
Abstract
Objective:
The aim was to assess the relationship between the coronary calcium score and the common bile duct (CBD) diameter, to determine whether the increase in CBD diameter in patients without hepatobiliary disease could represent cardiovascular disease, or the extent of atherosclerosis in coronary arteries.
Materials and Methods:
The study cohort consisted of 103 patients referred for computed tomographic angiography (CTA) for coronary artery assessment. None of the patients had a gallbladder, biliary, or pancreatic disease or surgery history. The Agatston score determined the rates of arterial calcification. The diameter of the CBD was measured for a sonogram.
Results:
There was a statistically significant relatively strong correlation between calcium score and CBD diameter (r = 0.44, P = .001), independent of baseline variables, such as demographics and cardiovascular risk profiles. In the multivariable regression model, advanced age (beta = 0.825, P = .005), history of hypertension (beta = 0.591, P = .034), and history of coronary stenting (beta = 1.339, P = .001) were shown to be the main determinants of CBD dilatation.
Conclusion:
A statistically significant correlation existed between the CBD diameter and calcium score, within the coronary arteries and this could represent a shared pathophysiology between CBD dilatation and the severity of coronary atherosclerosis.
Biliary disorders associated with a biliary system obstruction can affect a significant portion of the world’s population. Most biliary diseases result in the dilation of intrahepatic and extrahepatic bile ducts. The diameter of the common bile duct (CBD) is an important factor used to differentiate obstructive (dilated CBD) from non-obstructive causes of jaundice. 1 Sonography is a well-established method for evaluating the extrahepatic biliary system and serves as a major diagnostic tool in suspected bile duct obstruction. To better understand the significance of a dilated CBD, it is essential to establish the normal diameter. 1 However, establishing an accurate reference range for the diameter of the CBD remains a topic of debate. A reference range is needed to determine the significance of spontaneous abnormalities or atypical dilation. CBD diameters exceeding the upper limit of this range can be classified as abnormal.
Traditionally, using sonography, the CBD diameter’s upper limit is determined as 6–7.0 mm, in those individuals without cholecystectomy and 10 mm in post-cholecystectomy patients. 2 However, contrast-enhanced abdominal computed tomography (CT) has yielded a more prominent upper limit for diameter of the CBD. In a sample of 604 asymptomatic subjects, the largest diameter reported ranged from 1.8 to 11.8 mm. 1 The diameter of the CBD can change in response to various factors, including age, cholecystectomy, sphincterotomy, certain drugs, such as methadone, measurement location, respiration, and body mass index (BMI).3–9 Among these factors, age has been a focus of many studies. Although the results of these studies have been controversial, and a strong correlation between age and CBD diameter has not been established, some considerations have been suggested for evaluating the normal CBD width with aging. For example, adding 0.2–1.0 mm to the normal upper limit of the CBD diameter, for each increased decade of age, starting at age 40 or 60. 10 Since the increased diameter of the CBD in the elderly is associated with reduced blood flow to the CBD, it could be inferred that the CBD diameter changes may indicate atherosclerosis in arteries. In this regard, the relationship between the calcium aortic score and CBD diameter was investigated, and a moderate relationship between these two parameters was reported. 10 This study was the first to determine the relationship between CBD diameter and coronary artery calcium score using a 64-slice abdominal CT examination.
If a significant relationship is observed between these two variables, it could be concluded that changes in CBD diameter may not only represent cardiovascular disease but also indicate the extent of atherosclerosis in the coronary arteries. Furthermore, considering the non-invasive nature of sonography, in measuring CBD diameter, this could be used as a primary diagnostic test for estimating the severity of coronary artery atherosclerosis, based on patients’ calcium score without known biliary disease.
Materials and Methods
Study Setting and Participants
The current study was completed with a prospective cohort and conducted at a teaching hospital in Tehran, Iran, between May 2018 and September 2019. The study received approval from the hospital’s local ethics committee (IRB# IR.SBMU.REC.9716). The study’s objectives were explained to the patients, and written informed consent was obtained from all participants. The study recruitment included individuals with coronary artery disease (CAD) and referred for coronary artery computed tomographic angiography (CTA). The exclusion criteria included a history of liver, gallbladder, biliary, or pancreatic disease or surgery, such as patients with cholelithiasis or any gallbladder or pancreatic abnormality. Before the examination, serum bilirubin levels, alkaline phosphatase, and liver transaminases were measured and reported as within normal reference ranges for all patients. Patients taking medications that caused smooth muscle relaxation (e.g., calcium blockers and papaverine hydrochloride) and patients with a BMI of more than 25 kg/m2 were also excluded from the study. In addition, patients with a history of coronary artery stent implantation or coronary artery bypass grafting (CABG) were evaluated separately based on their history of atherosclerosis.
Coronary Artery CTA
CTA was performed with a 64-slice device (Siemens Co., Germany), at least 6 hours after the patient’s last meal, and two board-certified radiologists examined the images obtained in all patients. Each patients’ heart rates were evaluated, and a rate of 65 beats per minute was considered appropriate for starting imaging. If necessary, Metoral tablets were used to lower those patients with an elevated heart rate. The patient’s coronary CTA images were assessed to find any stenosis or plaques (see Figure 1). The rates of calcification of plaques were given a number called an Agatston score. Based on the total calcium score, grading of coronary artery disease was done as below:
No evidence of CAD: 0 calcium score
Minimal: 1–10 calcium score
Mild: 11–100 calcium score
Moderate: 101–400 calcium score
Severe: > 400 calcium score
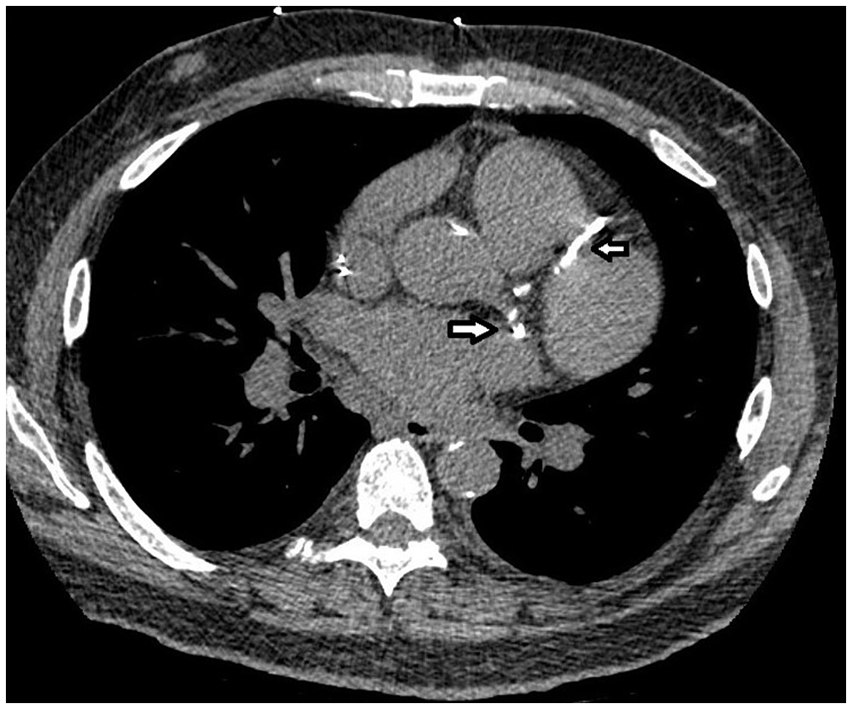
An axial image from the cardiac computed tomogram that shows calcified plaques in the left circumflex and left anterior descending artery (indicated with white arrows).
Sonography of the CBD
Sonography was performed on patients after a fasting period of 6–12 hours by a diagnostic radiologist with 15 years of experience, in conducting sonography. The radiologist was blinded to each patient’s Agatston score. A Samsung WS80A ultrasound equipment system (Samsung Healthcare.com) equipped with a curvilinear transducer (2.5–3.5 MHz) was used for the examination. Patients were examined supine or in the left lateral oblique position and during a deep inspiration, using a right subcostal approach. The CBD was measured below the cystic duct and closely associated with the right hepatic artery. Electronic calipers were used to measure the CBD diameter from the outer to inner edges of the duct (see Figure 2). Three measurements were taken, and the average was considered the CBD’s final diameter. A cut-off value of 7.0 mm was considered for CBD dilatation in this study.
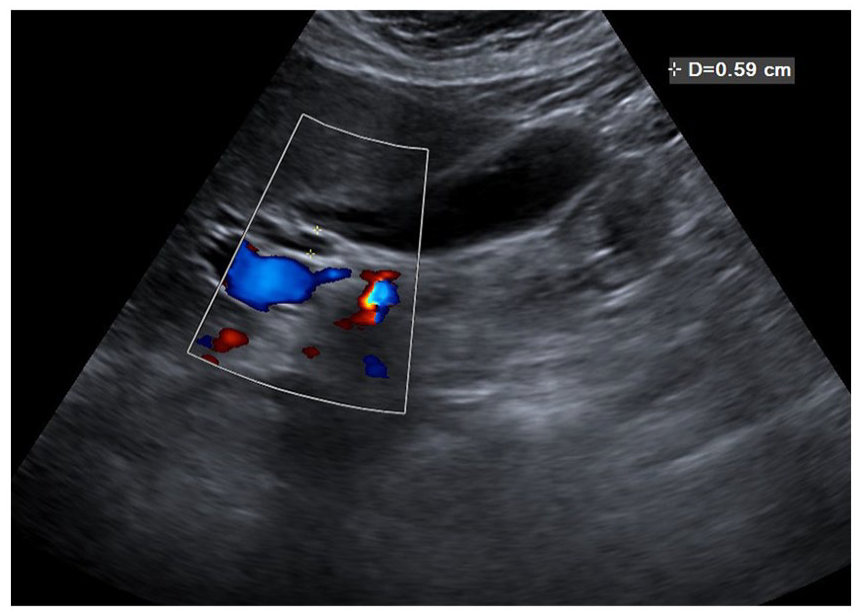
A sonogram of the liver, which demonstrates the method of measuring the diameter of the common bile duct. The electronic calipers are used to measure the diameter of the common bile duct and placed on the outer and inner edges of the duct.
In addition to the CBD sonographic findings and the calcium score of each patient, demographic characteristics and clinical signs of patients were also recorded.
Statistical Analysis
Descriptive data were reported as a mean and ± standard deviation (SD) for continuous variables. Numeric data (percentage) were provided for categorical variables. The Kolmogorov-Smirnov test was used to determine a normal distribution of continuous variables. The means of continuous variables with normal distribution were compared using an independent group t-test. Proportions for categorical variables were compared using the chi-square test. Pearson’s or Spearman’s correlation test, which determines the association between quantitative variables. The multivariable linear regression model was employed to determine the main factors correlating with increased CBD diameter. All statistical analyses were performed using SPSS version 22.0 software (IBM, Armonk, New York), and a P-level of < .05 was determined a priori, as statistically significant.
Results
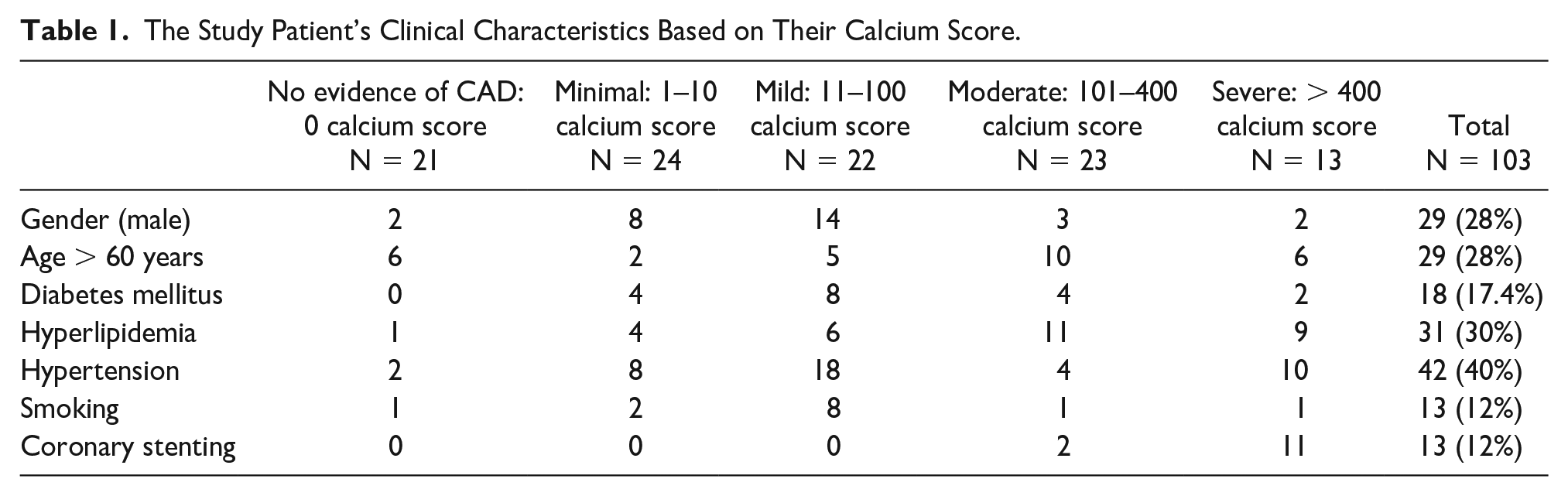
In this study, a total of 103 patients who were referred for CTA and met inclusion criteria were enrolled, however, 21 patients had no evidence of CAD, 24 had minimal CAD, and 22, and 23 had mild and moderate CAD based on their Agatston score, respectively. Thirteen patients had severe CAD (Agatston score > 400). The mean age of participants was 53.79 ± 10.79 years and ranged from 31 to 76 years. In this cohort, 28% were male. Overall, 17.4% had diabetes, 40% were hypertensive, 12% were current smokers, and 30% had hyperlipidemia (see Table 1).
The Study Patient’s Clinical Characteristics Based on Their Calcium Score.
The mean calcium score in men was 49.82 ± 11.74, and in women was 47.32 ± 23.50, with no significant difference (P = .920).
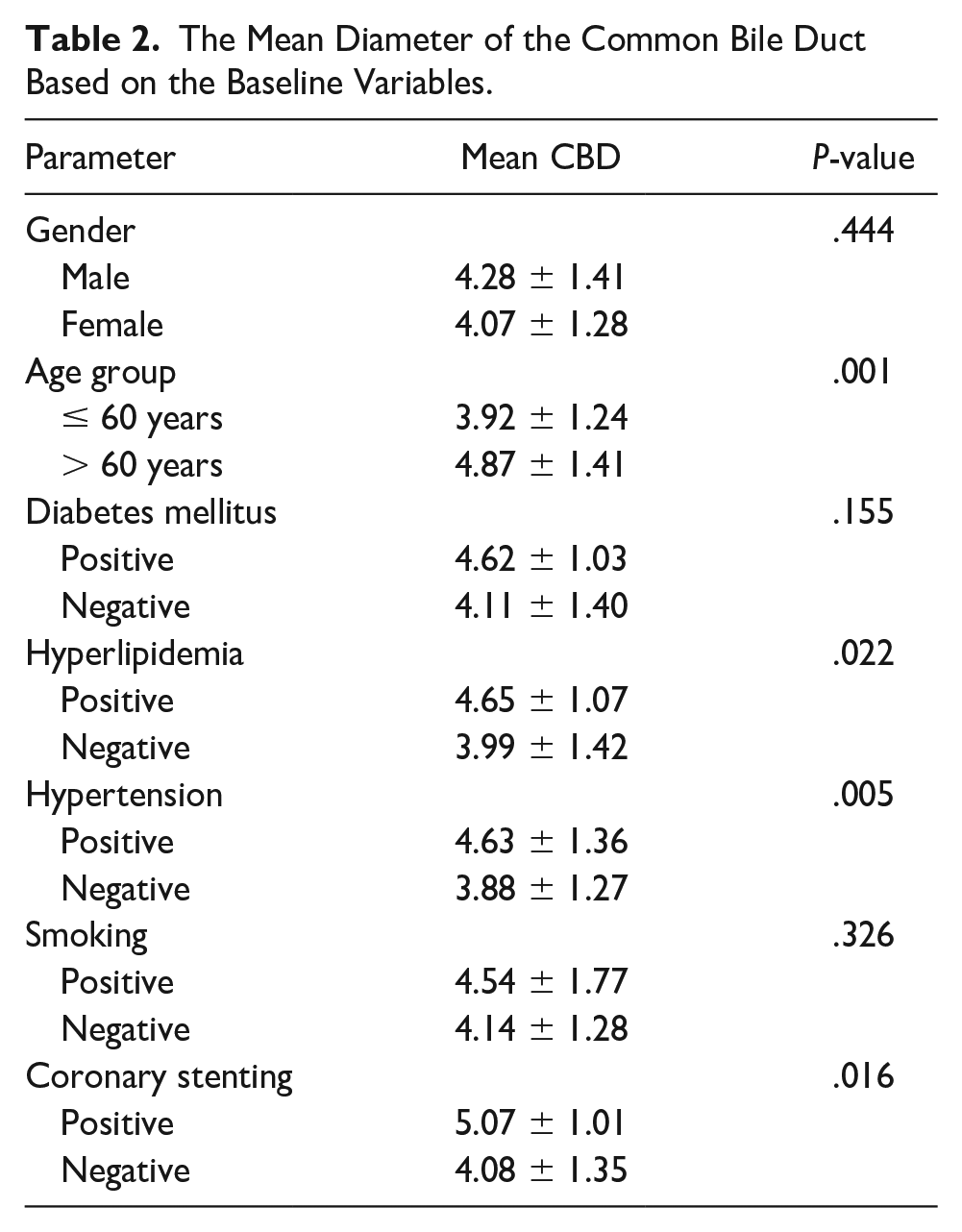
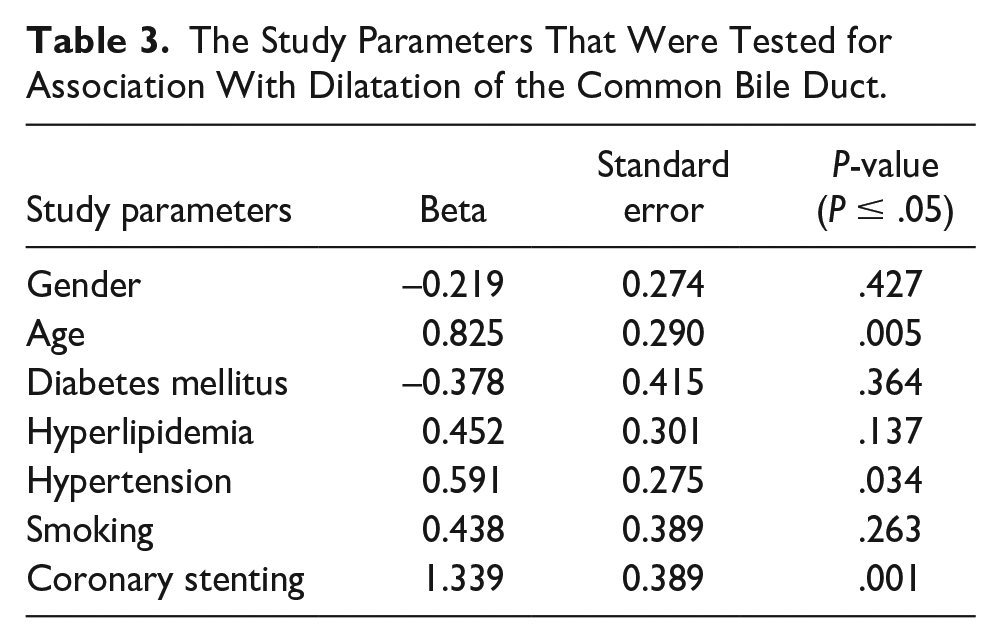
The mean CBD diameter according to the baseline variables is summarized in Table 2. In this regard, the mean CBD diameter was independent of gender, smoking, or history of diabetes. In contrast, a higher mean CBD diameter was found more in older patients than younger patients, as well as those with hyperlipidemia compared with cases without hyperlipidemia. Likewise, a higher mean CBD diameter was found in patients with hypertension compared with patients without, and in patients with a history of coronary stenting than in those without this intervention (see Figures 3–8). In the multivariable regression model, advanced age (beta = 0.825, P = .005), history of hypertension (beta = 0.591, P = .034), and history of coronary stenting (beta = 1.339, P = .001) were shown to be the main determinants of CBD dilatation (see Table 3). A statistically significant relatively strong positive correlation was observed between calcium score and CBD diameter (r = 0.444, P = .001). In addition, a similar association was found between age and the Agatston score (r = 0.543, P = .014) (see Table 4).
The Mean Diameter of the Common Bile Duct Based on the Baseline Variables.
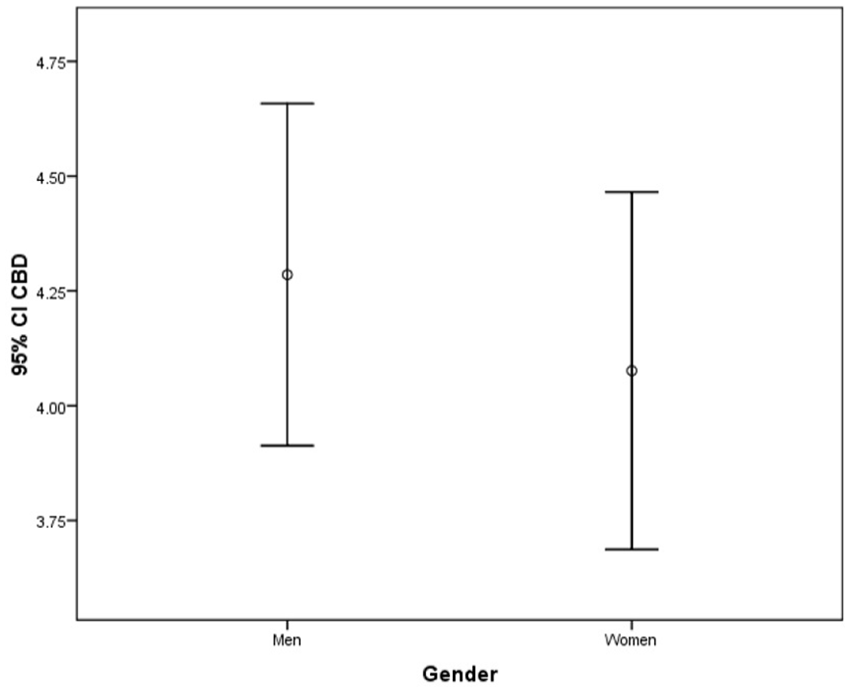
A box plot that compares the mean diameter of common bile duct in men and women.
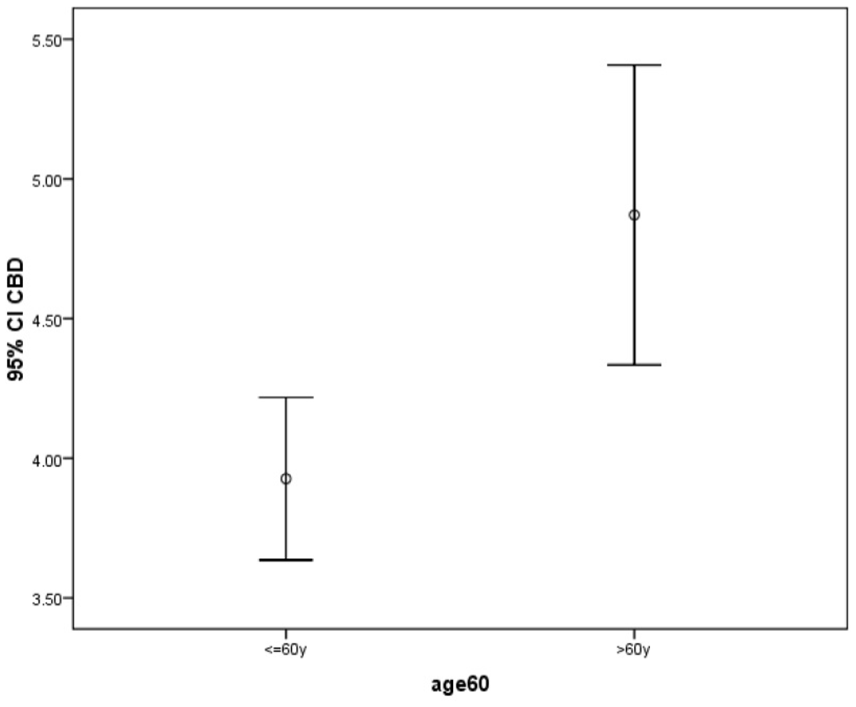
A box plot that compares the mean diameter of the common bile duct in patients younger than 60 and those older than 60.
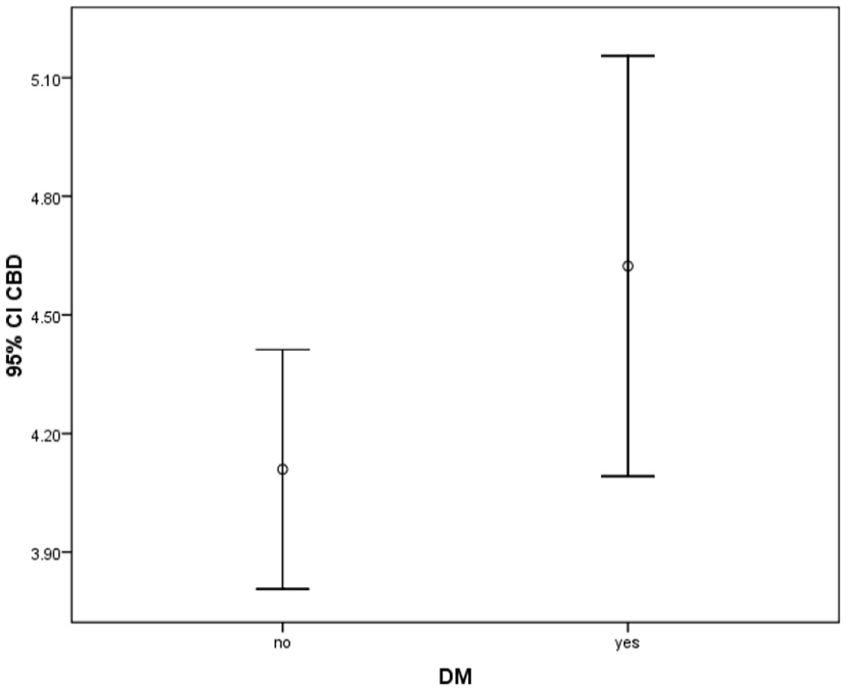
A box plot that compares the mean diameter of the common bile duct in diabetic and non-diabetic patients.
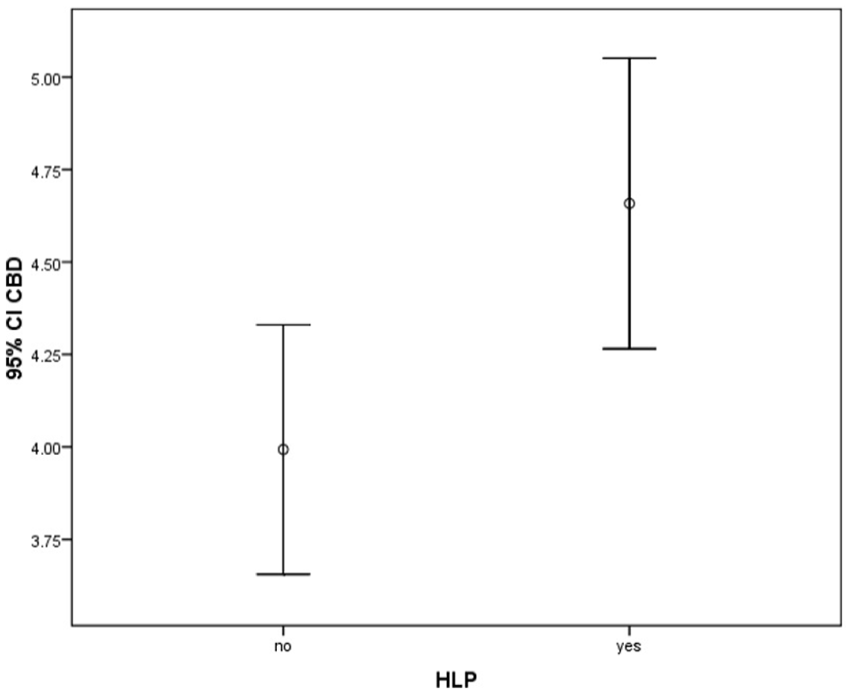
A box plot that compares the mean diameter of the common bile duct in patients with and without hyperlipidemia.
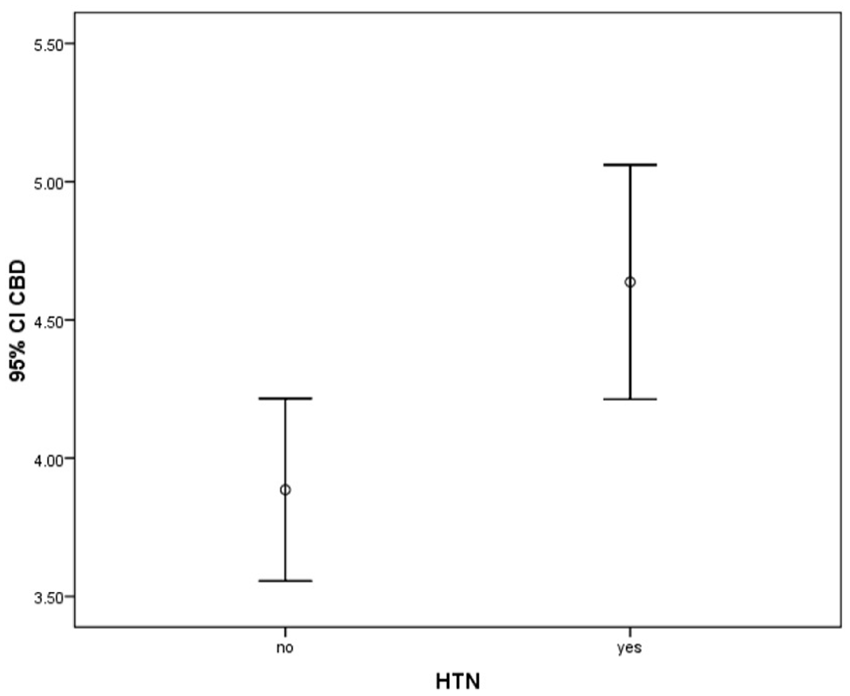
A box plot that compares the mean diameter of the common bile duct in patients with and without hypertension.
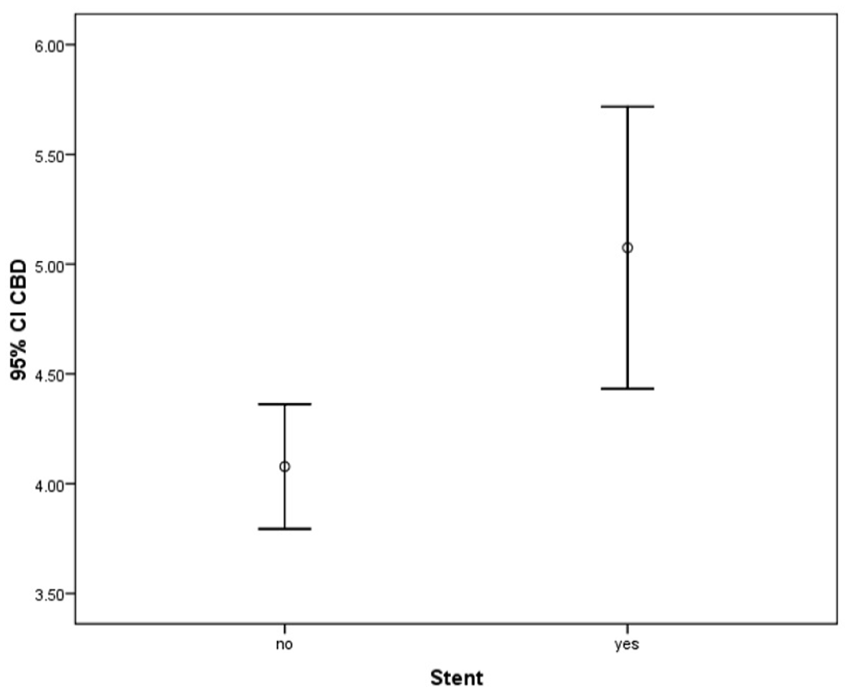
A box plot that compares the mean diameter of the common bile duct in patients with and without coronary stenting.
The Study Parameters That Were Tested for Association With Dilatation of the Common Bile Duct.
The Strength of Association Between Age, Common Bile Duct (CBD) Diameter, and Agatston Score, for This Study Cohort.
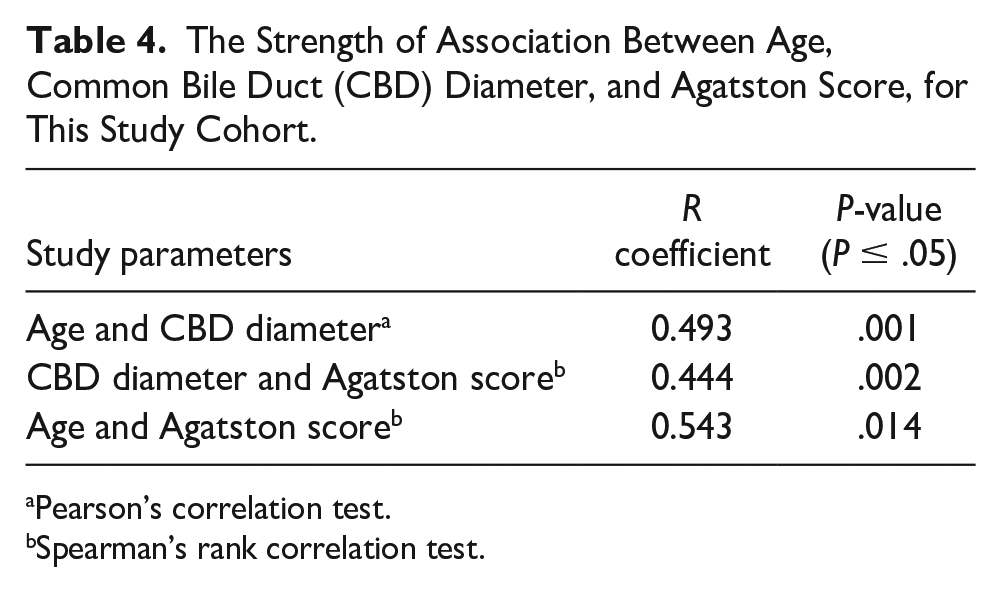
Pearson’s correlation test.
Spearman’s rank correlation test.
Discussion
The role of CT and sonography in assessing various diseases is well known.11 –19 This cohort study investigated the potential association between coronary artery atherosclerosis, based on CT, and the diameter of the CBD, which was measured during sonography. Therefore, the Agatston calcium score method was utilized to assess the level of coronary artery atherosclerosis. The findings obtained in this study revealed a positive correlation between CBD diameter and coronary Agatston calcium score.
As discussed earlier, several factors can influence CBD diameter, and radiologists need to consider these factors when determining whether an observed increase in diameter is pathological. This cohort of patients demonstrated that in addition to factors, such as old age, history of cholecystectomy, drug use, and high BMI, atherosclerosis was also a variable that affected the size of their CBD. Previous research has shown that connective tissue fibers replace normal smooth myocytes as individuals’ age, and tissue metabolism undergoes changes, likely associated with decreased blood supply. 20 These findings and evidence of hypoxia and smooth muscle relaxation 21 suggest the need for further studies to determine the extent to which chronic hypoxia can impact the diameter of the CBD.
Several recent studies have highlighted the susceptibility of pathological changes in biliary dilatation following atherosclerotic changes in the bile ducts, particularly the CBD. Moharramzad et al, found a close correlation between the atherosclerotic score, based on the Agatston score, and the diameter of the CBD. 9 This may suggest that the occurrence of atherosclerosis, especially with age, leads to changes in the vascular supply to the biliary system, particularly the bile ducts. This diminished vascular supply may cause significant changes in the muscles of these ducts and ultimately result in changes to CBD diameter. However, histological evaluations and pathological studies are required to prove such hypotheses, and further research in this area is recommended. Moreover, studies have suggested an association between acute cholecystitis and choledocholithiasis with ischemic heart disease. Salameh et al reported that one-fifth of patients with angina pectoris that needed coronary angioplasty and stenting also required CBD exploration. 21 That study would support the findings of the current study regarding the association between a history of coronary stenting and CBD diameter. In addition, Zheng et al found that patients with a history of gallbladder disease had a 1.15-fold increased risk of coronary heart disease compared with individuals without gallbladder disease. 22 They observed increased intima-media thickness, plaque formation, and calcification in the aorta and iliac arteries, suggesting a link between biliary disease and atherosclerosis. 23 The current study has revealed significant findings regarding the association between CBD diameter and cardiovascular risk factors, such as old age, hypertension, and previous history of coronary intervention. The observed relationship between increased CBD diameter and aging is consistent with findings from other published studies,4,24,25 indicating that aging may lead to decreased flexibility and inflammation in the bile ducts. Similarly, the association between hypertension and CBD diameter may be related to biliary dysfunction and underlying hypertension, although further evaluation is needed to understand the pathophysiology of this relationship.
Limitations
These results are limited by the non-randomized research design with threats to internal and external validity. In addition, the study was conducted at a single center with a convenient sample of patients. The limited the sample size and inability to utilize the full capacity of all university hospitals, in the area, is an additional limitation. In addition, extensive exclusion criteria were implemented to control various factors affecting atherosclerosis and CBD diameter, which further reduced the sample size. Including patients with clinical atherosclerosis, such as those with myocardial infarction, stroke, or peripheral arterial disease, could have increased the number of study patients. However, ethical considerations and radiation risks associated with abdominal CT for these patients prevented their inclusion in the study. It is recommended that future studies focus on investigating the association between CBD diameter and the use of the atherosclerotic cardiovascular disease (ASCVD) score to further enhance our understanding of this possible association.
Conclusion
The findings of this study revealed a statistically significant relatively strong correlation between CBD diameter and the calcium score, within coronary arteries, which may suggest a potentially shared pathophysiology between CBD dilatation and the severity of coronary atherosclerosis. It is important to note that this study had inherent limitations, therefore, the results must be interpreted with caution, regarding the broader population. Further studies with larger and more diverse cohorts are needed to confirm these findings and establish a specific diagnostic cut-off point for CBD diameter. Such a diagnostic cut-off point would be valuable in clinical practice, as measurements exceeding this threshold in patients without the known biliary disease could indicate higher calcium scores in the coronary arteries. This could potentially warrant further evaluation of these at risk patients using more invasive imaging techniques, such as coronary CTA or routine diagnostic angiography.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study received approval from the hospital’s local ethics committee (IRB# IR.SBMU.REC.9716).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used for the purpose of this study.
Trial Registration
Not applicable.