosis of hemoventricle. However, the use of CT is limited in the intensive care unit. This has prompted the exploration of alternative imaging techniques. Sonography offers a noninvasive, portable, and cost-effective option for assessing the ventricular system. A case study is presented of a 64-year-old female patient with a ruptured aneurysm who underwent endovascular coiling and the placement of an external ventricular drain. Point-of-care ultrasonography revealed ventricular dilatation that was associated with hyperechoic content and that was consistent with hemoventricle. The CT examination confirmed the diagnosis, and the patient received appropriate treatment. This case highlights the value of sonography as a complementary diagnostic imaging tool in situations where CT may be limited.
A hemoventricle is a rare and life-threatening condition in which blood accumulates in the brain’s ventricles. It can result from various causes, such as complications of intraparenchymal hematomas, and may lead to serious complications, including hydrocephalus and cerebral ischemia. 1 The diagnosis of hemoventricle is usually made with computed tomography (CT), but this technique has some limitations, especially in the intensive care unit (ICU). Sonography is an alternative diagnostic imaging technique that can assess the ventricular system of the brain. Sonography is noninvasive, portable, inexpensive, and accurate. 2
Case Report
A 64-year-old female, with no prior medical history, was admitted to a medical facility for a subarachnoid hemorrhage. It was caused by the rupture of a left posterior inferior cerebellar artery aneurysm. She underwent endovascular coiling of the aneurysm and placement of an external ventricular drain (EVD) for acute hydrocephalus, which was removed a few days later. The patient also required mechanical ventilation for respiratory failure and developed pneumonia that was treated with antibiotics. Several days after admission, the patient experienced a decline in consciousness. The use of point-of-care ultrasonography, in the ICU, serves as an extension of the physical examination and is the primary imaging assessment for critically ill patients, including the current case. The sonographic equipment utilized was a Sparq ultrasound equipment system (Philips Medical, Andover, MA) and a 2- to 4-MHz phased array transducer and a preset for transcranial Doppler studies. Applying grayscale imaging, through the transtemporal window, revealed dilatation of the lateral ventricles and the third ventricle, along with hyperechoic content within the left lateral ventricle and the third ventricle. This was diagnostically consistent with a hemoventricle (see Figure 1). A CT of the brain confirmed the diagnosis. The neurosurgery service performed EVD placement on the left ventricle, with drainage of bloody fluid. The patient developed super-refractory status epilepticus that was unresponsive to multiple antiepileptic and anesthetic drugs. The family requested no further invasive measures that ultimately lead to the patient’s death, a few days later.
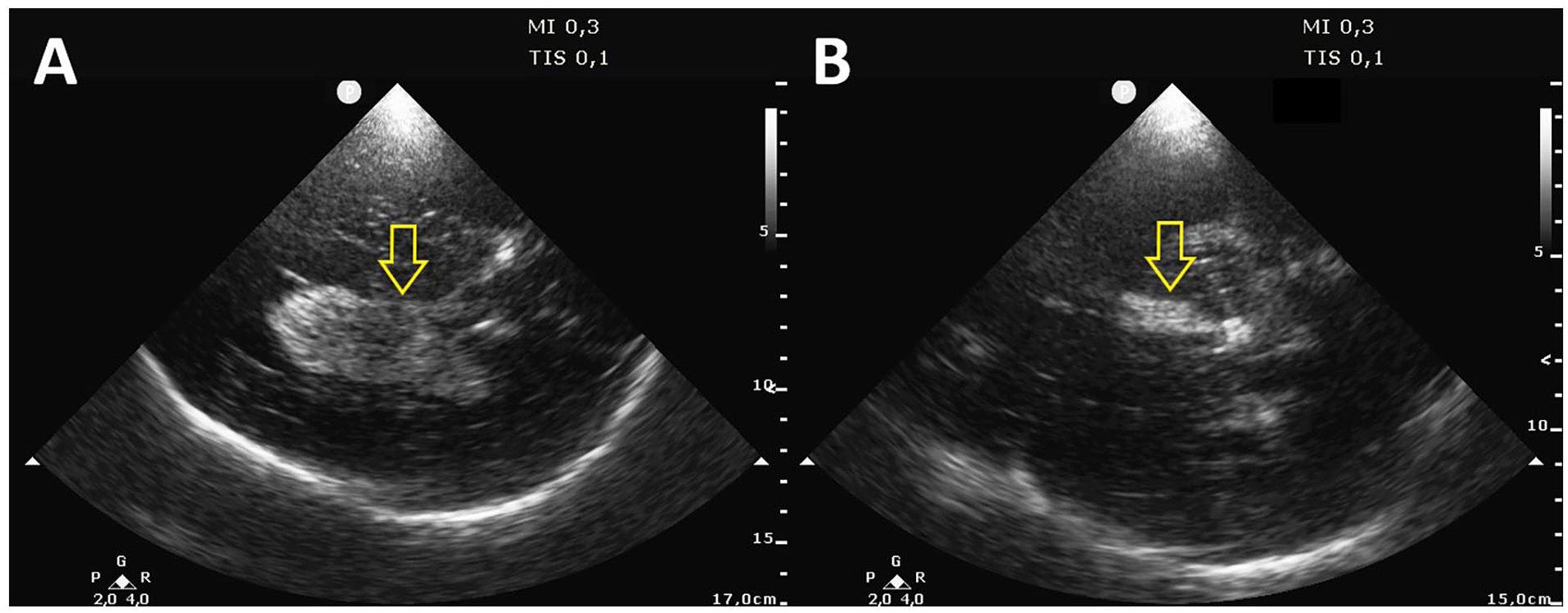
Transcranial sonographic image showing dilated lateral and third ventricles and a hyperechoic content filling the entire left lateral ventricle (A) and the third ventricle (B), consistent with hemoventricle.
Discussion
In regard to hemoventricles, it is important to note that approximately 70% of them are secondary in nature. These secondary cases are often discovered as complications of intraparenchymal hematomas (40%) or in conjunction with subarachnoid hemorrhage (10%). 3 It is essential to emphasize that secondary hemoventricles tend to have poor patient outcomes. Conversely, primary hemoventricles represent a rare form of hemorrhagic stroke confined to the ventricular system. They typically originate from an intraventricular source, with the choroid plexus being the usual suspect in such cases. 4 According to a study, the predominant causative factors were arterial hypertension, intraventricular arteriovenous malformation, Moyamoya disease, and intraventricular aneurysms. 5
Patients with hemoventricle are prone to developing secondary complications, such as hydrocephalus, cerebral ischemia, vasospasm, and poor long-term outcomes. 3 Due to its severity, the prompt diagnosis of hemoventricle holds vital diagnostic importance.
The preferred imaging technique used in diagnosing hemoventricle or other intracerebral hemorrhage pathologies is CT. It allows for pathology to be detected efficiently by detecting the blood within the ventricle, which appears as a hyperdense lesion (see Figure 2). Additional pathologies, such as, cerebral edema and hydrocephalus can also be identified through CT. 2 Although CT can be beneficial in the diagnosis of cerebral pathologies, it does have the limitations of radiation exposure, cost, and lack of easy accessibility.

A computed tomogram of the brain that displays a hemoventricle as a hyperdense lesion within the lateral ventricles.
Magnetic resonance imaging (MRI) is superior in detecting small intracranial hemorrhages, which can be challenging to diagnose with CT. Hemorrhage is best detected with gradient-echo T2 weighted sequences, where it appears as a hypointense lesion (see Figure 3). However, it is not recommended to routinely perform an MRI of the brain. The challenges lie in transporting the patient to the imaging suite and the extended imaging duration, which can make MRI impractical during the acute stage. 6
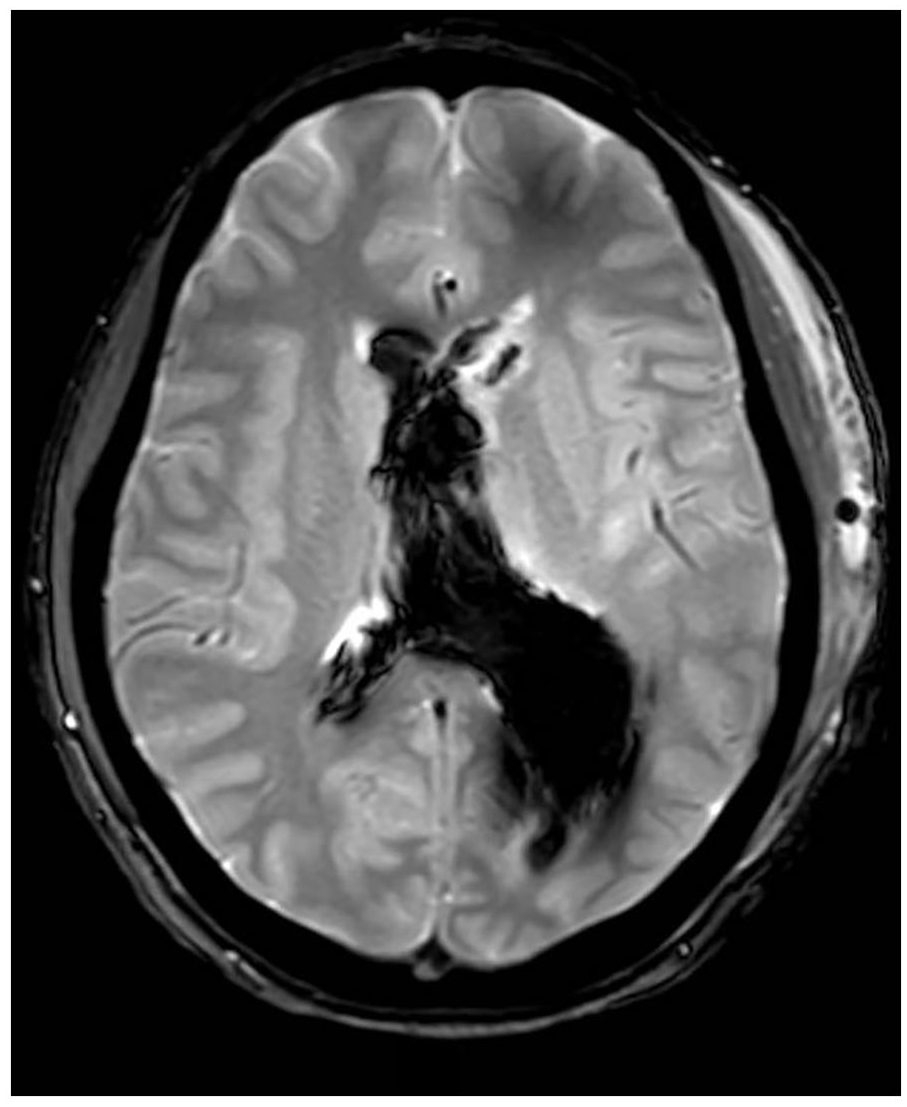
A magnetic resonance imaging view that was generated using a gradient-echo T2-weighted sequences. This image reveals a hemoventricle as a hypointense lesion within the lateral ventricles.
Sonography provides a noninvasive, portable, and cost-effective alternative that can be performed, at the bedside, by trained clinicians. It offers accurate real-time information regarding ventricular size, shape, and contents. In the presence of blood, sonography can detect a hyperechoic content partially or completely filling the ventricular cavity. 7 Nevertheless, sonography has its own limitations, including reliance on operator expertise, interobserver variability, technical challenges related to acoustic window, skull thickness, and artifacts, as well as limitations in visualizing all parts of the ventricular system.2,8
The optimal treatment approach for hemoventricle continues to be a subject of debate. While an EVD is recommended for managing acute hydrocephalus in patients with decreased consciousness, it is linked to relatively high rates of rebleeding, central nervous system infections, and catheter obstructions. Another therapeutic option for addressing obstructive acute hydrocephalus resulting from hemoventricle is the direct removal of the intraventricular clot through minicraniotomy. However, limited information is available regarding the outcomes associated with this particular surgical technique in hemoventricle cases.3,4
Conclusion
This case is an example of how sonography of the brain played a significant diagnostic role in the early detection of a hemoventricle, which was later confirmed by CT. This diagnostic process allowed for prompt surgical intervention, with the placement of an EVD. This case demonstrates that sonography of the brain can be considered a valuable diagnostic point-of-care tool and may be a first choice for diagnosing a hemoventricle that may have resulted from cerebral aneurysmal rupture.
Footnotes
Ethics Approval
Approval for this study was waived in accordance with the local regulations because this study is a case report of a single patient and did not include protected health information, data analysis, or testing of a hypothesis, and was de-identified.
Informed Consent
Written consent was obtained from the patient before the publication of this case report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.