
Abstract
Fahr’s disease is a rare neurological disease that typically presents with neurological manifestations such as movement disorders. In a first recorded patient with Fahr’s disease in Bhutan, psychiatric diagnosis of bipolar affective disorder with current episode of severe depression was made, which is also a known manifestation of Fahr’s disease. Diagnosing a first case of Fahr’s disease is important for Bhutan because, though, it is a rare disease and it emphasizes the importance of recognizing other rare causes of psychiatric illness to tailor the treatment to the individual.
Introduction
Fahr’s disease (FD) is a rare neurological disease that was first described by a German Neurologist Karl Theodore Fahr in 1930. 1 The disease is characterized by bilateral calcification of the basal ganglia, thalamus, dentate nucleus, cerebral cortex, cerebellum, subcortical white matter, and hippocampus. 1 It occurs as an autosomal dominant disease or sporadically, with prevalence being less than 1 in 1,000,000. 1 Genetic causes have been known to occur in about 49% of the cases. 2
A variant of Fahr’s phenomenon, Fahr’s syndrome (FS), differs from FD. FS always occurs secondary to underlying cause of excessive calcium deposits, and the most common cause is hypoparathyroidism. The cause of FD is idiopathic. In addition, FS occurs earlier (30–40 years of age) compared to FD, which occurs a little later (40–60 years of age). Apart from these differences, they resemble in their clinical manifestations of symptoms and signs. 3
Among various presentations of FD, movement disorders such as spasticity, gait disorder, speech disorders, chorea, tremor, dystonia, and Parkinsonism are the commonest manifestations.4,5 Psychiatric manifestations occur in about 40% of patients. Ranging from mild depression and anxiety to more severe forms like mood disorders and psychosis, cognitive dysfunction is a common occurrence of FD. 6 Behavioral problems like apathy, disinhibition, aggressiveness, and impulse control disorders are also manifestations of FD. Other known manifestations of FD include migraine with aura, vertigo, and epilepsy. 3 It has been reported that the most common psychiatric condition associated with FD is mood disorders in which depression is described to be occurring commonly than mania. 7 It has been reported that unipolar mania or bipolar disorder occurs in about 31% of patients with psychiatric manifestations of FD. 8 In 2013, Saleem et al 1 described the following diagnostic criteria for FD:
Bilateral calcifications of basal ganglia on neuroimaging (other brain regions may also be calcified).
Progressive neurologic dysfunction: generally a movement disorder and/or neuropsychiatric manifestations. Age of onset is typically fourth or fifth decade (may present in childhood).
Absence of biochemical, metabolic, mitochondrial, or other systemic abnormalities.
Absence of infectious, toxic, or traumatic cause.
Family history consistent with autosomal dominant inheritance pattern.
Excluding primary causes of excessive calcium deposits such as hyperparathyroidism and phenylketonuria, among others, is an important step in diagnosing FD. 5 The most sensitive diagnostic test for FD along with the history and investigations is brain computed tomography (CT) 4 which is helpful in localizing and assessing the extent of calcium deposits.
Case presentation
A 32-year-old male was admitted to the Psychiatry ward, Jigme Dorji Wangchuck National Referral Hospital with symptoms of severe depression. The history was obtained from the individual, his friends of the monastic school, and his family members who seemed reliable. His past psychiatry history revealed he had two episodes during which he exhibited elevated and irritable mood, disinhibition, increased talkativeness, becoming violent at home, and with increased energy and reduced need for sleep, suggestive of mania but was never evaluated by a psychiatrist. These episodes resolved spontaneously after about a month. He had normal inter-episodic functioning. There was no significant history of drug or alcohol use. He has a younger brother who has a psychiatric disorder suggestive of schizophrenia.
The mental state examination revealed prominent self-neglect, no eye contact, poverty of speech, tearfulness, and significant psychomotor retardation. His speech needed repeated prompting with low tone and volume, and the contents were reduced. His mood was low and the affect was depressed. There were no delusions or any perceptual disturbances. His cognitive function was intact and insight was partially intact. He reported passive suicidal ideations, but there were no past attempts. His physical examination, especially neurological examination, was unremarkable. A diagnosis of bipolar affective disorder and current episode of severe depression was made using the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5).
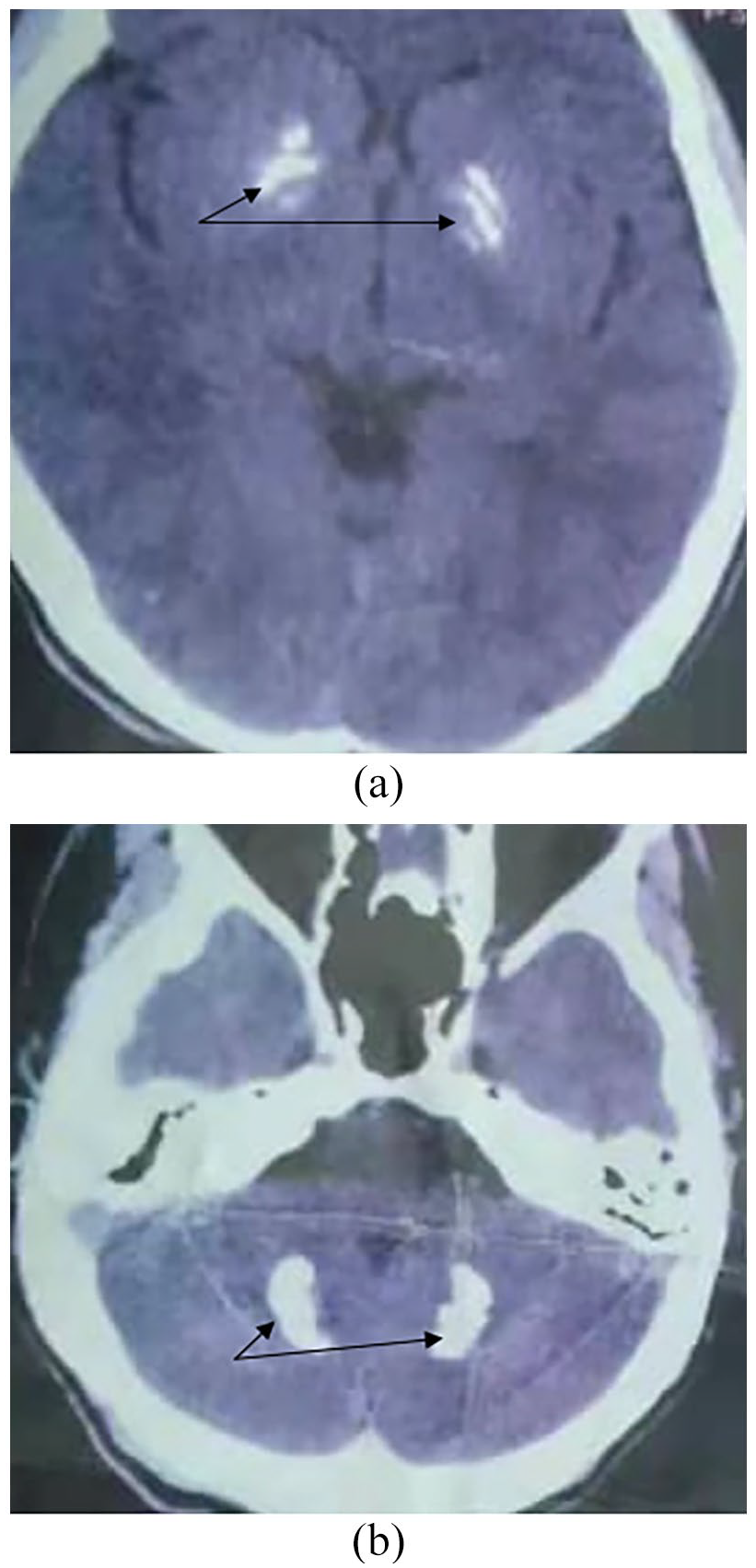
A CT scan of the brain of the index person revealed bilateral calcifications of the basal ganglia, thalamus, and cerebellum as indicated by arrows in Figure 1(a) and (b) respectively.

(a) Bilateral basal ganglia calcification of the index person. (b) Bilateral cerebellar calcification of the index person.
His blood calcium was normal. Despite the minimal decrease in vitamin D-25-hydroxyl level, the parathyroid hormone level was normal. Therefore, hypoparathyroidism was excluded. Other laboratory investigations such as thyroid, liver, and renal tests were normal. Infectious causes such as tuberculosis and human immunodeficiency virus infection were also excluded. Therefore, the primary cause of basal ganglia calcification could not be established. His blood workups are depicted in Table 1.
Blood investigation results of the index person.

H: high; L: low; MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; RDW-SD: standard deviation of red blood cell distribution width; RDW-CV: coefficient of variation of red cell volume distribution width; MPV: mean platelet volume; SGOT: serum glutamic-oxaloacetic transaminase; AST: aspartate transaminase; ALT: alanine transaminase; TPHA/RPR: Treponema pallidum hemagglutination test/Rapid plasma reagian.
We traced the reports of his younger brother and found that he also had bilateral symmetrical calcifications of globus pallidus, bilateral dentate nuclei, and cerebellar folia with no known cause, and that he was being managed as schizophrenia. He has been on maintenance antipsychotics with risperidone 2 mg in the night and olanzapine 5 mg in the night. He lives with his parents and engages in household works under his parent’s supervision.
Figure 2(a) and (b) shows the bilateral symmetrical calcifications of basal ganglia and cerebellum folia, respectively, of the index person’s younger brother.
(a) Bilateral basal ganglia calcification of the index’s brother. (b) Bilateral calcification of cerebellar folia.
A diagnosis of Bipolar Affective Disorder Type I with current episode of severe depression secondary to FD was made. He improved with mood stabilizers (sodium valproate 200 mg in the morning and 400 mg in the night) and second-generation antipsychotics (risperidone 2 mg three times a day). He is in the monastic school at his village and continuing his monastic schooling and is being followed up at the local hospital of his village.
However, genetic testing of both the index and his brother was not carried out due to unavailability of the facility.
Discussion
There are many causes of basal ganglia calcification. Therefore, it is important to exclude other secondary causes of calcifications before considering FD. But in FD, a rare neurological disease, though, several genetic mutations have been so far found to be associated with it, and the exact etiology remains unclear. 9 Genetic causes have been known to contribute to about 49% of the cases. It has been reported that the disease locus is predominantly distributed on chromosome 14q. 5 The identified causative genes include SLC20A2, PDGFRB5, and PDGFB6; mutations in SLC20A2 are the major cause of FD, however. 2 These mutations disturb the normal homeostasis of phosphate in the brain, causing excessive calcium deposits. 2
Although the age of onset of FD has been described to be 40, many people may not exhibit clinical symptoms. However, by 50 years, penetrance of FD is considered full if abnormal calcium deposit in brain CT scans is used as the major criterion for its diagnosis. 2 Up to one-third of patients may remain asymptomatic even though incidental calcifications may be observed in the brain CT scans. 2
The individual described in our case was diagnosed with Bipolar Affective Disorder Type I with current episode of severe depression secondary to FD. The age of onset is not typical in our case; however, literatures have described occurrence of FD in earlier ages. Due to unavailability of resources, he was not subjected to genetic testing. The psychiatric history of his younger brother in addition to the resembling calcifications observed in the brain CT scans of them may indicate the familial nature of FD. The clinical response to treatment has been known to be variable.2,3 Both the siblings responded to psychotropics and mood stabilizers, although the index individual described in the case responded better to the treatment as he did not require everyday supervision unlike his younger brother.
Other psychiatric presentations such as impulse control disorders, obsessive compulsive disorder, and dementia have also been reported apart from bipolar disorder in FD.5,9
The most commonly affected area is the internal globus pallidus, although other areas such as putamen, caudate, dentate nucleus, thalamus, centrum semiovale, subcortical white matter, cerebellum, and brain stem have been observed to have calcifications in FD.4,7 This diverse involvement of the central nervous system also explains the diverse clinical manifestations associated with FD.
Currently, there is no definitive cure for FD. 7 The treatment involves symptomatic relief. 7 However, in the face of either poor effectiveness or bad tolerance to the currently administered medications such as antiepileptics in patients with FD, 1 further work is needed to understand the etiology and therefore devise effective therapies.
Conclusion
FD ranges with a range of clinical symptom: from psychiatric manifestations such as mood disorders to the most common presentation, movement disorders. FD, although rare, is one of the organic causes of mood disorders. The diagnosis of FD was reached after excluding other secondary causes of basal ganglia calcifications. Although genetic testing was not carried out, a positive family history consistent with autosomal dominant pattern was present.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Institutional Review Board (IRB), Khesar Gyalpo University of Medical Sciences of Bhutan: Ref. No. IRB/Approval/PN/2022/007/564, dated 8 April 2022.
Informed consent
An informed written consent was obtained from the index person, his younger brother, and his father (index person’s Legally Authorized Representative) for their anonymized information to be published in this article.