
Abstract
Objective:
Laboratory accreditation has been shown to impact variability and completeness. However, little data exist demonstrating the impact of personnel credentialing on completeness and efficiency. Therefore, the aim of this study was to evaluate exam completeness and efficiency among staff with an advanced cardiac sonographer (ACS) credential, Registered Diagnostic Cardiac Sonographer or Registered Cardiac Sonographer and noncredentialed staff.
Materials and Methods:
Retrospective review of adult and pediatric echocardiograms at eight facilities in three states. Exam completeness was compared with Intersocietal Accreditation Commission (IAC) standards and completeness by pathology was compared with the American Society of Echocardiography (ASE) standards.
Results:
This study was based on the review of 1147 patient cases. Of the cases reviewed, 60.3% were performed by credentialed (non-ACS) sonographers, 28.3% were completed by credentialed ACS, and 11.3% by noncredentialed staff. The credentialed staff completed exams ≤ 12 hours. The exams were reviewed for compliance with IAC standards and completed by ACS staff: 80.0% in aortic stenosis and 55.6% in non-ACS staff. Those patient cases for mitral regurgitation (14/19) were 73.7% IAC compliant, cases completed by credentialed non-ACS (20/56) were 35.7% compliant, and those completed by noncredentialed sonographers (2/11) only 18.2% were compliant. Cases specific to patent ductus arteriosus were 92.1% compliant with IAC standards that were completed by ACS compared with 77.9% completed by non-ACS staff. Cases of pulmonary hypertension were also evaluated for IAC compliance and 61.8% met the standard with ASE versus 41.7% completed by non-ACS.
Conclusion:
Examinations performed by ACS are more often complete in important pathology. Examination efficiency is highest among credentialed sonographers.
Keywords
Early models of a clinical expert in an advanced practice role suggested demonstration of excellence in clinical practice, leadership, and teaching with advanced education in pharmacology, advanced pathophysiology, and clinical correlation and other core-level curriculum.1,2 Unlike early proposals of the ultrasound practitioner working autonomously, 3 the current day advanced cardiac sonographer (ACS) consistently works in partnership with physicians and other health care providers to enhance patient care, improve lab quality, and increase efficiency. Consistency in implementation of the concept has been advanced education, additional clinical training, and internship with the requirement of completion of a national credentialing examination.3,4 The ACS credential is a currently utilized by employers as both a qualification and separate position that has a specific job description and competencies.
Echocardiographic laboratory accreditation, through the Intersocietal Accreditation Commission (IAC), ensures performance of echocardiography at a benchmarked standard. The application process for IAC accreditation includes a thorough review process by a panel of medical experts of the facility, equipment, technical component, and interpretation completeness and timeliness. Although not mandated in cardiac care currently, lab accreditation has demonstrated improvement in report completeness and image quality compared with nonaccredited labs. 5 In addition, improvement in interpretation concordance, accuracy, and reproducibility impacts the accuracy of evaluating patients with valvular heart and congenital heart disease. The ACS student completes formal education in IAC preparedness, as part of their required curriculum. Having sonographers with advanced training may improve reporting efficiency while retaining senior sonographers, which provides additional career opportunities. 6 The aim of this research study was to evaluate the improvement in patient examination completeness and efficiency, with the addition of ACS, in hospital and clinic settings.
Materials and Methods
Study Population
This retrospective study reviewed echocardiograms performed at eight hospitals or combined inpatient/outpatient facilities in California, North Carolina, and Idaho between June 2022 and August 2022. The secondary analysis of the imaging data was deemed to qualify as exempt from institutional review board (IRB) review (Category 2) at Community Regional Medical Center because the research involved the use of educational evaluations that were not influenced by the researcher. The data were abstracted without direct or indirect identifiers. This study was performed to meet required program curriculum standards of the ACS educational program accredited by the Committee on the Accreditation of Allied Health Educational Programs (CAAHEP). The ACS students in this ACS program reviewed 150 echocardiographic cases to determine whether the imaging was compliant with IAC required sonography protocols. Data abstracted included facility of performance, sonographer, completeness, pathology present, and exam timing. These recorded cases were included in that curriculum requirement. In addition, the ACS students are required as part of the Research Methods and Biostatistics course to obtain the Collaborative Institutional Training Initiative (CITI) training certificate and participate in a mock research project. Prior to admission into the ACS educational program, all students had to obtain approval from their respective hospitals to complete the required curriculum. All records were reviewed by the current ACS students with oversight of the ACS program faculty. Sonographers who performed the cases that were reviewed were coded according to their credential achieved (ACS; credentialed [registered diagnostic cardiac sonographer [adult or adult and pediatric] or registered cardiac sonographer] non-ACS; and noncredentialed staff). Of these facilities, four were academic hospitals, two regional hospitals, one pediatric hospital, and one community hospital with shared outpatient clinics. Laboratory accreditation at the time of study completion was recorded; six of eight facilities had obtained IAC accreditation. All the facilities’ imaging protocols followed both American Society of Echocardiography (ASE) Standards and Guidelines 10 and IAC recommended requirements (both adult echocardiography and pediatric echocardiography, respectively) 11 and included all the ASE recommended criteria required for pathology assessment. When assessing compliance for patent ductus arteriosus (PDA), 92% of the patient cases met the complete imaging protocol. There were two pediatric echocardiography laboratories assessed in this study.
Study Procedures
Following ASE recommended Standards and Guidelines, 10 echocardiographic-specific protocols were reviewed to examine four pathologies, including: aortic stenosis (AS), mitral regurgitation for adult transthoracic echocardiogram, as well as pulmonary hypertension, and PDA, for a pediatric transthoracic echocardiogram.
The aortic stenosis evaluation was considered complete if the following measurements were obtained: left ventricular outflow tract (LVOT) diameter, pulsed wave LVOT time velocity integral (TVI), continuous wave (CW) Doppler TVI, and Pulsed Echo Doppler Flowvelocity meter (PEDOF). Apical, right parasternal border (RSB) and suprasternal notch (SSN) images were acquired in patients with moderate to severe aortic valve stenosis estimated by Doppler measurements. The mitral regurgitation evaluation was considered complete in patients with at least moderate mitral regurgitation if the following images/measurements were obtained: color Doppler of the jet in all views; CW Doppler in apical views; and jet height (vena contracta width) in parasternal long axis. The pulmonary hypertension evaluation was considered complete if the following images/measurements were obtained: tricuspid regurgitation color Doppler and CW Doppler images with measured peak velocity and pressure gradient, comparison of pulmonary with systemic pressure (blood pressure was required) notation of mid-systolic notching (CW Doppler) in branch pulmonary arteries, and parasternal short axis to determine septal flattening (systolic, diastolic, or both) images. The PDA evaluation was considered complete if the following images/measurements were obtained: PDA size by two-dimensional images, color flow Doppler and direction of shunt, CW Doppler sampling in the right ventricular outflow tract and high parasternal short axis view, measurements of the left atrium (LA)/aorta ratio, and LA volume (when LA dilatation).
Study Outcomes
The two outcomes were exam completeness and time efficiency. Exam completeness was measured as compliance with IAC echocardiographic protocols on complete transthoracic echocardiographic exams as well as pathology-specific images in patients with aortic stenosis, mitral regurgitation, pulmonary hypertension, and PDA. Efficiency was measured as the time from the start of the transthoracic echocardiographic exam to the completion of the physicians’ final report and analyzed as a categorical variable (0–12, 12–24, and > 24 hours. Compliance with IAC protocols for completion and adherence were dichotomously coded: 1 = Yes, 0 = No.
Statistical Analysis
Categorical variables are reported as counts and percentages. Categorical variables are presented as frequency counts and percentages and compared using chi-squared tests. A comparison of facilities comparing those employing ACS with those not employing ACS was also performed. The effects of whether or not the facility was accredited, whether or not the facility employed ACS staff and if the exam was performed by credentialed staff on IAC compliance was evaluated using logistic regression. All variables were forced in the multivariable model to determine association of exam completeness in 995 cases.
Statistical significance was set a prior a P ≤ .05. All statistical analyses were performed using SPSS version 27.0 (SPSS, Chicago, IL).
Results
Characteristics of Study Participants
Most sonographers were non-ACS credentialed (81.7%, 76/93), followed by ACS-credentialed sonographers (10.7%, 10/93), and noncredentialed sonographers (7.52%, 7/93). Table 1 presents the frequency distribution of the participating sonographers (93) at the eight facilities (labeled A–H) categorized by their credentials/status.
The Credentials/Status of Sonographers Who Participated in the Eight Study Facilities.
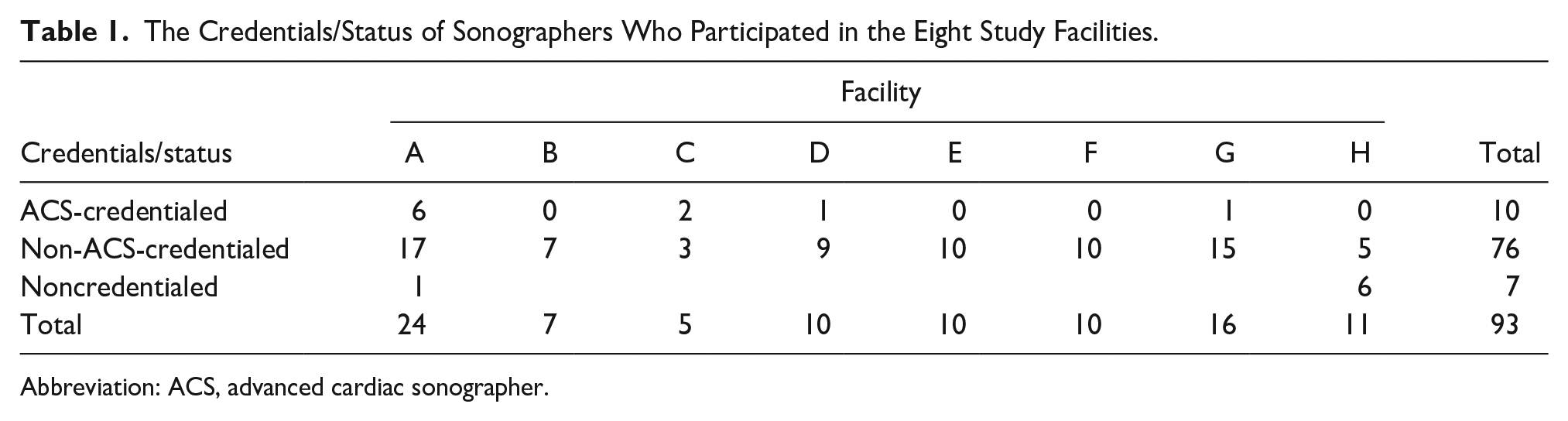
Abbreviation: ACS, advanced cardiac sonographer.
In total, 1147 cases were reviewed at eight hospital and outpatient facilities. Most cases were adult transthoracic (73.9%, 848) and 299 (26.1%) pediatric transthoracic echocardiograms were retrospectively reviewed. The majority of cases were performed by credentialed (non-ACS) sonographers (60.3%, 692), 28.3% (325) were performed by credentialed ACS and 11.3% (130) were performed by noncredentialed staff. None of the noncredentialed staff were new graduates.
A total of 302 cases with pathology were identified among the 1147 echocardiographic examinations. The most frequent examination (31.8%, 96) was aortic stenosis, followed in order of frequency by mitral regurgitation (28.5%, 86), PDA (23.5%, 71), and pulmonary hypertension (16.2%, 49).
Outcome: Exam Completeness
Overall, 806 (70.3%) studies were compliant with IAC protocols. In studies without pathology, compliance was highest with ACS (191/227, 84.1%) and lower with, credentialed non-ACS (376/541, 69.5%) and noncredentialed (78/108, 72.2%, P < .001). The aortic stenosis, mitral regurgitation, pulmonary hypertension, and PDA pathology examinations were more IAC protocol compliant when performed by ACS than when performed by those without ACS credentials. A higher proportion of the examinations by the ACS for aortic stenosis (16/20, 80.0%) were compliant with the IAC protocols compared with credentialed non-ACS (35/63 [55.6%]) and noncredentialed sonographers (6/13 [46.2%]; see Figure 1). A higher proportion of the examinations by the ACS for mitral regurgitation (14/19, 73.7%) were compliant with the IAC protocols compared with credentialed non-ACS (20/56, 35.7%) and noncredentialed sonographers (2/11, 18.2%). The pediatric echocardiograms were performed in an IAC (Pediatric/Fetal) laboratory and followed IAC-specific pediatric echo protocols. There was (35/38, 92.1%) IAC compliance for PDA by ACS-credentialed sonographers compared with (23/32, 77.9%) compliance by credentialed non-ACS sonographers (see Table 2).
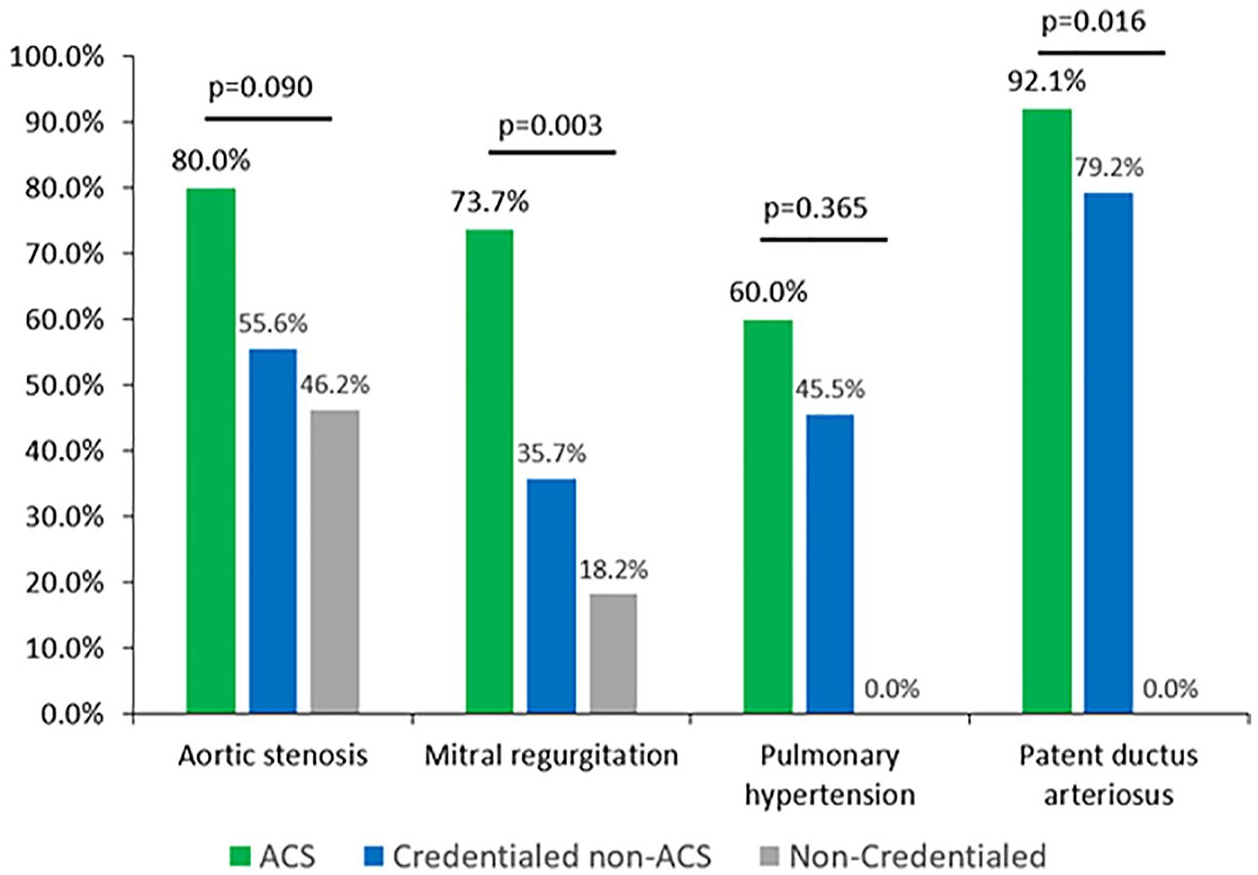
A bar graph that shows the exam compliance, based on Intersocietal Accreditation Commission (IAC) guidelines, for pathology and stratified by the credentialing status of the sonographers. ACS, advanced cardiac sonographer.
The Percentage of Patient Cases With Associated Pathology that Were Accurately Performed by Each Group of Sonographers.
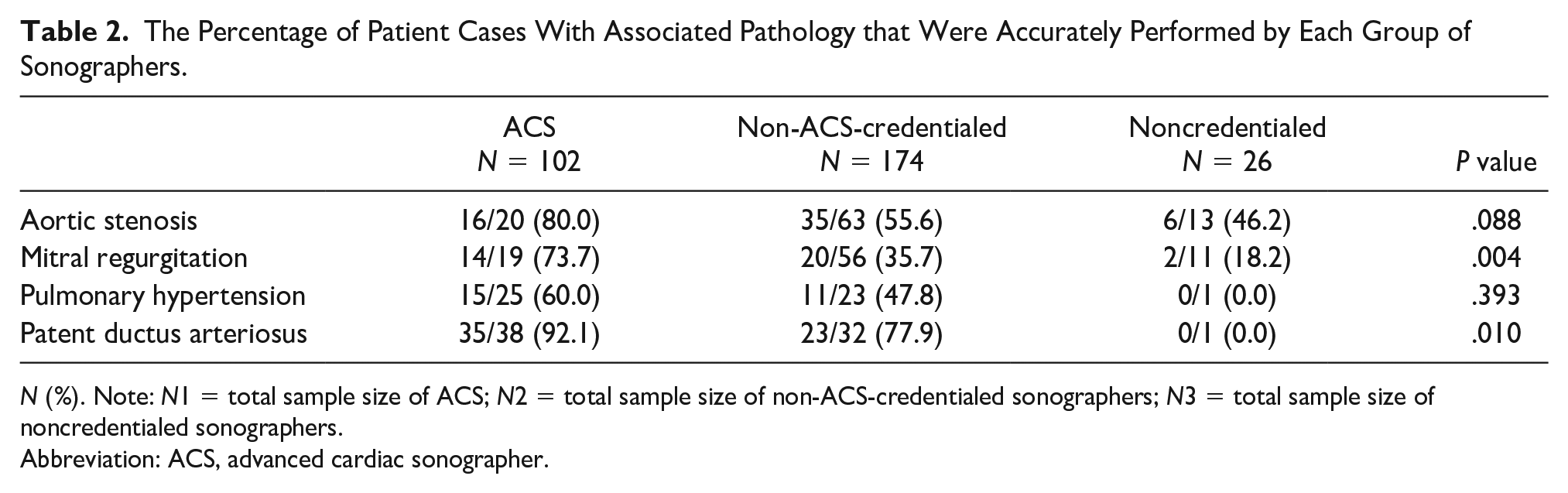
N (%). Note: N1 = total sample size of ACS; N2 = total sample size of non-ACS-credentialed sonographers; N3 = total sample size of noncredentialed sonographers.
Abbreviation: ACS, advanced cardiac sonographer.
When comparing facilities who employed ACS versus those who do not, facilities with ACS more frequently performed a complete protocol (80.0% vs 38.1%, P = .001). Although there was higher compliance in mitral regurgitation (62.1% vs 42.1%) and pulmonary hypertension (61.8% vs 41.7%), the values were not statistically significant (P > .05). Significant predictors of IAC compliance were being performed in an accredited facility (HR = 13.16; CI = 8.59–20.17, P < .001), being performed in a facility that employs ACS (HR = 2.70; CI = 1.79–4.08, P < .001), and being performed by credentialed staff (HR = 2.69; CI = 1.68–4.31, P < .001) (see Table 3).
The Multivariable Predictors of Laboratory Compliance With Intersocietal Accreditation Commission (IAC) Guidelines for Echocardiograms.
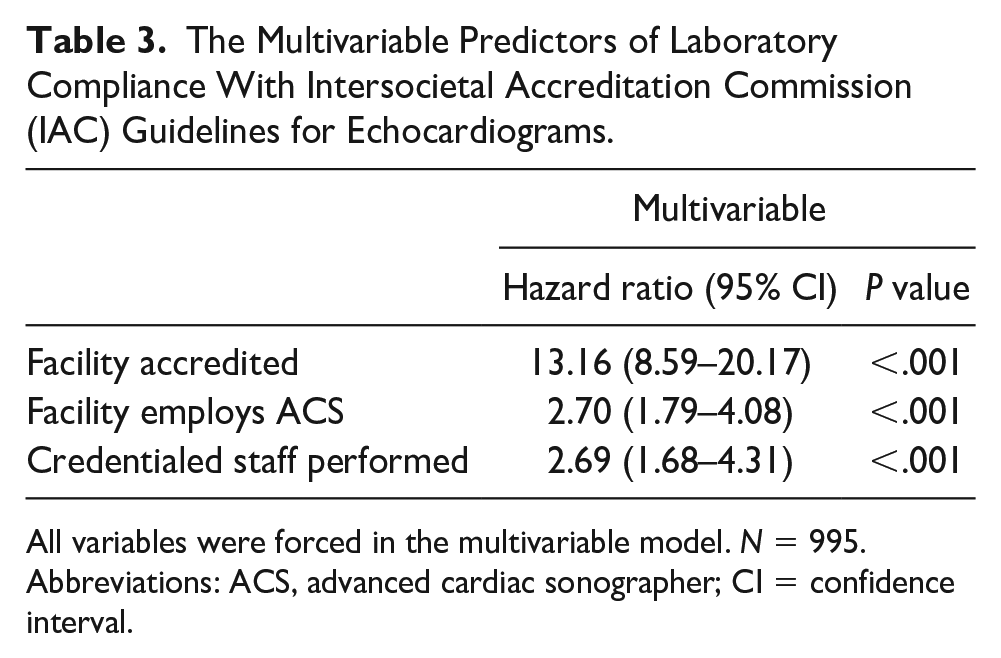
All variables were forced in the multivariable model. N = 995.
Abbreviations: ACS, advanced cardiac sonographer; CI = confidence interval.
Interobserver bias was evaluated by the random selection n = 150 cases of the total n = 1147 cases (13.1%) for double review by a separate reviewer to show percentage of variability. This was completed by Zoom with ACS students and ACS instructor providing oversight. Of the 150 cases, the discrepancy of results was 3/150, resulting in a 98% concordance between reviewers.
Outcome: Time Efficiency
The proportion of ACS who took ≤ 12 hours (74.8%, 240/321) from the start of the transthoracic echocardiographic exam to the time of final physician report was similar in proportion to credentialed non-ACS (75.1%, 520/692) (see Table 4). Noncredentialed staff had the lowest percentage of studies performed within 12 hours (59.2%, 77/130, P < .001) (see Figure 2).
The Comparison of Patient Examination Time Efficiency Compared by Groups of Sonographers.
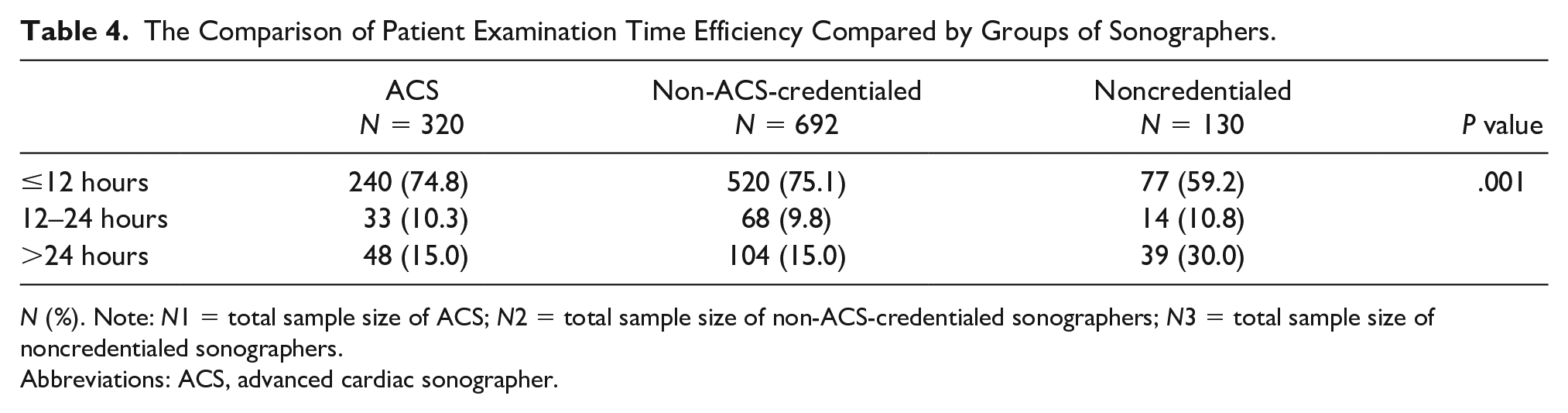
N (%). Note: N1 = total sample size of ACS; N2 = total sample size of non-ACS-credentialed sonographers; N3 = total sample size of noncredentialed sonographers.
Abbreviations: ACS, advanced cardiac sonographer.
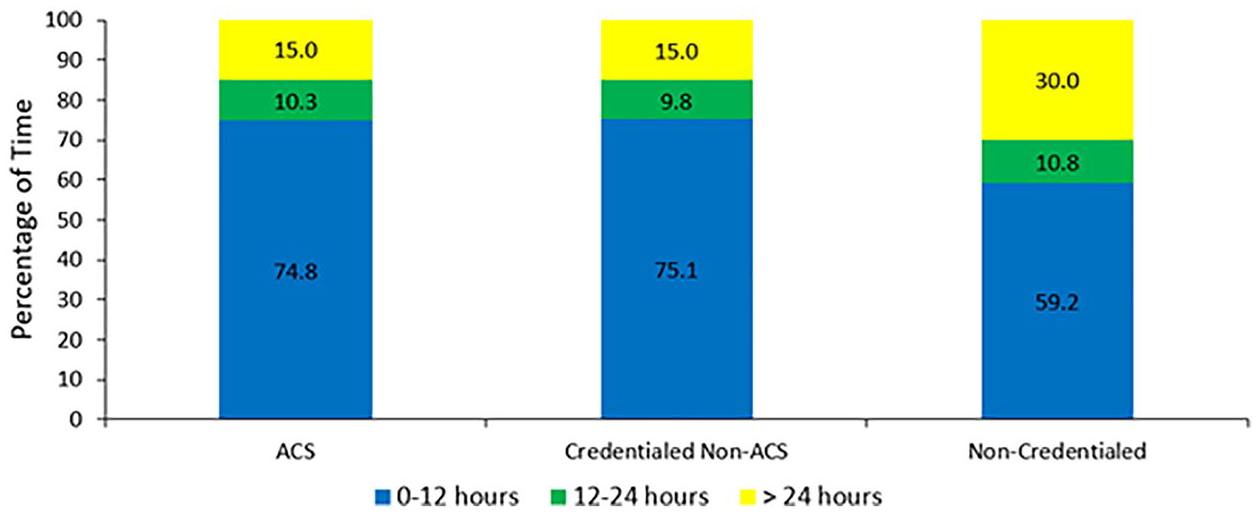
A bar graph that demonstrates the efficiency of the patient examinations that were completed by the credentialed status of the sonographers. ACS, advanced cardiac sonographer.
Discussion
The primary study finding demonstrated that examinations performed with ACS are more often complete in important pathology. This impact in exams performed for ACS is also seen in facilities that employ ACS. The second finding was that examination efficiency improved among credentialed sonographers. Many workplaces that utilize an ACS often provide mentorship, education, and collegial feedback.
This is the first study to examine quantitative parameters related to time efficiency and IAC protocol compliance, when comparing ACS-credentialed versus non-ACS-credentialed sonographers. The ACS has many benefits to patient care, patient flow, and laboratory management. Having the ACS as a resource for everyday oversight and partnering with performing sonographers ensures the necessary images are obtained to answer the clinical question thereby resulting in fewer repeat tests. 7 The ACS aids in creating preliminary reporting to provide physician workflow that is patient centered and time efficient. Despite recommendations in standardization in performance and reporting of echocardiography studies, variation in acquisition remains due to patient’s characteristics, sonographer’s experience, and training.8,9
Since this is the first study to evaluate the impact of credentialing on echocardiographic studies, future studies may be important to further investigate variables of impact. These additional metrics could include inpatient or outpatient testing, year of sonographer’s experience, patient body habitus, and institutional factors that might impact completeness and efficiency.
Limitations
The study design was preexperimental and has threats to internal and external validity. It also did not control for imaging differences in body habitus, patient position, lung/air artifact, patient condition, and patient movement. In addition, staff shortages and/or heavy patient volume leading to intermittent sonographer fatigue was considered. The impact of these variables on completeness and efficiency would be consistent when sampling from a large patient population. There are many variables that affect the efficiency calculation (sonographer begin the exam to physician completion), which may diminish the impact of the sonographer, therefore underestimating the effect. In addition, institutional processes, such as shift assignments and image download processes may affect efficiency. Future studies may be helpful to assess the sonographer performance time and its impact on overall efficiency.
Conclusion
This is the first study to prospectively evaluate the impact of credentialing on exam completeness and efficiency. These results would suggest that credentialed sonographers complete patient exams more efficiently than noncredentialed sonographers. This study may also indicate that ACSs perform more complete exams when compared with nonadvanced sonographers. These results provide baseline evidence of the important potential of credentialing and advanced credentialing in cardiovascular health care. Institutional and patient variability factors affecting completeness and efficiency may be important to evaluate in future studies.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Teresa Daniele (UCSF-Fresno) who serves as the CRMC-ACS Program Medical Director, for her exceptional oversight of the ACS program. This study would not have been possible without the tireless efforts of the ACS graduates/students from the CRMC Advanced Cardiac Sonography Program who collected the data for this study. These cardiac sonographers included:
ACS Graduates:
Robyn Nachtigall-Hill, ACS, RDCS (AE, PE)
Sarah Griffith-Hesser, ACS, RDCS (AE, PE)
Lorenzo Luna, ACS, RDCS (AE, PE)
Jordan LeMay, ACS, RDCS (AE, PE)
Anne Boschma, ACS, RDCS (AE, PE)
ACS Students:
Tammy Witke, RDCS (AE, PE)
Daniel Shnapek, RDCS (AE)
Jesse Hernandez, RDCS (AE, PE)
Amanda Bustamante, RDCS (AE)
Sheila Harness, RDCS (AE, PE)
Farhana Kinlaw, RDCS (AE, RCCS)
Brandi Mello, RDCS (AE, PE)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The secondary analysis of the imaging data was deemed to qualify as exempt from IRB review (Category 2) at Community Regional Medical Center because the research involved the use of educational evaluations that were not influenced by the researcher.
Informed Consent
The data were abstracted without direct or indirect identifiers.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used for the study.
Trial Registration
Not applicable.