
Abstract
Background:
POCUS is increasingly in utility and application across a variety of specialities. Although several professional societies, including the European Society of Intensive Care Medicine (ESICM) have recommended focussed Neurological ultrasound be a core competency, recommendations on how best to achieve this competency are lacking.
Aim:
The purpose of this systematic review was to assess what best-practice and evidence-based recommendations are available to achieve competency in Neurological Point-of-care ultrasound (NeuroPOCUS).
Methods:
We undertook a structured systematic review of publications and studies on the training of NeuroPOCUS for intensive care.
Results:
Our search strategy yielded a total of 4965 publications, reduced to 3551 following de-duplication. Despite this, only 28 publications were relevant following review of title and abstract and only 12 of these on full-text review. We identified three prospective studies, four consensus statements and five publications as posters and published abstracts. Structured analysis of these revealed minimal evidence-based teaching recommendations, and significant variability in teaching method.
Conclusion:
Compared to other modalities of POCUS (e.g. Cardiac and Lung), NeuroPOCUS lags behind with regards to utilisation and training in the general intensive care setting. Further work is needed to establish how this technique can be effectively taught and assessed for clinical application.
Keywords
Introduction
The use of clinical ultrasound has evolved far beyond the original confines of the radiology department. Point-of-care ultrasound (POCUS) imaging now has an established role across multiple clinical specialities in guiding real-time patient management, becoming progressively more distinct from traditional diagnostic imaging. Within critical care, POCUS use has dramatically increased, probably for the valuable real-time information it can provide in a critically ill patient. This, in turn, has led to the development of various competency frameworks to ensure clinicians are appropriately trained and working within a defined scope of practice.
Whilst the utility of cardiac, lung, and intra-abdominal POCUS is now well acknowledged in critical care, the role of brain- or Neuro-POCUS is still in its relative infancy. Modern advances mean imaging and Doppler technology can often be applied successfully in adults without the anatomical limitations associated with scanning through the skull. The use of concurrent B-mode, Transcranial Doppler (TCD), and Transcranial Colour-Coded Duplex assessment of structural components continues to evolve. Until recently, Neuro-POCUS had classically involved applying basic TCD screening methods to isolated pathologies encountered in Neurocritical care, such as aneurysmal subarachnoid haemorrhage. However, it has started to develop its own distinct and valuable role in general critical care and is no longer a skillset confined within Neurocritical care.
Guidelines from the American Society of Neuroimaging specify substantial prior ultrasound experience, at least 100 scans, and a test examination for a practitioner to become proficient. 1 Robba et al. 2 have defined an approach to developing Neuro-POCUS competencies in the critical care setting, stratified according to skill levels (ranging from basic, basic-plus to pre-advanced and advanced), based on the complexity of imaging techniques and analyses being performed.
Recent ESICM guidelines have included TCD of the middle cerebral artery (MCA) as a core competency for the general intensivist. 3 However, how best to achieve this competency is currently poorly defined compared to other POCUS modalities, which have a clearly described process for training and assessment. 4 For example, the UK critical care echocardiography programme mandates a face-to-face course followed by a period of supervised scanning with a recognised mentor, completion of a logbook of 50 scans of contemporary case-mix, and a formal assessment. 5 Such explicit requirements are lacking for Neuro-POCUS in critical care.
Also unlike other POCUS modalities, there are several perceived barriers to the use of Neuro-POCUS in the general critical care setting, for example, lack of expertise or lack of utility.
We conducted a systematic review of the published literature with the aim of identifying best practice and recommendations on the competencies (clinical utility) and how best to train colleagues in Neuro-POCUS.
Methods
To ascertain what current evidence was available on the delivery of training and competency assessment for Neuro-POCUS, we devised a structured electronic search strategy (see Supplemental Material for full details) and used it to search Medline and Embase via OVID, and CINAHL via Ebsco on 05/04/2024.
The returned papers were exported to the Rayyan systematic review platform, through which their titles and abstracts were screened for suitability against pre-defined inclusion and exclusion criteria. Inclusion criteria were any peer-reviewed published manuscript or consensus publication, involving brain ultrasound teaching and any staff group (including medical staff, nursing staff and/or allied health professionals). Publications were limited to critical care and emergency environments. There were no design restrictions.
Exclusion criteria were paediatric and neonatal studies due to anatomical and image acquisition process differences, rendering them non-applicable to adult populations. Non-neurological ultrasound papers were excluded. There were no set language restrictions, though the search strategy was only performed in English.
Screening was completed in duplicate by two blinded independent reviewers. Once all the papers had been screened, blinding was lifted and papers were included or excluded when consensus was present. In cases of discrepancy, the paper was re-reviewed and discussed by the two screening authors in order to reach a consensus. In the event of ongoing discrepancy, a third senior author reviewed and assessed the paper in question according to the pre-defined inclusion or exclusion criteria, with that decision taken as final. Full text copies of the selected papers were obtained and reviewed by a single author. Any paper excluded on full text review was re-assessed by two senior authors to ensure accuracy. The intervention was taken to be the teaching method used, and outcome as the paper’s own defined method of competency assessment; papers only pertaining to survey results were excluded. Using a structured teaching assessment table, data were systematically extracted using the key domains of assessment including competency definition, theoretical and practical assessment, and revalidation.
Results
A total of 4965 papers were identified using the above search strategy. After removal of duplicates, 3551 articles had their titles and abstracts screened against the pre-defined inclusion and exclusion criteria. Twenty eight articles were deemed potentially suitable for inclusion and their full texts were reviewed. Following this, a further 11 articles were subsequently removed as these did not involve teaching; one was excluded as it did not include neurological ultrasound; four were excluded as they included only audit or summary data. Twelve applicable publications were confirmed, consisting of three prospective studies and five published abstracts or posters (Figure 1, Table 1), and four consensus statements which will be considered separately. The majority of the prospective studies and abstracts/posters were published following workshops or courses. There was wide variability in terms of the structure of these publications and their associated courses.
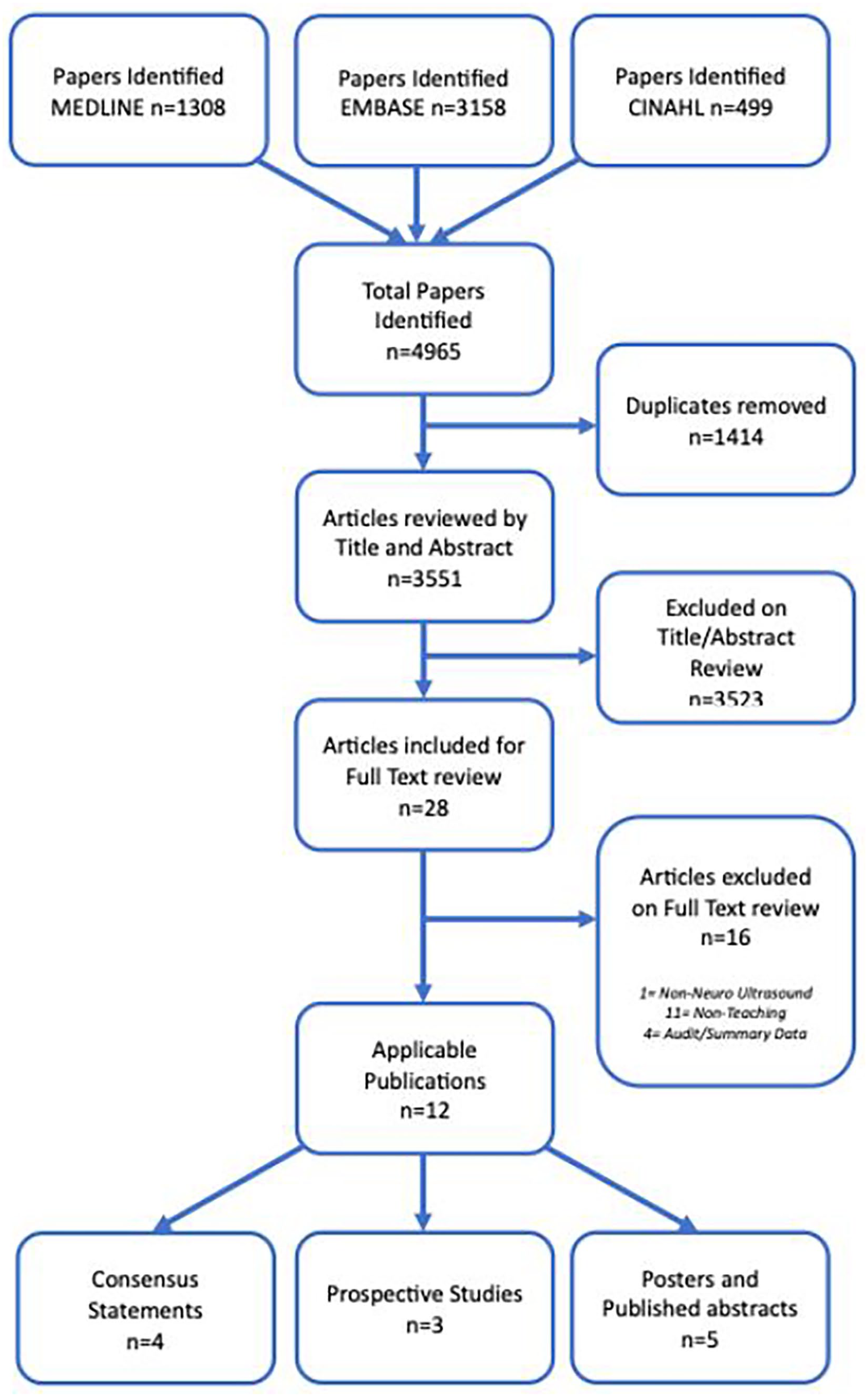
Consort diagram.
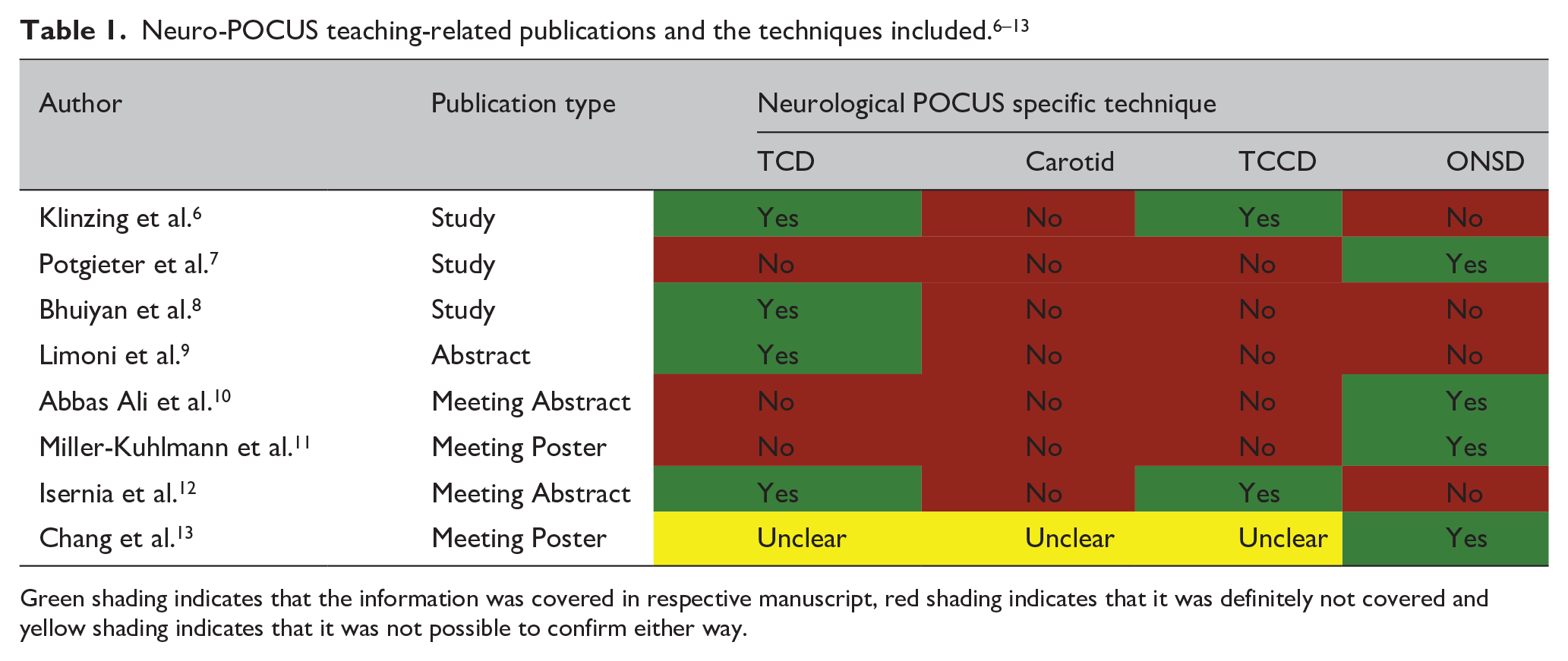
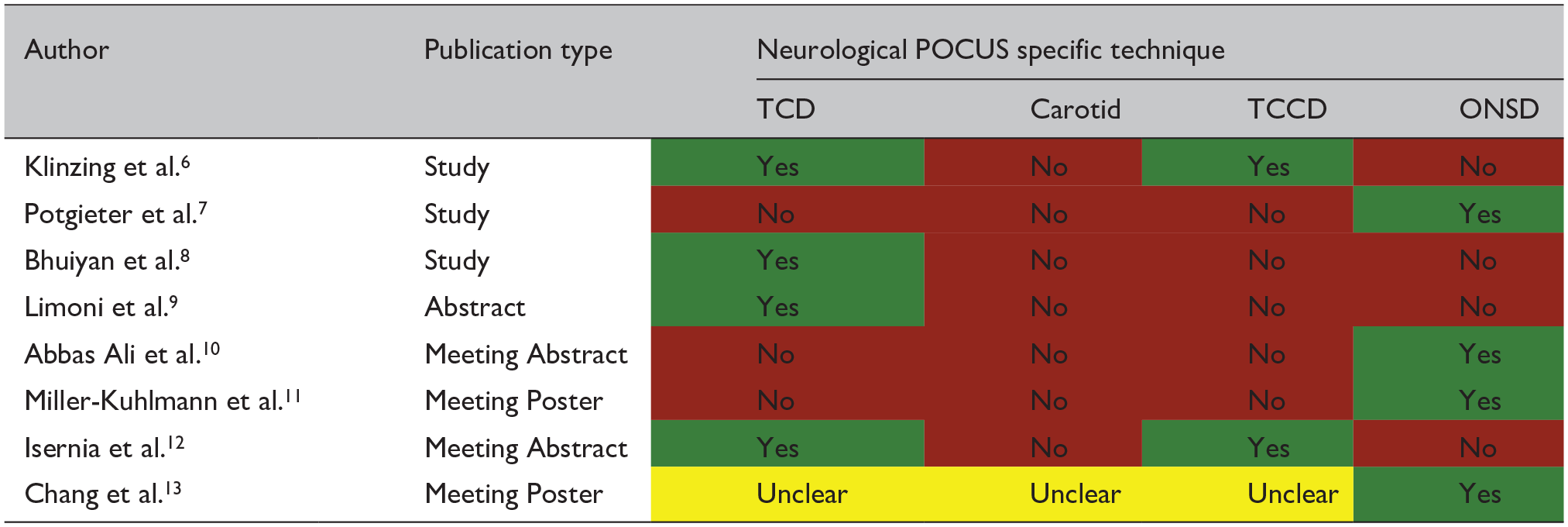
Green shading indicates that the information was covered in respective manuscript, red shading indicates that it was definitely not covered and yellow shading indicates that it was not possible to confirm either way.
Of the eight teaching-related publications, four included only Optic Nerve Sheath Diameter (ONSD) training.7,10,11,13 The remaining four involved TCD training,6,8,9,12 with two of these further incorporating TCCD in their training and/or assessment,6,12 although details on training and outcomes were frequently lacking in most of these. None of these publications mentioned carotid ultrasound.
Course structure and target audience
The majority of the teaching-related publications employed an initial course as part of the teaching (Table 2).6,7,9–13 There was notable variability in terms of the course structure and outcomes. Course duration ranged from 2 h to 6 days, but there was little specific detail about the courses themselves. Course participants came from a wide variety of backgrounds, consisting of medical students, physicians, neurosurgeons, nurses, advanced care practitioners, research scientists and intensivists.
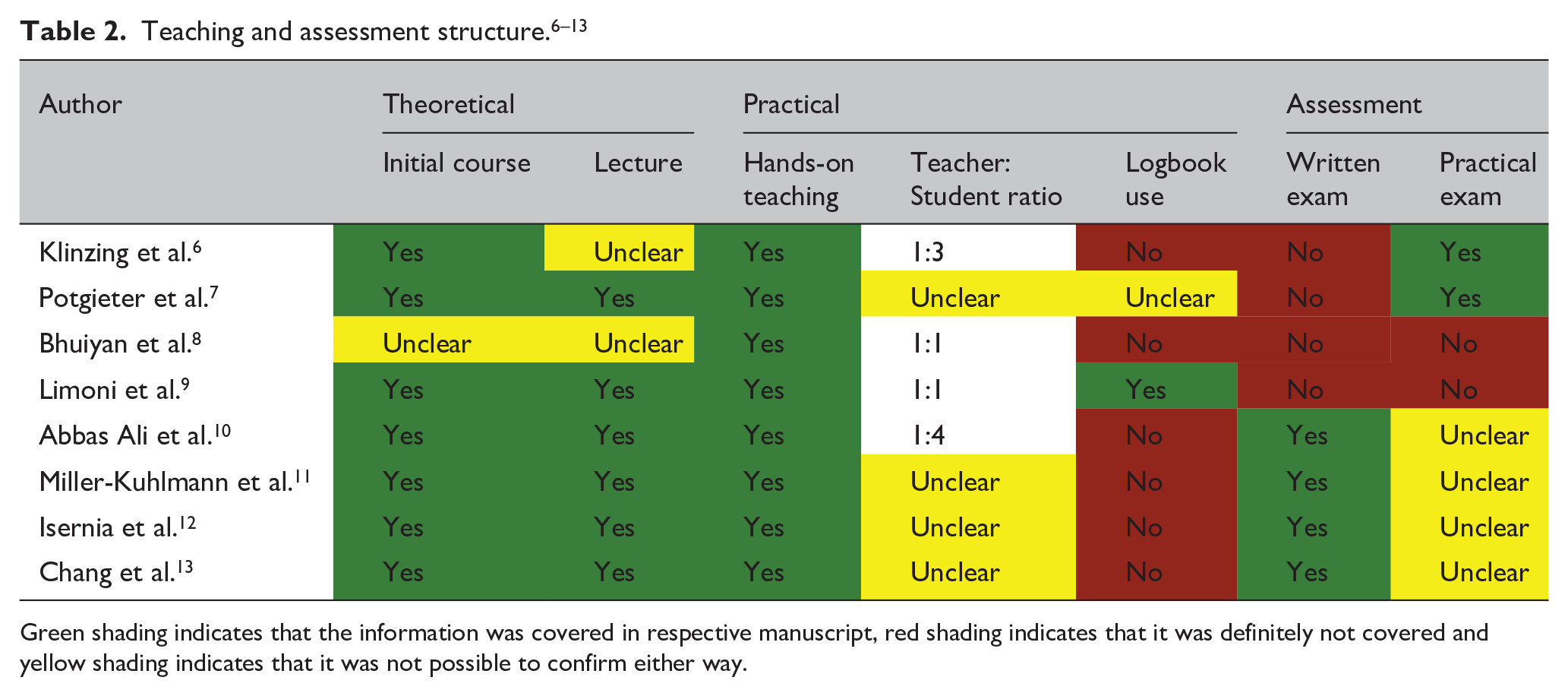
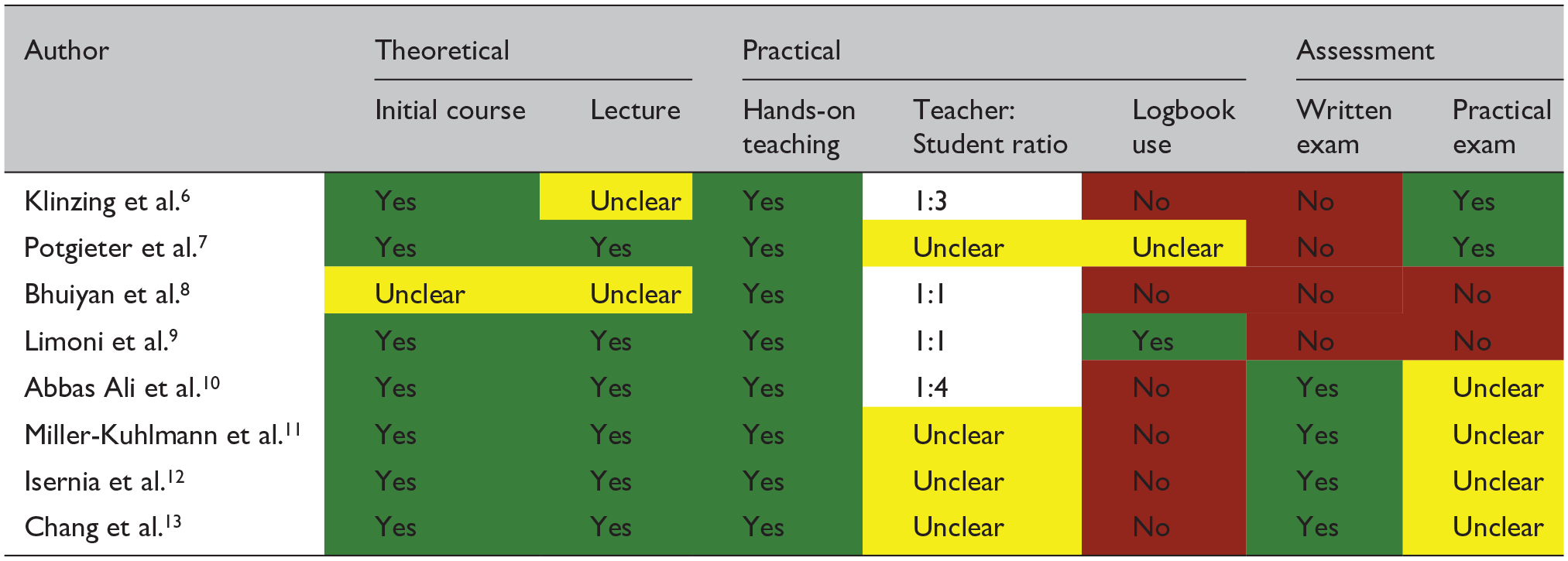
Green shading indicates that the information was covered in respective manuscript, red shading indicates that it was definitely not covered and yellow shading indicates that it was not possible to confirm either way.
Theoretical components
Apart from the study by Bhuiyan et al., 8 the theoretical teaching began with attendance at a didactic, face-to-face course, with six of these including a lecture component.7,9–13 No publication specified use of an online or e-learning teaching method, despite the increasing popularity of such a teaching format in modern medical education. Bhuiyan et al. 8 conducted a 6-day programme but did not mention an initial course or lecture in their publication. It was unclear as to whether or how theoretical knowledge was delivered in their programme, though potential alternatives to lectures could include pre-course reading material or face-to-face mentorship, etc.
Hands-on/practical components
All identified studies incorporated a hands-on teaching aspect; the ratio of lecture: hands-on time and total duration of the hands-on component were not specified, although the latter was often less than 6 h. The trainer: trainee ratio, where mentioned, varied from 1:1 to 1:4. Also of note was the marked variation in the way the experts or trainers had gained their experience. For example, Potgieter et al. 7 mentioned that ‘over a period of approximately one month, this group of “instructors” became sufficiently familiar’. Through the process of reviewing the full texts, it became apparent that in some cases, relatively minimal teaching was followed by swift progress to clinical application. As a notable extreme, one publication used an entirely untrained cohort for comparison. 8
Logbook and assessments
The use of a personal logbook was not specified in any of the teaching-related publications, though one study did require 100 supervised scans to be performed, taken to represent logbook equivalence. 9 Six of the eight teaching-related studies included an assessment component, of which two were practical, and four were written only (without mention of a practical assessment). Two studies did not describe any written or practical assessment, although one of these two was the aforementioned study that specified 100 supervised scans. All assessments were done in-house rather than through a national or centralised process.
Consensus statements
The literature search also identified four consensus or expert recommendation and opinion papers, two of which included Neuro-POCUS within a whole-body POCUS examination.2,3,14,15 The Brain ultrasonography consensus on skill recommendations and competence levels produced by Robba et al. 2 grouped both ONSD and aspects of structural imaging into the Basic Plus competency, in keeping with more modern clinical practice. Of note, the European Society of Intensive Care Medicine (ESICM) competencies omitted ONSD from their set of competencies. 3 No consensus document has specified methodology for competency assessment in Neuro-POCUS.
Discussion
Our systematic review has highlighted significant variation and gaps in Neuro-POCUS training internationally, supporting the findings from the international survey conducted by the European Society of Neurosonology and Cerebral Haemodynamics (ESNCH). 16
As with all other POCUS skillsets, competencies must be clearly defined before a Neuro-POCUS teaching programme can be developed. It is generally accepted that a comprehensive analysis of all the main vessels in the brain is beyond the scope of most general intensivists and neurointensivists. The approach, as described by Robba et al., which stratifies skill levels according to complexity of technique and image analysis, is in keeping with those used in other POCUS modalities such as cardiac ultrasound.2,5,17 Whilst multiple organisations and expert groups have made recommendations on competencies, specifics on how to achieve these competencies have been conspicuously absent.
Being a practical skill, Neuro-POCUS training needs to incorporate both theoretical and hands-on components. Most of the studies in this systematic review adopted a face-to-face, didactic lecture format for the theoretical component varying between 6 and 24 h in duration; the reason for such a wide range is unclear, but could be related to the characteristics of the target audience or content that is being taught.
With regards to the hands-on component, the duration, faculty:learner ratio, minimum number of supervised scans, logbook use and method of assessment were not clearly specified in most of the studies. Recommendations from specialist societies have specified that neurologists need to perform over 100 scans to become competent. 1 For intensivists looking to train in Neuro-POCUS, there are no equivalent recommendations at present.
Confirming the achievement of competencies usually involves some form of assessment – this was not clearly described in the majority of papers analysed. Assessment, being closely linked to accreditation and credentialing, has significant implications for the operational, legal, and ethical aspects of integrating Neuro-POCUS in the clinical environment.
The maintenance of competencies is a very important, yet often overlooked, component of most training and accreditation pathways. For example, the British Society of Echocardiography has an explicit process for revalidation after the initial acquisition of competency; this includes maintenance of a CPD diary and a recommended minimum number of scans. An equivalent process has not yet been defined for Neuro-POCUS.
The way forward
Whilst competencies in Neuro-POCUS have now been defined by professional organisations, details on the processes for developing these competencies are still lacking.
There is a need for clear, evidence-based practice so that robust and sustainable educational pathways and platforms can be developed to support intensivists who wish to acquire this skillset.
It is also pertinent to recognise that the way we learn and teach has evolved considerably beyond the ‘classroom’ through the use of online platforms. Social media platforms such as YouTube and other online repositories have altered the way we access and consume new information. Indeed, courses from various organisations are increasingly being delivered in a hybrid/blended format. These will have an impact on the learning process; at the very least, they are likely to reduce the amount of face-to-face interaction which is an important part of skills mentorship.
Equally, recent technological advancements have meant that handheld ultrasound devices with telementoring capabilities are becoming commonplace. This has directly improved accessibility to ultrasound for clinicians in geographically remote and/or resource-limited settings, though its impact on the learning process is yet to be quantified. Similarly, any effects related to the increasing use of machine learning/artificial intelligence for operator guidance and image interpretation are unknown.
These new opportunities which facilitate the training of larger and remote cohorts of clinicians present their own unique set of challenges, including the difficulties encountered in maintaining adequate distance supervision, scan governance and other quality/safety issues.
Conclusion
Our systematic review has shown that there is significant variation in practice and a lack of guidance and evidence on how best to deliver training and assess competencies in Neuro-POCUS for intensivists. This evidence gap is despite multiple bodies actively encouraging its use in critical care. Future work should address these issues with special focus on a set of high-quality, feasible, evidence-based recommendations on the delivery of training.
Supplemental Material
sj-docx-1-inc-10.1177_17511437251326744 – Supplemental material for Point-of-care ultrasound of the brain: A systematic review of competencies and training frameworks for intensivists
Supplemental material, sj-docx-1-inc-10.1177_17511437251326744 for Point-of-care ultrasound of the brain: A systematic review of competencies and training frameworks for intensivists by Adrian Wong, Richard Cashmore, Nurul Liana Roslan, Nourhan Ahmed, Mohamed Ibrahim, Isla Kuhn and Masumi Tanaka Gutiez in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A. Wong has received honoraria for the delivery of educational material from GE Healthcare and Mindray. These relationships have been disclosed to the journal and are being reported in the interest of transparency.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.