
Abstract
An 18-year-old female patient presented with a 1-month history of low back pain, which had worsened and was accompanied by radiating pain in the right lower limb for half a month. She was admitted to our hospital with computed tomography and magnetic resonance imaging findings suggesting calcification of the L3/4 disc and a large intraspinal mass at the L2–4 level. The patient’s symptoms did not improve with conservative treatment, and her muscle strength rapidly declined. Therefore, a right-sided L3 laminotomy was performed for decompression. Intraoperatively, a cystic intraspinal mass with calcification was observed, and upon incision, a toothpaste-like substance flowed out. Pathological examination revealed fibrous tissue with glassy deposits and calcifications. Postoperatively, the patient’s symptoms resolved completely, with no recurrence observed at the 2-month follow-up and complete resorption of the calcification at the L3/4 disc. Idiopathic intervertebral disc calcification with massive herniation poses a risk of permanent nerve function loss, and timely decompression is recommended to ensure a good prognosis.
Keywords
Introduction
Idiopathic intervertebral disc calcification (IIVDC) is a benign, self-limiting disease with an extremely low incidence, with only over 400 cases reported worldwide.1–3 Because it predominantly occurs in children, it is also referred to as juvenile IIVDC. It most commonly affects children aged 5 to 12 years and has a male:female ratio of approximately 8:5. 2 IIVDC is most frequently found in the cervical spine, followed by the thoracic and lumbar spine.1,4,5 The main symptoms include neck or back pain and restricted movement. 2 When disc herniation compresses the spinal cord or nerve roots, corresponding neurological dysfunction may occur. 5 The exact pathogenesis of this condition remains unclear, although it may be related to trauma or infection. 6
Different from common degenerative disc calcification in adults, IIVDC primarily affects the nucleus pulposus and rarely involves the annulus, with larger calcifications typically within the disc space. 2 Additionally, the herniation of IIVDC often occurs after calcification. Most cases progress quickly, and the process is reversible.7,8 By contrast, degenerative disc calcification often occurs following disc herniation, primarily involving calcification of the annulus fibrosus. 9 This type of calcification is irreversible, typically occurs within the spinal canal, and progresses slowly. From both pathological and clinical perspectives, degenerative disc calcification and idiopathic disc calcification are considered independent diseases.
There are no established standards for the treatment of IIVDC, and most doctors manage the disease based on their own experience. Previous studies have revealed that conservative treatments, such as nonsteroidal anti-inflammatory drugs and external fixation, generally result in a good prognosis, with only a small proportion of cases showing recurrence or progression, at least in the absence of herniation.6,10 In most cases, surgery is reserved for herniation with progressive neurological symptoms or recurrence.1,11 One study showed that conservative treatment can be effective even for herniation with myopathy, 12 while others recommend timely decompression because of the risk of permanent neurological function loss.5,8 The indications for surgical intervention remain controversial and require further clarification.
Here, we report a case of lumbar IIVDC with massive herniation in an 18-year-old patient who experienced rapid, progressive neurological deterioration. Importantly, we highlight a key characteristic imaging finding termed the “tail sign,” which may help distinguish IIVDC with herniation from other intraspinal calcific diseases, such as meningioma. 13 This case provides valuable reference information for the treatment of IIVDC with herniation for other researchers.
Case report
An 18-year-old female patient presented with a 1-month history of low back pain, which had worsened with radiating pain in the right lower limb for half a month. The patient reported that the pain had begun after lifting heavy objects while bending over. The pain was severe, affected her sleep, and was alleviated by bed rest but worsened with activity. She also experienced limited lumbar motion. Conservative treatment with etoricoxib at 60 mg per day and bed rest for half a month had limited effect. She subsequently visited a local hospital, where a computed tomography (CT) scan revealed calcification at the L3/4 intervertebral disc (Figure 1). Acupuncture and etoricoxib at 120 mg per day were prescribed for 3 days; however, her back pain worsened, and severe radiating pain in the front of the right thigh rendered her unable to walk. She was then admitted to our hospital. Treatment with flurbiprofen at 50 mg every 8 hours, methylprednisolone at 40 mg once daily, and 20% mannitol solution at 100 mL every 12 hours was initiated. However, the symptoms persisted and were accompanied by a rapid decrease in muscle strength.

Preoperative imaging. (a, b) CT scans showing massive calcification at the L3/4 intervertebral disc and (c–f) CT and MRI scans demonstrating massive herniation at L2/3 compressing the dural sac and nerve root. The red and white arrows indicate the “tail sign,” a direct channel between the calcified disc and the mass, resembling an umbilical cord or comet’s tail.
Laboratory findings showed no signs of inflammation. On physical examination, the patient was in a passive supine position with limited lumbar spine motion. Muscle strength in the right hip flexor was 2/5. The right-sided femoral nerve stretch test was positive. Both knee reflexes and Achilles tendon reflexes were absent, and the Babinski sign was negative. Magnetic resonance imaging (MRI) revealed a reduced T2-weighted signal at the L3/4 intervertebral disc with slight posterior herniation and compression of the dura mater. At the L2/3 level, a strip of mixed signal was observed in the epidural space with clear boundaries, corresponding to narrowed foramina and compression of the dura mater (Figure 1). CT showed a right-sided strip of high-density shadow in the spinal canal. Compression was noted on the anterior right edge of the dura mater and the right-sided nerve root at the L2/3 level. A direct calcific channel was identified between the intervertebral disc space and the mass. The density of this structure was intermediate between that of the vertebra and fluid, resembling an umbilical cord or a comet’s tail. We termed this phenomenon the “tail sign” (Figure 1).
Due to L3 nerve root compression, neurological dysfunction progressed rapidly, posing a risk of permanent neurological function loss. A right-sided laminotomy at L3 was performed, including removal of the ligamentum flavum and exposure of the intraspinal mass and dura mater. Significant compression of the right L3 nerve root was observed. During surgery, a cystic mass was identified within the spinal canal (Figure 2). Upon incision, a toothpaste-like substance was released. This material was sent for pathological examination, which revealed fibrous tissue with hyaline degeneration and calcification (Figure 2).
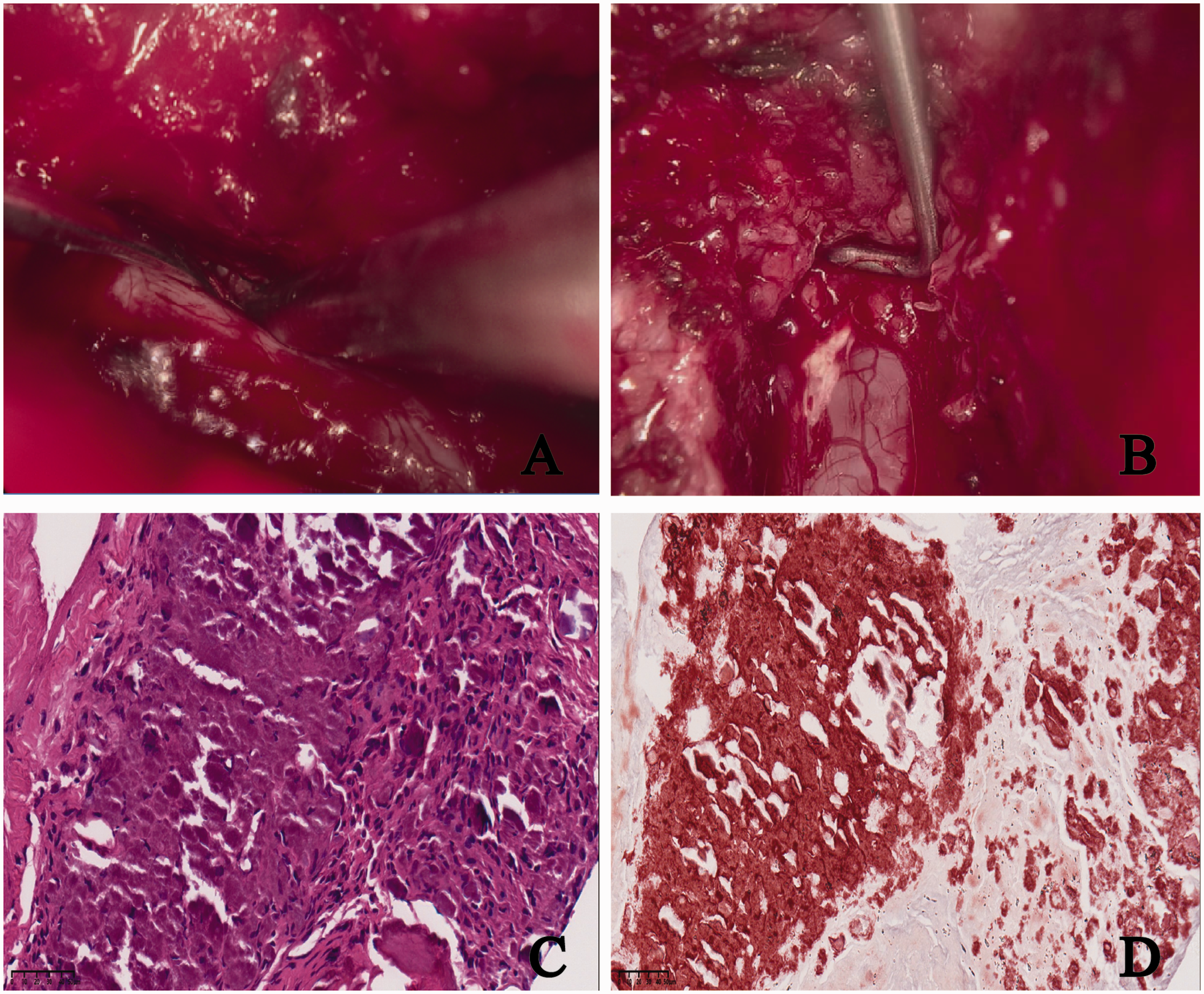
Intraoperative images. (a) A cystic mass is visible within the spinal canal, with the dural hook lifting the cyst wall. (b) A toothpaste-like substance is observed. (c) Hematoxylin–eosin staining and (d) Alizarin red staining showing fibrous tissue with glassy deposits and calcifications.
The patient made an excellent recovery without complications. Follow-up MRI at 2 months postoperatively showed complete absorption of the intraspinal calcification, with a small residual low-signal area at the L3/4 intervertebral space on T2-weighted imaging (Figure 3).

Postoperative MRI. (a, b) T2-weighted imaging showing recovery of the L3/4 disc.
Discussion
Juvenile IIVDC is a rare and distinct disc pathology characterized by calcification within the intervertebral space.1–3 Early-stage CT scans typically reveal dense calcifications in the disc space, most commonly affecting the nucleus pulposus.2,7 It has been suggested that idiopathic disc calcification may originate with calcification of the nucleus pulposus.11,14 When disc calcification herniates, neurological symptoms can occur. CT scans in such cases often show reduced calcification within the disc space and irregular, cloud-like calcifications in the spinal canal. 8 The “tail sign” is frequently observed in patients with herniation.15,16
IIVDC is usually not difficult to diagnose based on the patient’s clinical features and imaging findings. However, in some cases, IIVDC may involve the endplates and vertebral bodies with a mass compressing the spinal cord,7,17 mimicking a tumor; this can easily lead to misdiagnosis. 18 Previous studies have shown that intraspinal tumors, such as meningiomas and chondrosarcomas, can undergo calcification and exhibit imaging features similar to those of disc herniation,13,19 making differential diagnosis challenging. Notably, calcified intraspinal tumors, without disc calcification, do not involve the intervertebral disc. By contrast, IIVDC with herniation often exhibits the “tail sign,”5,10 which may have significant diagnostic value in distinguishing it from calcified intraspinal tumors.
The formation of the “tail sign” remains unclear, and an inflammation-related pathological process may be involved. IIVDC is reported to be discitis in nature, a process involving both the formation and regression of calcification.1,4,11 A previous study summarized current hypotheses to explain the regression of calcification: absorption of the herniation following dehydration, increased intraspinal hydraulic pressure, interaction of inflammatory factors, and re-accommodation of the herniation. 20 Pathological findings in patients with IIVDC typically reveal a mixture of fibrous cartilage, nucleus pulposus, and calcium salts,21–23 suggesting that the calcified disc softens and is gradually absorbed during the process, forming semi-fluid toothpaste-like material, as observed in this case (Figure 2) and other reported cases. 8 We propose that because the herniated material is semi-fluid and contains calcium salts, with a density intermediate between that of the vertebra and fluid, the “tail sign” can be observed on CT scans.
The degree of annulus fibrosis calcification may be related to the risk of massive herniation in IIVDC. The herniation rate of IIVDC is approximately 28%, as summarized by Dushnicky et al. 1 based on cases from 1999 to 2017, but the reason for this high risk remains unclear. Some studies have reported elevated inflammatory markers, such as the white blood cell count, high-sensitivity C-reactive protein, and erythrocyte sedimentation rate, during the course of IIVDC. 1 Additionally, surgical samples have revealed significant neutrophil infiltration, 14 supporting the hypothesis that IIVDC is a self-limiting form of discitis. 11 Annulus fibrosis calcification may indicate that inflammation compromises the integrity of the annulus fibrosis and its adhesion to the endplate cartilage, making it more susceptible to herniation from minor external forces. 10 As the nucleus pulposus and annulus calcifications are absorbed, the disc contents become semi-fluid, and the annulus structure becomes fragile, increasing the likelihood of massive herniation in patients with annulus calcification.12,24 This may explain why massive herniation is commonly seen in IIVDC.5,10
IIVDC is generally treated conservatively. Nonsteroidal anti-inflammatory drugs, muscle relaxants, and physical therapy often yield satisfactory results, with only 2% of cases showing no resolution.1,11 For patients with herniation, Xu et al. 12 recommended a “wait and watch” strategy, at least as an initial management approach, even in the presence of mild myelopathy. However, more than 20 cases have been managed surgically to rescue neurological function.1,4,5,11 Zhu and Chen 8 reported a case of lumbar IIVDC with ossification of the ligamentum flavum treated with posterior decompression and instrumented fusion when the patient showed aggravated neurological dysfunction, resulting in a good prognosis. Conversely, a case of IIVDC with thoracic myopathy managed by urgent decompressive thoracic laminectomy resulted in permanent motor and sensory deficits. 25 In this case, we initially selected a “wait and watch” strategy, but the patient’s neurological dysfunction worsened, necessitating laminotomy for decompression.
The surgical technique chosen for the treatment of IIVDC varies. For cervical IIVDC, anterior fusion is most commonly used, while posterior decompression or instrumented fusion is often applied in the thoracic and lumbar regions.1,4,5 Because IIVDC tends to regress spontaneously, lumbar laminotomy for timely decompression may be a better choice than instrumented fusion in young children. Among the more than 20 reported cases of IIVDC treated surgically, 5 only 1 case resulted in permanent neurological dysfunction, 25 highlighting the effectiveness and necessity of timely decompression. In this case, we performed timely laminotomy to decompress the right L3 nerve root, which resulted in excellent recovery without complications. Because both laminotomy and instrumented fusion have shown good prognoses and no recurrence, 5 we believe that for IIVDC with large herniation, decompression—but not fusion—should be prioritized.
This study has several limitations. The 2-month follow-up period was too short to draw definitive conclusions, despite the fact that more than 20 cases of IIVDC treated with surgery showed no recurrence. 5 Long-term complications, such as recurrence, back pain, and muscle atrophy, remain to be investigated. Additionally, the pathology in this case was not characteristic; no fibrous cartilage or nucleus pulposus was identified, as reported in other cases. 8 This may be due to the absorption of the herniation, suggesting a different pathological presentation during the progression of IIVDC. Furthermore, there have been reports of calcific disc herniation in adults with medical histories similar to that of our patient.12,26 These findings suggest that IIVDC may persist throughout the human lifespan and is not limited to childhood. The pathophysiology of IIVDC warrants further investigation.
Conclusion
In summary, IIVDC with massive herniation carries a risk of permanent nerve function loss, and timely decompression via laminotomy may be an effective approach to ensure a favorable prognosis.
Footnotes
Authors’ contributions
JX Chen treated the patient as a primary care physician and wrote the main manuscript. XQ Fang and WB Xu performed the surgery. S Dai, KM Huang, and YH Chen assisted in the surgery. JX Chen and XQ Fang edited the manuscript. All authors read and approved the final manuscript. The reporting of this study conforms to the CARE guidelines. 27
Availability of data and materials
All data in this article are available.
Consent for publication
The patient provided written informed consent for the publication of their personal and clinical details, including any identifying images, in this study.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The patient provided written informed consent for the treatment and authorized the use of her specimens and imaging data. This study was approved by the Ethics Committee of Sir Run Run Shaw Hospital.
Funding
This work was supported by the National Natural Science Foundation of China Youth Fund (82203446).