
Abstract
This case study describes a 13-year-old male who presented with ventricular fibrillation and pulseless ventricular tachycardia (VT) that occurred during football practice. An echocardiogram showed severely diminished biventricular function with an ejection fraction (EF) of 23% and an anomalous left main coronary artery from the right sinus with an apical echogenic mass of 1.2 cm × 1.2 cm, believed to be a thrombus. The patient underwent unroofing of the left main coronary artery. He was discharged on lisinopril, aspirin, and metoprolol, and a follow-up echocardiogram 79 days after discharge showed improved EF of 51% and resolution of the apical thrombus. It is crucial to remember that postsurgical approaches may still present challenges even after the initial repair or intervention. It is important to remain vigilant and aware of any potential issues that may arise as they can have significant impact on the overall success of the procedure.
Keywords
Practitioners face many challenges with anomalous origin of a left coronary artery (CA). Anomalous origin of a left CA can be associated with cardiac arrest, which can be particularly devastating in young athletes 1 in whom sports activities can induce ischemia and life-threatening arrhythmias. 2 Examples of a normal left main CA and normal right CA are provided (see Figures 1 and 2).
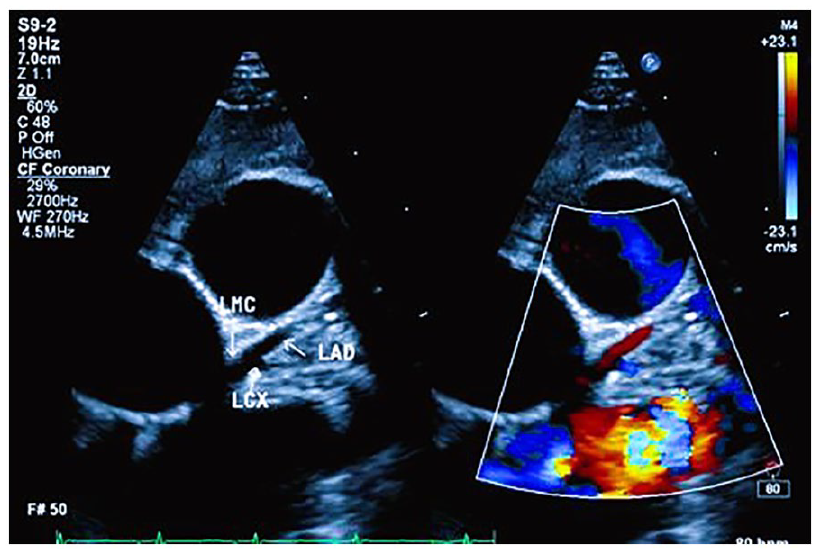
The parasternal short-axis view, with slight clockwise rotation, reveals the left main coronary artery (LMCA), proximal left anterior descending artery (LAD), and proximal left circumflex coronary artery (LCX). Color Doppler imaging, when applied, confirms a normal blood flow pattern, further supporting the overall assessment.
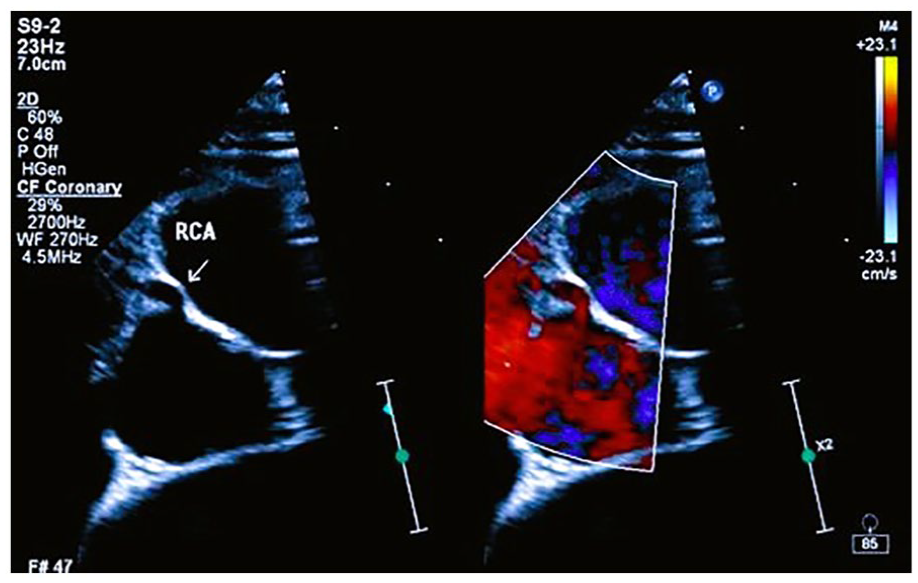
The parasternal short-axis view, with slight clockwise rotation, reveals the course of the right coronary artery (RCA) in relation to the anterior and right structures and its proximity to the aorta. Color Doppler imaging adds valuable information about blood flow patterns within the RCA.
Diagnosing patients may be difficult because children and adolescents are often asymptomatic, and the initial presentation may be sudden cardiac arrest or sudden death. 3 Coronary artery origin from the wrong sinus of Valsalva is the second most common cause of sudden death on the athletic field in the United States. 4 In these patients, exercise produces myocardial ischemia and sudden cardiac death. 5
Case Study
The patient was a 13-year-old male previously healthy who presented with sudden cardiac arrest during football practice. There is a significant family history of myocardial infarction on the paternal side. The patient’s grandfather suffered a myocardial infarction at the young age of 40 years old and died 10 years later, due to a second myocardial infarction. In addition, three paternal aunts died in their late fifties due to heart disease, although the specific cause was unknown.
When the patient collapsed, cardiopulmonary resuscitation (CPR) was initiated by bystanders within 1 minute of collapse and continued for 4 minutes until emergency medical services arrived at the scene. When the paramedics arrived, the patient was in ventricular fibrillation. He was defibrillated with 125 Joules and was transported to the local emergency department. Upon arrival at the hospital, the patient was in pulseless ventricular tachycardia (VT). Cardiopulmonary resuscitation was reinitiated, and he was successfully cardioverted with 300 Joules. Due to continued runs of VT, amiodarone was initiated. The echocardiogram showed normal ventricular wall thickness with severely diminished biventricular function, with a left ventricular (LV) ejection fraction (EF) of 23% (see Figure 3 and Supplemental QR code for videos 3.1–3.3).
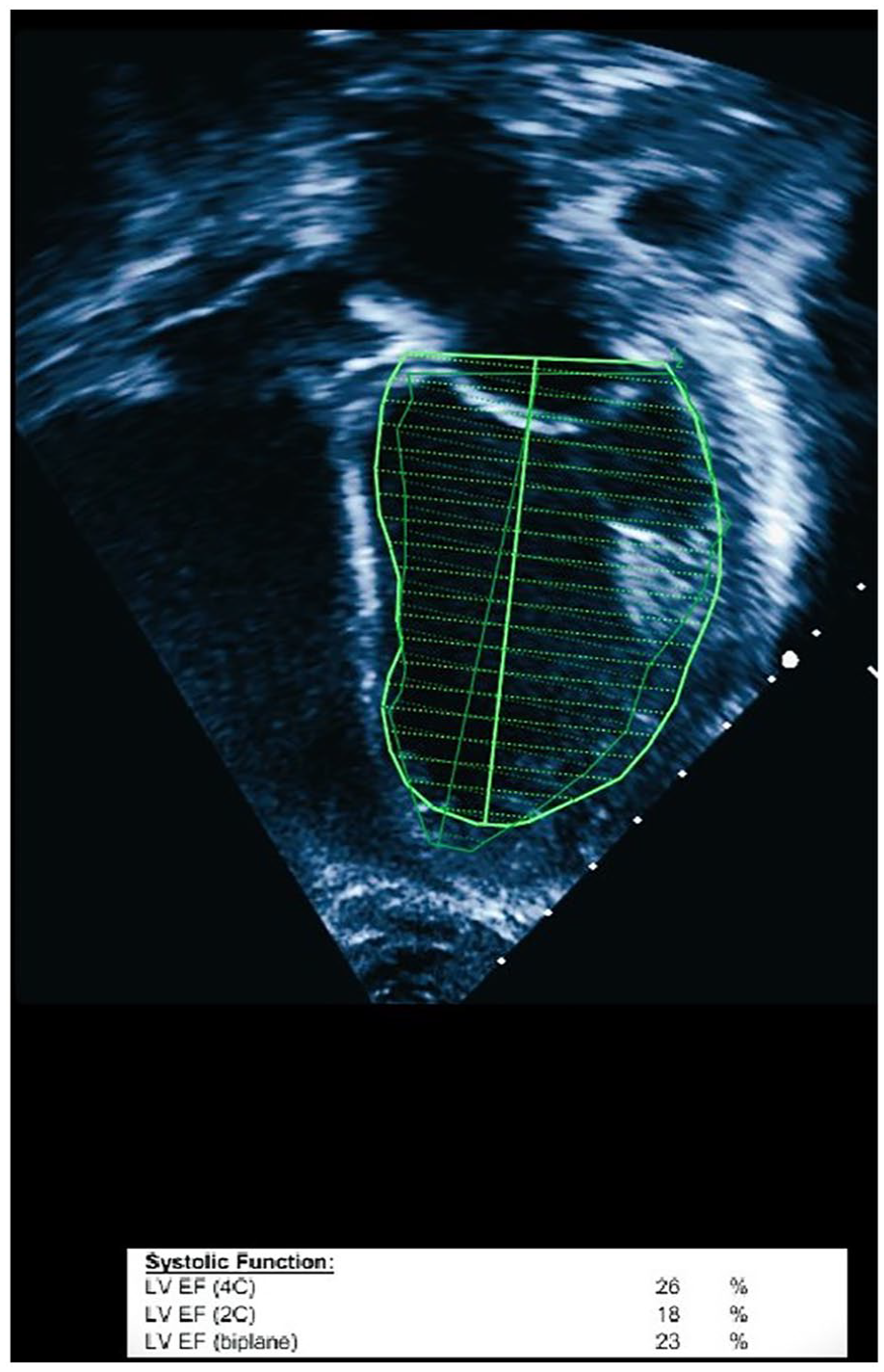
In the apical four-chamber view, a 2D echocardiogram was performed on the patient. The results revealed severely diminished cardiac function, as measured by the Simpson method, with an ejection fraction (EF) of 23%. EF, ejection fraction; LV, left ventricular.
The patient had another short run of VT followed with hypotension. Chest compressions were administered for 2 minutes, followed by an epinephrine bolus. Sinus rhythm was restored, but due to hemodynamic instability, the patient was placed on venoarterial (VA) extracorporeal membrane oxygenation (VA ECMO).
A transesophageal echocardiogram during cannulation revealed an anomalous left main CA from the right sinus. It also showed a severely depressed LV function with EF of 15%, LV (Global Longitudinal Strain [GSL]) = −2.8% (see Figure 4A). A postcannulation transthoracic echocardiogram showed Doppler flow aliasing through a 9-mm interarterial course (IAC), suggestive of CA compression. Pulse-wave Doppler of the coronary diastolic flow velocity is seen in Figure 4B (see Figure 5 and Supplemental QR code for video 5A). It is important to note that the patient had been on VA extracorporeal membrane oxygenation (ECMO), for a total of 5 days. A computed tomographic angiogram (CTA) was later performed before surgery to confirm echocardiogram findings (see Figure 6A and B).
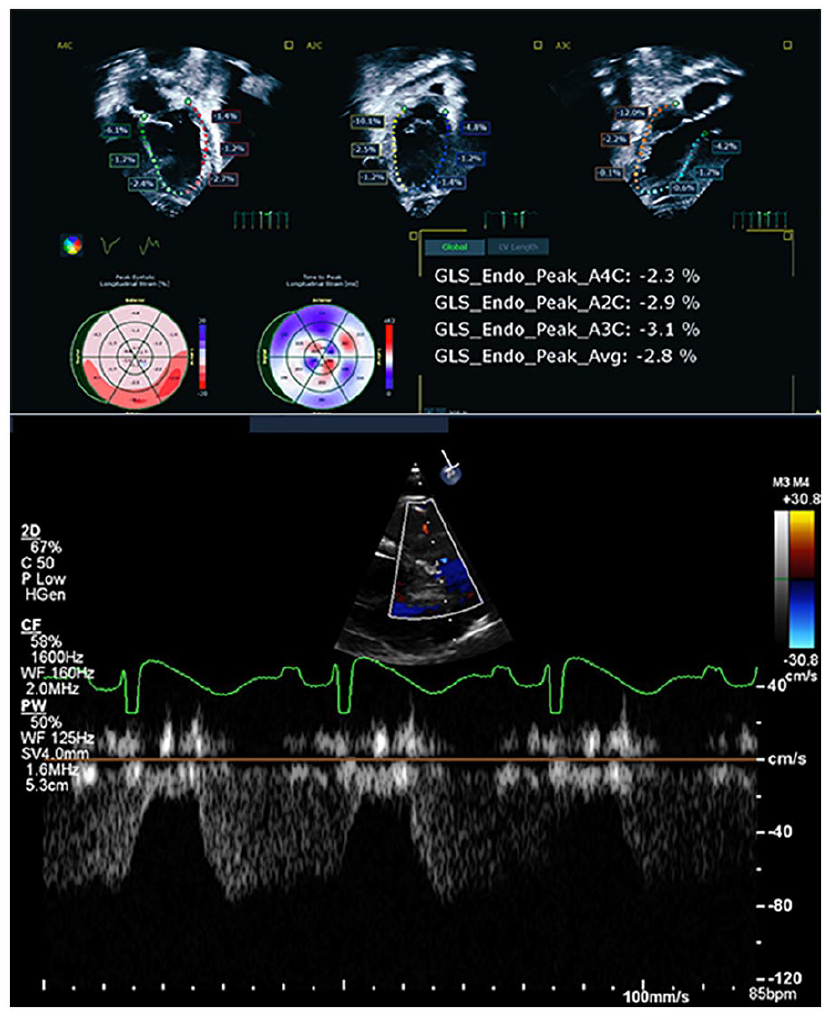
(A) The image was obtained during (Pre-OP) which highlights Global Longitudinal Strain (GLS) of −2.8% strain. (B) Pulse-wave (PW) Doppler tracing of coronary diastolic flow velocity.
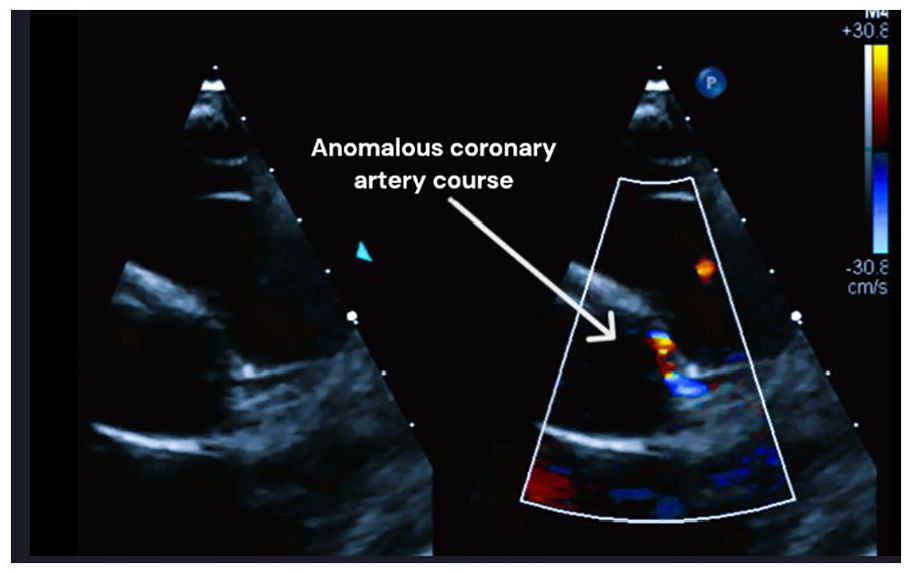
The image, obtained using the parasternal short-axis view with slight clockwise rotation, reveals an anomalous origin of the left main coronary artery (LMCA) from the right aortic sinus of Valsalva. The LMCA takes an intramural and interarterial course. Color Doppler imaging confirms abnormal flow patterns with aliasing velocities. Image obtained (Pre-OP).
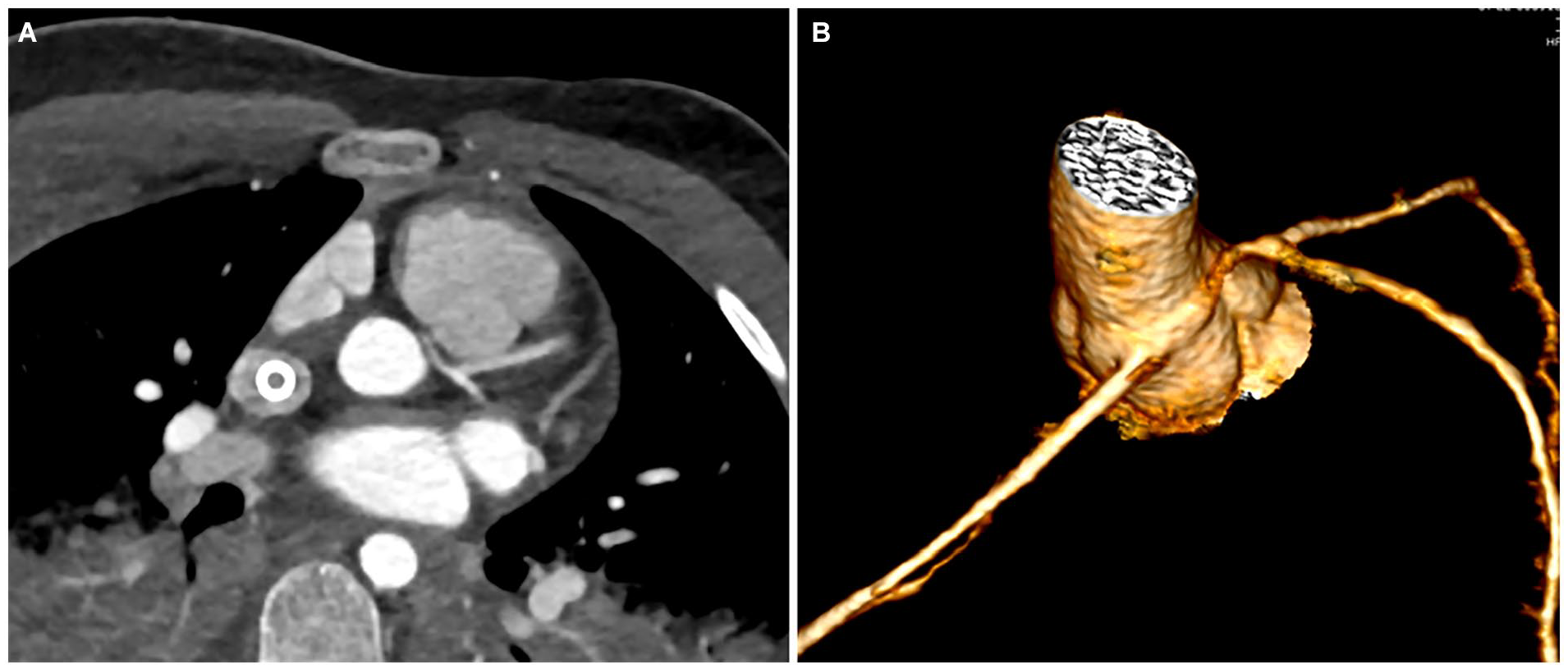
(A) An image of a computed tomographic angiography (CTA) which was performed to evaluate coronaries. (B) A 3D volume rendering image provides a more comprehensive and detailed understanding of coronary anatomy.
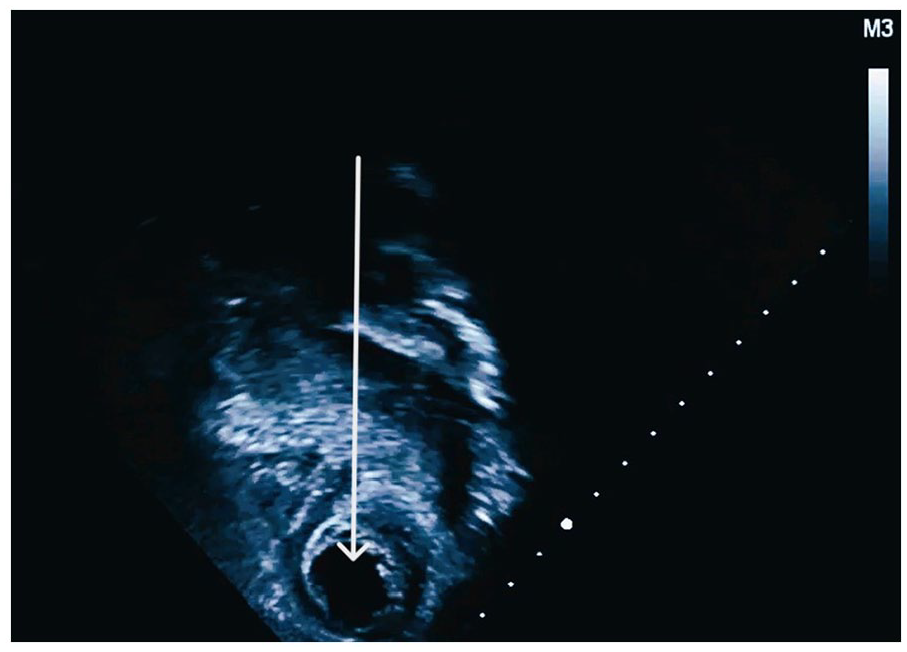
The patient then underwent unroofing of the left main CA (see Figure 7 and Supplemental QR code video 7A). A predischarge echocardiogram showed apical akinesis and a 1.2 cm × 1.2 cm apical mass/thrombus (see Figure 8 and Supplemental QR code for video 8A), which was treated before discharge with a bivalirudin drip. A follow-up echocardiogram was done 6 days after initial discovery showed resolution of LV thrombus (see Figure 9 and Supplemental QR code for video 9A). After a total of 31 days of hospitalization, the patient was discharged on lisinopril 5 mg, taken once a day (QD), aspirin 81 mg taken twice a day (BID), and metoprolol 25 mg QD. Seventy-nine days after discharge, an outpatient echocardiogram showed an LV EF 51% and a GLS of −15.1% (see Figures 10 and 11 as well as the Supplemental QR code for videos 10A and 11A–C).
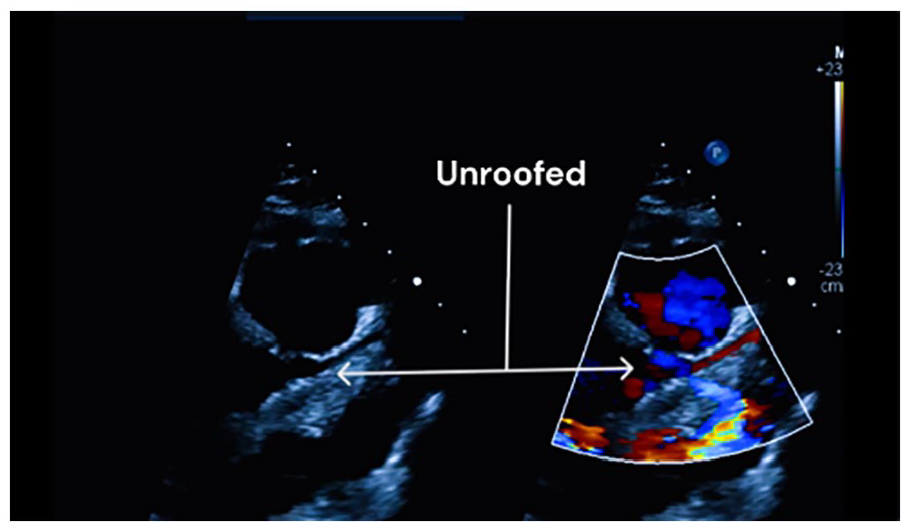
The image was obtained using the parasternal short-axis view with slight clockwise rotation. It shows improved color flow demonstrated by color Doppler imaging post unroofed coronary.
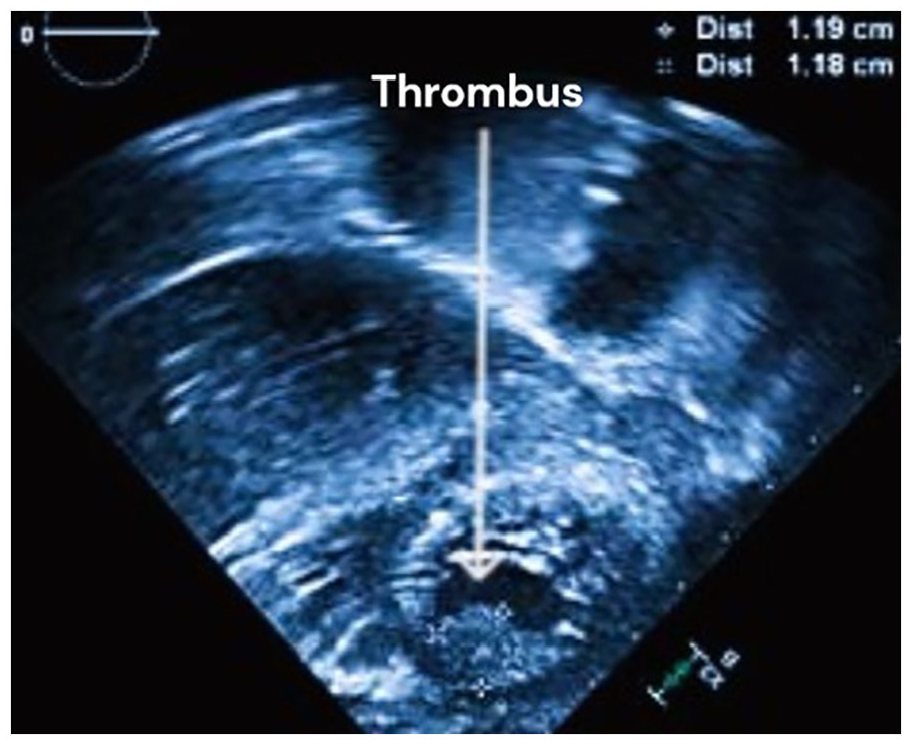
The static image obtained postoperatively (Post-Op) of the apical four-chamber sweep provides a precise visual representation of a thrombus, offering valuable insights into thrombus formation in cardiac imaging.
The static image obtained postoperatively (Post-Op) of the apical four-chamber sweep provides a precise visual of the dissolved thrombus.
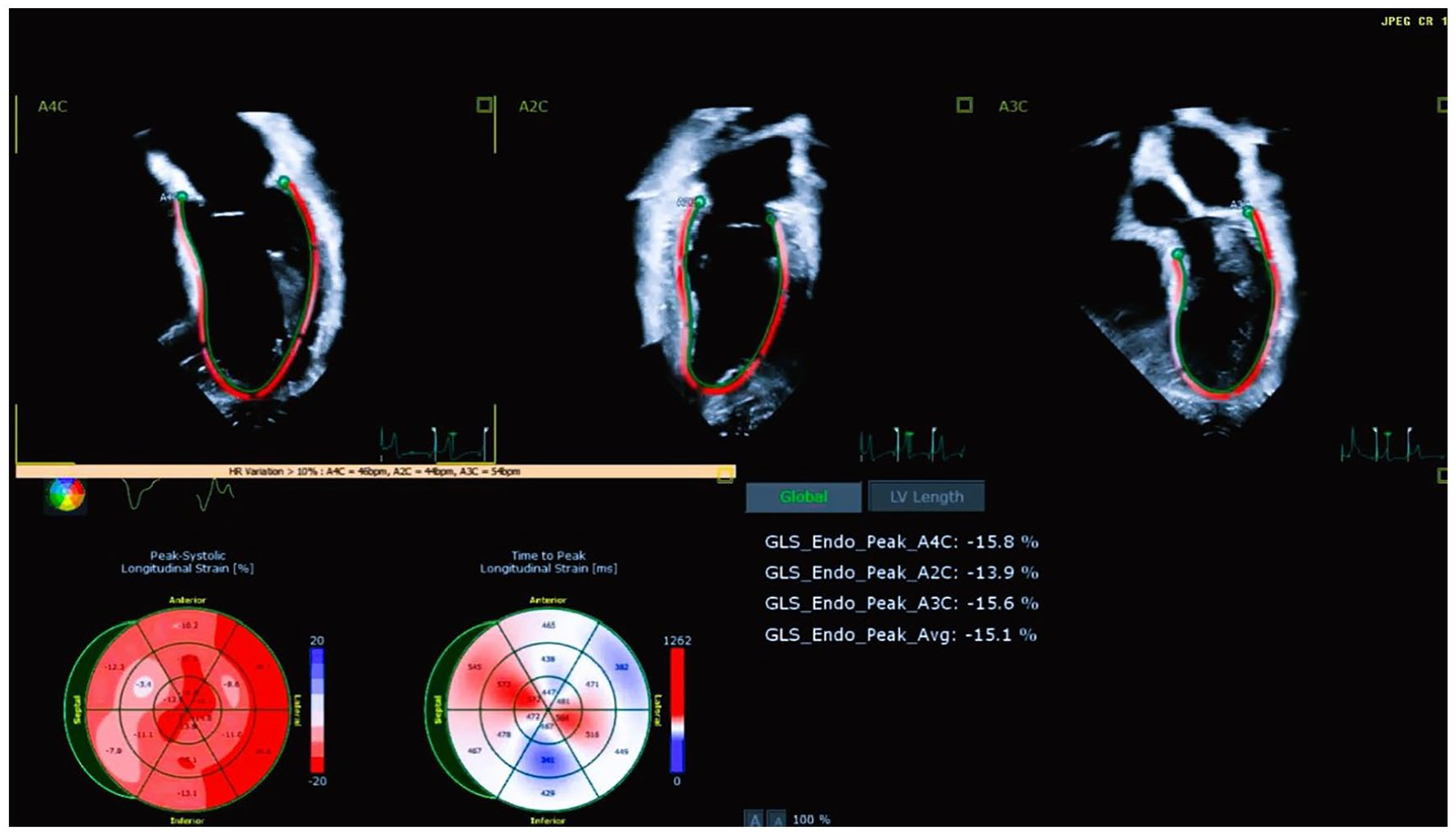
The image obtained postoperatively (Post-Op) highlights an improved Global Longitudinal Strain (GLS) of 15% strain.
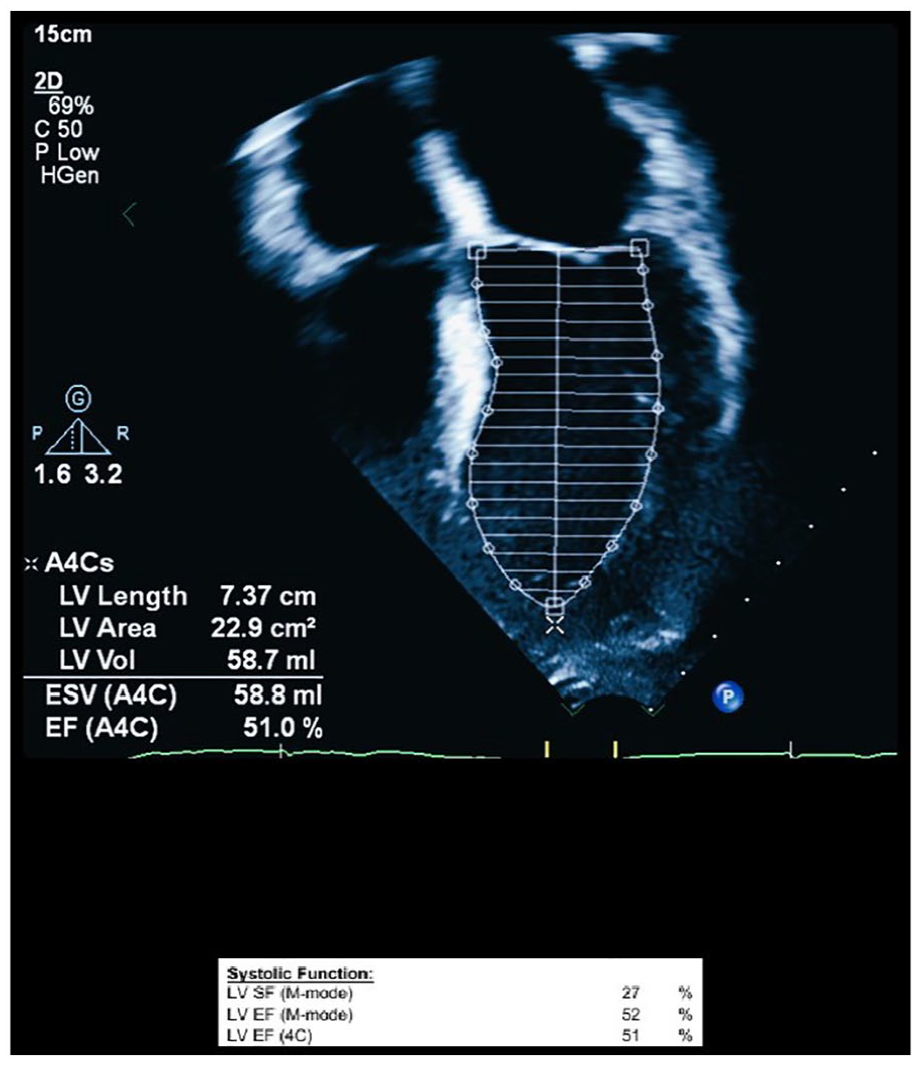
In the apical four-chamber view, a 2D echocardiogram was performed on the patient. The results revealed significantly improved cardiac function, as measured by the Simpson method, with an ejection fraction (EF) of 51%. LV, left ventricular.
Discussion
Anomalous origin of a CA is a rare congenital abnormality associated with myocardial ischemia and sudden cardiac death,6,7 Anomalous origin of the left CA arising from the right sinus (ALCA) with an IAC becomes dangerous during physical activity. As the heart rate increases, the aorta and pulmonary artery increase in diameter as they accommodate to an increased stroke volume. The anomalous coronary artery becomes squeezed, thereby creating an obstruction at the time of highest myocardial oxygen demand. The etiology of sudden death in individuals with ALCA is commonly associated with ventricular arrhythmias from myocardial ischemia during or following strenuous activity. This can be aggravated by proximal vessel narrowing, ostial stenosis, or having the anomalous CA an acute angle.8 –10
The American Heart Association and American College of Cardiology Scientific Statement differentiates between the much higher-risk left anomalous coronary arteries (L-ACAOS) with IAC and the lower-risk right anomalous coronary arteries (R-ACAOS) with an arterial course (AC) and states that those with R-ACAOS who are asymptomatic can return to competitive sports after exclusion of ischemia. However, the risk of sudden cardiac death in patients with anomalous coronary artery origin cannot be eliminated, and careful evaluation and management are necessary.11 –13
In this patient, the diagnosis of anomalous left main coronary artery from the right sinus was made during his hospitalization, and unroofing of the left main coronary artery was performed to alleviate the obstruction and prevent further myocardial ischemia. One surgical technique used to address anomalous coronary arteries is known as “unroofing.” During this procedure, the surgeon carefully removes the tissue that covers or compresses the abnormal coronary artery. By doing so, the artery is given a clearer and unobstructed path for blood flow. The primary goal of unroofing is to enhance perfusion to the heart muscle, known as the myocardium, and reduce the risk of complications that can arise from restricted blood flow.
Unroofing surgery for anomalous aortic origin of a coronary artery (AAOCA) alters coronary anatomy by opening the intramural segment so that the anomalous coronary orifice arises perpendicularly from appropriate aortic sinus. Computational fluid dynamics modeling (CFD) allows for quantification of hemodynamics linked to morbidity such as wall shear stress (WSS), relative to patient-specific features like the angle of origin (AO). 14
By removing the tissue that hinders proper blood flow, unroofing aims to improve the delivery of oxygen and nutrients to the heart muscle. This can help alleviate symptoms and reduce the risk of complications associated with inadequate blood supply to the myocardium.
It is important to note that the specific details of the unroofing procedure may vary depending on the individual case and the surgeon’s approach. Consulting with a qualified health care professional will provide more personalized and accurate information.
The patient was discharged on lisinopril, aspirin, and metoprolol, which are commonly used medications for the management of heart failure and prevention of recurrent myocardial infarction. The follow-up echocardiogram showed a marked improvement in LV function and resolution of the LV thrombus, indicating successful management of the patient’s condition.
Conclusion
Anomalous origin of a coronary artery is a rare congenital abnormality associated with myocardial ischemia and sudden cardiac death. Careful evaluation and management are necessary to prevent adverse outcomes in affected individuals. The case presented highlights the importance of prompt diagnosis and management of anomalous coronary artery origin in young athletes to prevent sudden cardiac death.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793231200192 – Supplemental material for The Importance of Cardiac Prescreening: A Case Report of Cardiac Arrest in a Teen Athlete
Supplemental material, sj-docx-1-jdm-10.1177_87564793231200192 for The Importance of Cardiac Prescreening: A Case Report of Cardiac Arrest in a Teen Athlete by Jose Luis Bastida and Maria S. Horenstein in Journal of Diagnostic Medical Sonography
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because The information provided is for medical and educational purposes.
Informed Consent
Informed consent was not sought for this study because all case data were deidentified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.