
Abstract
Objective:
Work-related discomfort is a pervasive issue among ultrasonography users. The Sonography Work Systems (SWS) framework was constructed as a means of examining relationships within and across components of the sonography work systems, work processes, and work/worker outcomes. A database of ultrasonography users was established as a foundation for a longitudinal survey study to examine worker health and well-being and explore the most salient work systems and process factors associated with work-related discomfort.
Materials and Methods:
An estimated 100 000 unique ultrasonography users were invited to complete the online questionnaire through an e-mail campaign. Snowball sampling occurred through social media posts and encouragement for respondents to share the survey link with colleagues. The questionnaire included items that examined participant demographics, selected constructs from the SWS, and the prevalence of work-related musculoskeletal discomfort, visual discomfort, and headaches. Individual and multi-factorial regression models were conducted to examine SWS factors associated with the likelihood of experiencing the three types of work-related discomfort.
Results:
A total of 3659 valid responses were included in the analysis, with 86% of respondents reporting that they regularly experienced musculoskeletal discomfort that they directly attributed to their work. About half (54.2%) of the respondents have engaged in sonography-related ergonomics training, and respondents indicated using adjustable equipment approximately 74% of the time. Workplace culture was rated as primarily positive, but respondents indicated that employers implement only two of seven commonly recommended ergonomic policies and procedures. Working in an organization with more policies, using adjustable equipment more frequently, taking more work breaks, engaging in a positive work culture, and minimizing interruptions to workflow were key factors associated with reduced likelihood of work-related discomfort.
Conclusion:
This study provides a new framework for examining and addressing factors that contribute to ultrasonography users’ experience of work-related discomfort. Despite increased participation in ergonomics training and the use of adjustable equipment, the prevalence of work-related discomfort remains high among ultrasonography users. The findings highlight the need for attention to be directed at organizational factors and work processes to identify and implement evidence-based solutions to improve the health and well-being of medical ultrasound users.
Keywords
Work-related musculoskeletal disorders (WRMSDs) among sonographers and other users of ultrasonography have become an increasingly prominent research focus, discussion topic, and intervention target over the past three decades.1 –10 The Grand Challenge to stop WRMSDs related to performing medical ultrasonography was launched to address these ongoing concerns. This effort is supported by the WRMSD Grand Challenge Alliance (hereafter referred to as the “Alliance”), which includes the American Institute of Ultrasound in Medicine (AIUM), the American Registry for Diagnostic Medical Sonography (ARDMS) and Inteleos, the American Society of Echocardiography (ASE), the Intersocietal Accreditation Commission (IAC), the Joint Review Committees on Education in Cardiovascular Technology (JRC-CVT) and Diagnostic Medical Sonography (JRC-DMS), the Society for Vascular Ultrasound (SVU), and the Society of Diagnostic Medical Sonography (SDMS). 11 Several initiatives are associated with this Grand Challenge, including a Design Summit, hackathons, and a longitudinal research study of ultrasonography users. The goals of the latter are to document, over time, the health and well-being of ultrasonography users, to explore how their work and environmental conditions affect these outcomes, and to learn what types of interventions are or have the potential to be effective at reducing WRMSD. 12
A full understanding of how to support worker health and well-being requires careful consideration of the complex intersections between various worker, work, and workplace factors. 13 The Systems Engineering Initiative for Patient Safety (SEIPS) framework is a leading sociotechnical systems model that provides a useful foundation for identifying these critical factors. 14 Although the SEIPS framework focuses on health care outcomes for patients, health care professionals, and organizations, it is possible to use this framework to examine worker health and well-being outcomes.12,15 When applied to those who conduct ultrasonography, this framework can be used to examine work system factors that include work organization (e.g., schedules), tools and technologies (e.g., ultrasound equipment systems, transducers, examination tables), tasks (e.g., sonography examinations), people (e.g., users of ultrasonography, patients, supervisors), and internal (e.g., settings, workplace culture) and external environments (e.g., COVID pandemic). Each of these factors contributes to the worker’s physical, cognitive, and social-behavioral work processes that result in worker health and well-being outcomes alongside other organizational and patient outcomes. Both positive and negative worker health outcomes influence the system and re-impact the ultrasonography users, as they continue to engage in work activities over time.
Using this SEIPS model as a foundation, the Sonography Work Systems (SWS) framework was developed (See Figure 1) to depict each of these critical relationships among the work systems, work processes, and ultrasonography users’ health and well-being. Leveraging the support of the multi-disciplinary Alliance, a database of ultrasonography users was established as a means for engaging practitioners across all applications of medical sonography in a longitudinal research project to examine associations of SWS components to worker health and well-being. This article describes the ultrasonography users who joined this database, provides an analysis of the current prevalence of WRMSD within the sonography community, and identifies the most salient work system and process factors related to ultrasonography users who regularly experience work-related musculoskeletal discomfort, visual discomfort, and headaches.
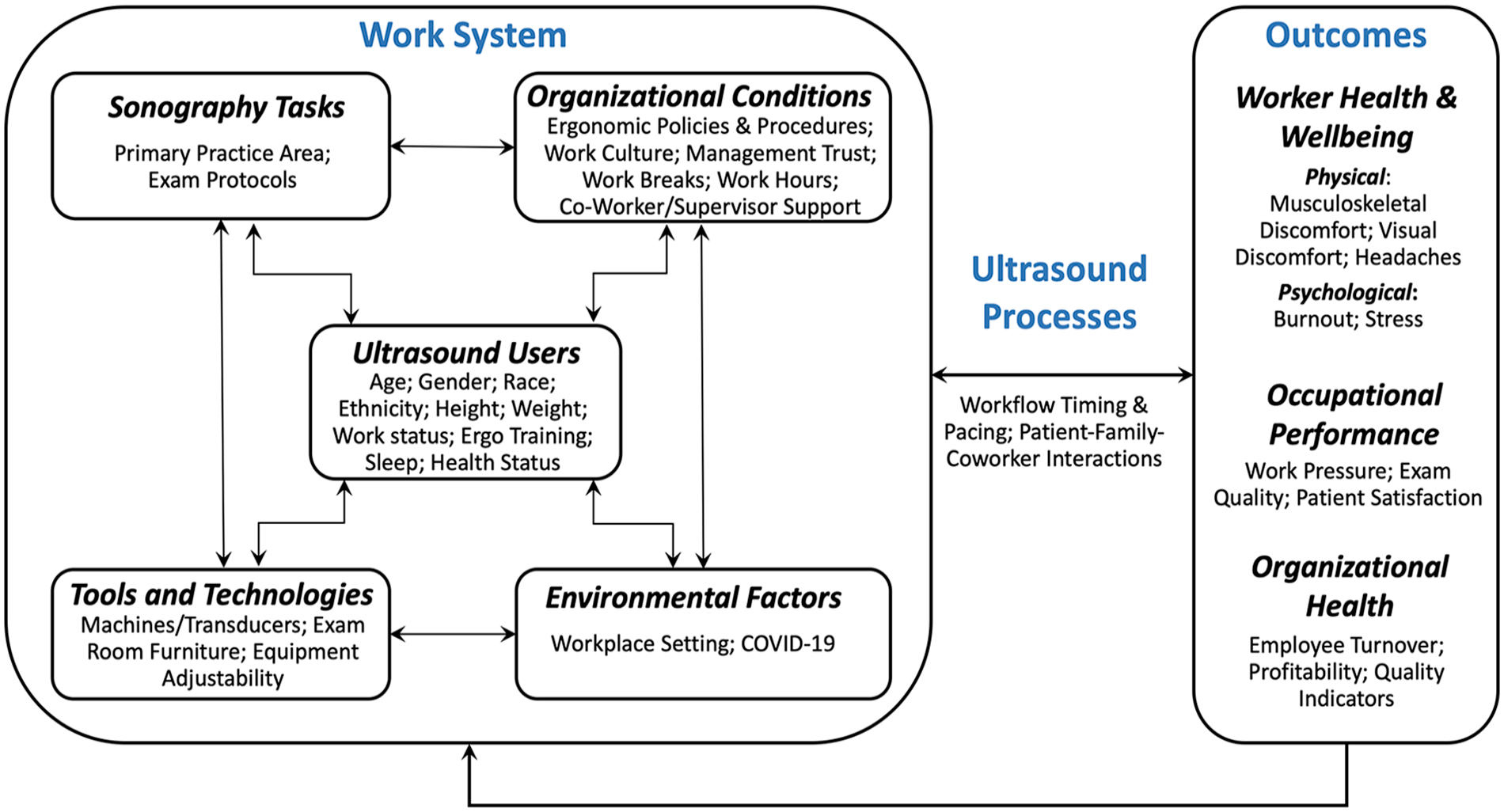
The Sonography Work Systems model demonstrating the relationship among the five work systems constructs, ultrasound processes, and three types of outcomes. Items listed within each component are provided as examples and are not meant to be inclusive of all potential contributing factors, processes, or outcomes.
Materials and Methods
This prospective survey research project was designed to gather longitudinal data from a cross-disciplinary cohort of ultrasonography users. The project was reviewed and approved by the host university’s social and behavioral institutional review board (2021B0113). The approved questionnaire was presented after respondents reviewed an electronic consent form; data were only collected from individuals who agreed to voluntary participation in the survey study.
Respondent Sample
Survey respondents were solicited through a synchronized e-mail campaign sent to members of WRMSD Grand Challenge Alliance organizations who had opted-in to receive e-mail notifications from their organization(s). The e-mail campaign consisted of four messages, beginning with a brief introductory e-mail sent during the first week of June 2021 prior to the launch of data collection. Once the questionnaire was active, an initial invitation to participate (June 8, 2021) and two weekly follow-up reminders (June 16, 2021, and June 22, 2021) were sent. To ensure the privacy of member data, each Alliance organization sent e-mails to its respective member list. The three largest organizations each sent 89 905, 22 693, and 11 544 initial invitations, among which there was potentially a large amount of member overlap. Although distributed by the organizations, the content, signature, and reply contact for each e-mail were associated with the research team. This recruitment strategy conveyed to recipients that the Alliance organization distributing the message fully supported the research effort, but that independent university researchers were conducting the study. In addition to the e-mail campaign, snowball sampling occurred through social media posts by the research team and Alliance member organizations, and encouragement for respondents to share the survey link with colleagues.
Questionnaire Deployment and Design
Data were collected using a questionnaire deployed via Qualtrics that was available from June 8 to 28, 2021. Two screening questions were used to identify qualified respondents who were working in a job that required the use of ultrasonography. Respondents were excluded if they were not working (i.e., looking for work, laid off, on disability), were a student, or were working in a country other than the United States or Canada. In addition, to be included, respondents were required to provide contact information (e.g., e-mail) and a valid job title for purposes of data validation and future follow-up.
Close-ended questions were developed that would allow for a broad description of ultrasonography users’ physical health and the exploration of work system factors and work processes that are critical to worker health outcomes, as conceptualized in the SWS framework. Questions aiming to develop a deeper understanding of the complexities among the individual sub-components of the work system were reserved for future components of the longitudinal study. Details of the broad constructs evaluated by this initial questionnaire are provided in the following sections of this article.
Work systems
Person
Demographic questions included gender, racial and ethnic identities, age, handedness, height, and weight, the latter of which allowed for calculating each respondent’s body mass index (BMI). Work status was captured as full-time, part-time, or per diem (e.g., traveler, contractor, self-employed). Respondents indicated their training by selecting medical or sonography-related credential(s) they held (multi-choice allowed) and by selecting “yes” or “no” to the question: “Have you ever completed any sonography-related ergonomics training?” Respondents who indicated having received ergonomics training selected the provider(s) and method(s) of training received (i.e., self-study, hands-on, online lecture, in-person lecture), the most recent year they participated in ergonomics training, and if the ergonomics training was applicable or helpful in their work.
Environment
Two broad questions were included to describe the respondents’ external and internal working environments. First, respondents provided the zip code where they primarily engaged in sonography work. The zip codes were used to categorize respondents into four regions (i.e., Northeast, Midwest, South, and West) based on the U.S. Census Bureau’s geographic division; 16 the respondents from Canada were not allocated to regional sub-categories due to the limited sample size. Second, the internal environment was operationalized as the general workplace setting in which a respondent conducted sonography, allowing for multi-selection among the following: hospital, outpatient clinic/lab, physician’s office, urgent care, educational setting, or other workplaces.
Tasks
Areas of sonography application were identified by asking respondents to indicate practice specialties in which they apply their sonography skills at work. Respondents chose one or more imaging practice areas from the following: abdomen, breast, cardiac adult, cardiac fetal, cardiac pediatric, musculoskeletal, obstetrics/gynecology (OB-GYN), pediatric, vascular, veterinary, point-of-care (e.g., rehabilitation, emergency medicine, sports medicine), or other practice area.
Tools
In this initial questionnaire, it was important to gain an understanding of the overall adjustability and ergonomic features of the ultrasound equipment system and other furniture or equipment within sonography suites, examination rooms, and other spaces where imaging is conducted. The researchers developed six best-practice statements regarding the use of adjustable equipment (i.e., ultrasound equipment systems, chairs for conducting examinations, chairs for administrative tasks, examination tables or patient beds), access to adequate space in examination rooms, and an overall assessment of ergonomically correct examination performance (Supplemental Appendix A). Respondents used a visual analog scale to indicate the percentage of time (0%–100%) across the last 7 days that each statement was true. The researchers used the mean percentage of time across these six questions to represent a respondent’s overall use of adjustable equipment in the analyses.
Organization
The questionnaire evaluated four broad organizational factors. First, using the same question structure as with adjustable equipment, researchers calculated the mean percentage of time respondents took appropriate breaks from their work tasks. Next, respondents indicated if their employer at the primary place of employment did or did not apply each of seven ergonomic policies and procedures which were informed by recommendations in existing practice standards.17,18 Finally, items were extracted from the National Institute for Occupational Safety and Health’s worker well-being questionnaire (WellBQ) 19 to explore perceptions of workplace culture (five statements) and trust in management (one statement). Respondents rated agreement with each statement using a four-point, Likert-type scale ranging from strongly disagree (i.e., 1) to strongly agree (i.e., 4). The average rating across statements related to culture and the selected rating of trust ranged from 1 to 4 with higher scores representing a more positive workplace culture and more trust in management. The individual questions that determined a respondent’s value for each of these four organizational factors are included in Supplemental Appendix A.
Work processes
This initial questionnaire explored one broad work process construct, interruptions to the timing and pacing of workflow, using four statements of situations that often occur within sonography workplaces. Respondents indicated how frequently (i.e., 0%–100% of the time) they worked outside of their scheduled work shift or adjusted their workflow due to late patients, administrative issues, and examination difficulties (Supplemental Appendix A). The mean of these four questions was used to represent the overall percentage of time a respondent regularly experienced interruptions to their workflow.
Work and worker outcomes
Musculoskeletal discomfort was identified by the Alliance and study team as a critical worker health outcome of focus. For this outcome, experiences of discomfort were examined across nine body regions: shoulder, elbow, wrist/hands, neck, upper back, lower back, hip/thigh, knees, and ankle/feet. In this portion of the questionnaire, participant reports were not restricted solely to work-related etiology. Rather, musculoskeletal discomfort was defined as any ache, pain, stiffness, burning, numbness, tingling, or other self-reported symptoms within a body region within the prior 12 months. A set of follow-up questions were completed for each body region in which a respondent reported experiencing musculoskeletal discomfort. These questions included a rating of the typical intensity of discomfort from 0 to 10 using a visual analog scale, the frequency of symptoms (e.g., daily, a few times a month), and whether the discomfort had occurred within the most recent 7-day period. Respondents also indicated if the discomfort was made worse by activities at work, made worse by activities outside of work, interfered with the performance of daily activities, or led to a permanent or temporary change in jobs/duties. Finally, respondents noted whether they had taken medication, sought health care support (e.g., doctor, therapist, chiropractor), or took sick leave from work due to their discomfort within each body region.
In addition to general musculoskeletal discomfort, respondents’ experiences of work-related physical discomfort were of interest as primary outcomes for the longitudinal study. Three physical health outcomes were examined by respondents indicating whether they do or do not regularly experience musculoskeletal discomfort, visual discomfort, and headaches during or following their work shift that they directly attribute to their work. In addition to physical discomfort, questions were included to explore the respondents’ overall perceptions of work performance. Respondents indicated how often they perceived their work performance to be poor (i.e., 100% indicating poor performance all the time) across three statements, with the final measure of work performance considered as the mean percentage of time across the statements (Supplemental Appendix A).
Data Management and Analysis
Data management was completed to identify and remove ineligible, duplicate, and incomplete responses. To be considered complete, respondents were required to complete questions within each section of the questionnaire, including a final question that asked for permission to include the respondent as a member of a database registry for future follow-up. Researchers examined the data set of complete responses for errors or outliers and calculated means (standard deviations) and frequencies (percentages) for all individual variables across the respondent sample. Then, a descriptive analysis of general musculoskeletal discomfort data was conducted to identify the 12-month and 7-day prevalence, intensity, and relative impact of region-specific musculoskeletal discomfort among respondents. Finally, the prevalence of work-related physical discomfort was identified by counting the number of respondents who indicated experiencing each of the three types of work-related discomfort: musculoskeletal, visual, and headaches. T-tests and chi-square tests were used to compare each of the work system, process, and outcome variables between respondents with and without work-related musculoskeletal discomfort as the primary worker health outcome of interest.
Following these descriptive analyses, a simple logistic regression was used to examine the relationships of each work system and work process factor to experiences of the three types of work-related discomfort. The discrete categorical variables of gender, race, ethnicity, and work status were modeled as binary (i.e., the largest category vs. all other respondents), and the multiple-response categorical variables of environment and tasks were modeled as binary at the level of each response category (i.e., “yes” vs. “no”). For ergonomics training, the primary question explored in the regression analyses was, “Have you ever completed any sonography-related ergonomics training?” All continuous variables were examined for normality prior to inclusion in the regression models. Finally, variables measured as a percentage of the time (i.e., using adjustable equipment, taking breaks, interrupted workflow) were scaled down by a factor of 10 to model changes in every 10% increment of time rather than every 1% increment of time.
The associational analyses were conducted in two stages. First, the individual regression models were created to explore associations of the person, environment, task, tool, organization, and process constructs to each of the three work-related discomfort outcomes. These results were used to build multi-factorial models that combined salient factors related to each discomfort outcome. Age, gender, ethnicity, race, work status, work environment, and task variables were included as key descriptors to be considered within the models. Any other variable that had a P value <.15 within the individual construct models was included in the multi-factorial prediction models for each work-related discomfort outcome. Using a significance level greater than a traditional 0.05 level in the early stages of the modeling process is recommended because beginning with smaller values has been shown to fail to identify variables that are known to be important. 20 The Statistical Analysis Software 9.4 (SAS Institute) was used for all analyses, and a P value of <.05 was set as a threshold for statistical significance in all final models.
Results
Overall Respondent and Work Characteristics
A total of 6172 survey starts were recorded based on respondents who clicked through the informed consent. Respondents who did not provide a valid job title (n = 1142) were not currently working (i.e., retirement, disability, students; n = 328), were employed in countries outside of the United States or Canada (n = 87), or who did not provide identifying contact information (n = 17) were excluded, and 32 duplicate responses were removed. The remaining 4566 responses, a 74.0% valid response rate, were reviewed for inclusion. A total of 3659 responses were deemed complete, a 59.3% completion rate, and were included in the final analysis.
Respondents were predominantly ultrasonography users with a sonography credential who reported working in clinical settings, with a small representation of individuals working in academia or having supervisory roles; approximately 1% of respondents were physicians (n = 41). The four most common practice specialties in which respondents conducted sonography examinations were vascular (n = 2011), abdomen (n = 1747), OB-GYN (n = 1967), and cardiac adult (n = 1253), and the most common credentials among respondents were RDMS (64.2%), RVT (47.5%), and RDCS (33.4%). Most responses were received from the United States (95.5%; n = 3495), and white, non-Hispanic, and female were each chosen as demographic descriptors by at least 85% of the sample. Most of the sample reported working full-time (80.2%; n = 2936). Hospitals and outpatient clinics or labs were the two most common workplace settings, with 58.5% and 46.5% of respondents, respectively, while 21.8% of respondents conducted sonographic examinations within physician’s offices and fewer than 10% worked in urgent care or educational settings.
Slightly more than half (54.2%; n = 1982) of the respondents reported having completed sonography-related ergonomics training. The ergonomics training took place an average of 5.3 years prior to the survey (standard deviation = 5.7 years). Of those who received training, 90.4% reported they were able to apply the ergonomics training to the workplace, and 85.2% indicated that the training was helpful in some way. Of those who engaged in ergonomics training, the majority received training from a medical or sonography association or other continuing medical education providers; training as part of an academic program or by the employer was much less common. Lectures were the most common training type, with 54.1% of respondents who received training attending online lectures and 63.2% having attended an in-person lecture; hands-on training was the least common, reported by approximately one-third of the sample.
Overall, the respondents worked in organizations with a generally positive work culture (2.9 ± 0.8, on a scale from 1 to 4), but respondents had mixed perceptions of trust in management (2.6 ± 1.0, on a scale from 1 to 4). While a plurality of respondents indicated somewhat agreeing that they could trust management (41.3%), only 17.8% of respondents strongly agreed, and 40.9% of respondents either somewhat or strongly disagreed. Responses to the individual questions related to percentages of time using adjustable equipment and taking work breaks had multi-modal distributions, which indicates between-participant variability that requires further exploration. However, when each participant’s responses to questions within a factor were aggregated and averaged, the resulting index scores for each factor were normally distributed. On average, respondents reported using adjustable equipment about three-fourths of the time (73.6% ± 21.1%) and taking regularly recommended work breaks about two-thirds of the time (64.9% ± 27.6%). Regarding work processes and outcomes, the respondents noted experiencing interrupted workflow timing and pacing and negative work pressure and performance slightly less than half of the time (46.9% ± 26.0% and 44.9% ± 26.0%, respectively).
Despite mostly positive overall reports relative to organizational factors across the sample, respondents noted that, on average, their employers had only 2.1 ± 1.9 out of the 7 recommended ergonomics policies or procedures in place. One-third (32.6%; n = 1192) of respondents indicated that they had reported an ergonomics issue or concern to their supervisor or employer. Of those who reported an ergonomics concern, only 27.5% (n = 328) felt that their concern was adequately addressed, and 6.0% (n = 71) of respondents reported experiencing retaliation or threat of retaliation for reporting their ergonomics issue. Finally, 41 (3.4%) of these respondents had requested a NIOSH worksite evaluation, and very few (0.9%; n = 11) contacted OSHA to file a complaint.
Experiences of Musculoskeletal Discomfort
Nearly all respondents (98.2%; n = 3592) reported experiencing musculoskeletal discomfort in at least one body region within the last 12 months, and 92.5% (n = 3386) of the sample indicated experiencing musculoskeletal discomfort in at least one region within the most recent 7-day period. The prevalence of recent (last 7-days) experiences of musculoskeletal discomfort was highest in the shoulder (71.7%), neck (61.1%), and wrist/hand (57.5%); fewer than one-quarter of the participants reported recently experiencing discomfort in any of the lower extremity regions (See Figure 2). Despite the varied prevalence, the average intensity of musculoskeletal discomfort fell within a narrow range of 4.6 to 5.2 (out of 10) across all body regions, and about half of the respondents indicated that their musculoskeletal discomfort interfered with daily activities (i.e., ranging from 44.1% to 61.6% across the body regions).
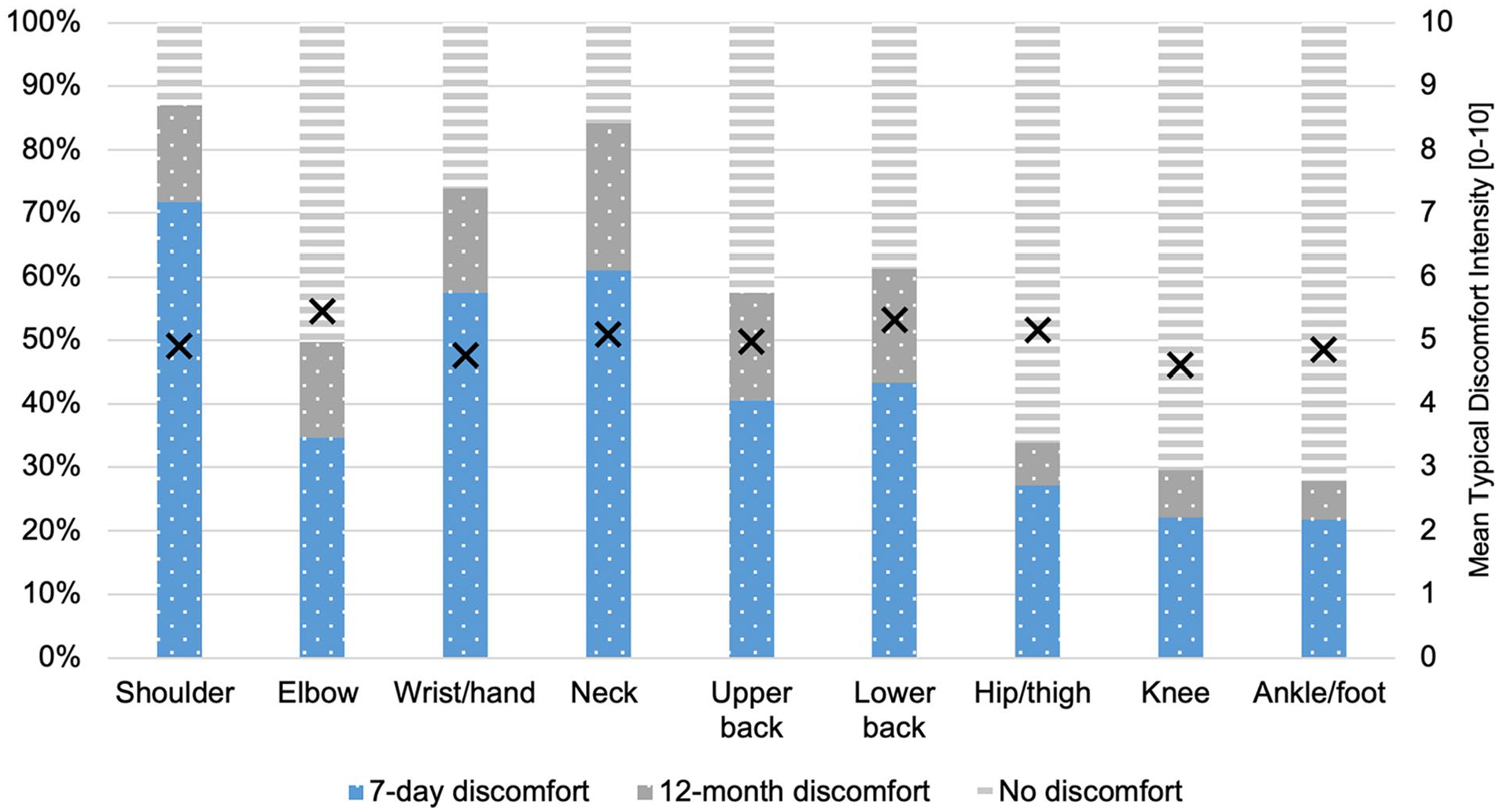
Seven-day and 12-month prevalence of musculoskeletal discomfort among survey respondents (n = 3659) by body region. Markers (X) indicate the mean typical intensity of discomfort (0–10) for each body region among participants who reported experiencing discomfort in that region within the most recent 12-month period.
Response percentages for all additional follow-up questions regarding experiences of musculoskeletal discomfort among those who reported discomfort within the last 12 months by body region are depicted in Figure 3. Across all body regions except the knee, work activities exacerbated musculoskeletal discomfort in more than 75% of the respondents who reported symptoms in each body region; work activities exacerbated discomfort in 62% of those with knee discomfort. In contrast, the knee was the body region with the highest percentage of respondents (65.4%) who indicated that non-work activities exacerbated discomfort, followed closely by the lower back and other lower extremity regions; fewer than half of respondents indicated that non-work activities exacerbated discomfort in the neck or upper extremities. Less than 15% of respondents indicated taking sick leave due to musculoskeletal discomfort. However, more than half of all respondents indicated taking pain-relieving medications—including up to 70% of individuals with shoulder and lower back discomfort. Furthermore, approximately one-third to one-half of ultrasonography users reported that they had sought medical care for the discomfort experienced across each body region. The shoulder (16.6%), wrist/hand (15.3%), and lower back (14.2%) were the body regions that had the highest prevalence of individuals who reported changing jobs or altering their work duties due to discomfort.
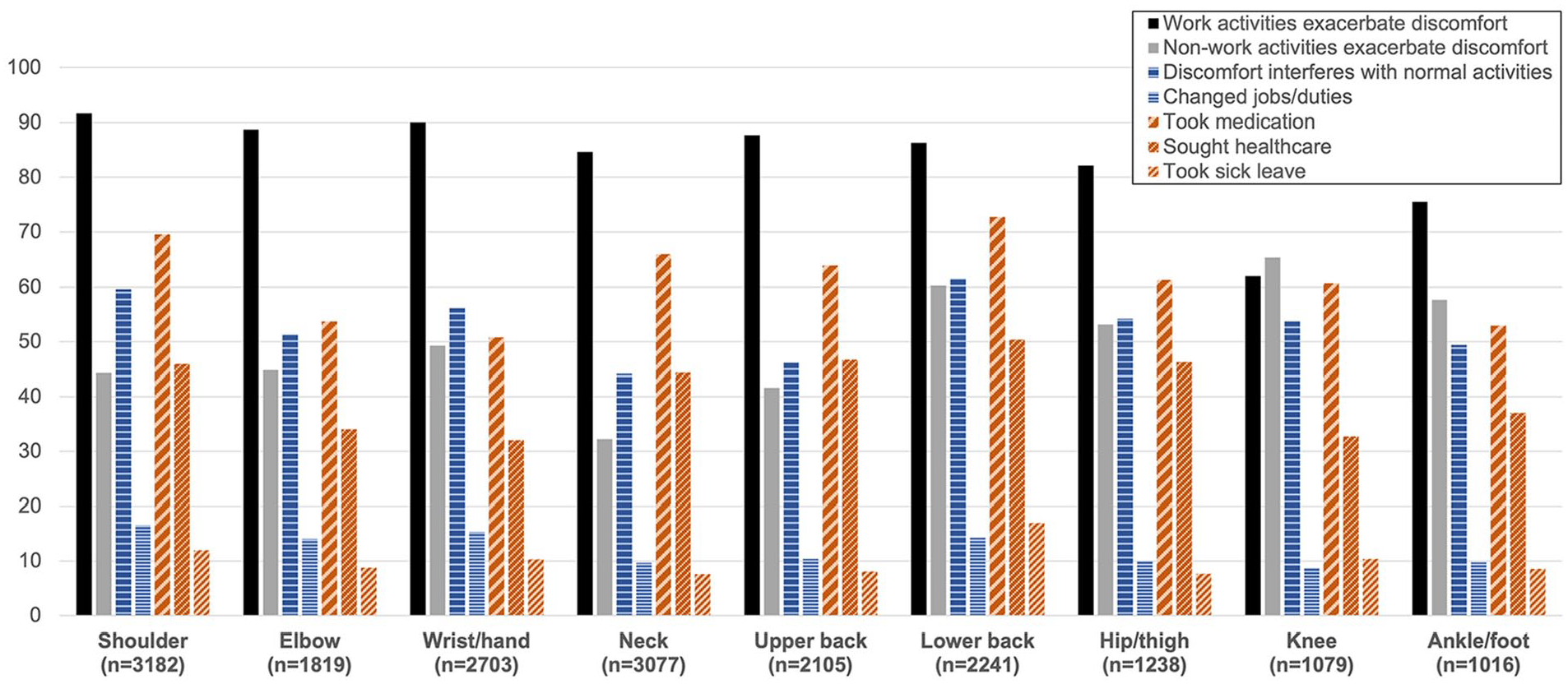
Percentages of ultrasonography users experiencing secondary impacts on musculoskeletal discomfort in each of nine body regions, including whether work and non-work activities exacerbate symptoms (solid bars), whether discomfort interferes with normal activities or required a change in jobs or duties (horizontal-patterned bars), and whether discomfort results in the use of medication, health care, or sick leave (diagonal-patterned bars). Percentages are calculated within each body region based on the number of respondents who reported discomfort in that specific body region.
Experiences of Work-Related Discomfort
Of the total sample, 86.0% (n = 3146) reported regularly experiencing musculoskeletal discomfort that they directly attributed to work, while 44.1% (n = 1613) and 40.0% (n = 1462) reported regularly experiencing work-related visual discomfort and headaches, respectively. One-quarter of participants (25.5%; n = 933) reported both visual discomfort and headaches that they attributed to work. Comparative analysis of individuals with and without work-related musculoskeletal discomfort demonstrated statistically significant differences across work system, process, and outcome variables. Within person(al) factors, there were significant differences in gender and race distribution between individuals with and without work-related musculoskeletal discomfort (P < .05) (See Table 1). Protective factors within work system variables of tools (i.e., adjustable equipment/spaces) and organization (i.e., work breaks, ergonomic policies, work culture, and trust in management) were rated to be higher in individuals without work-related musculoskeletal discomfort (P < .001) (See Table 2). Conversely, individuals who reported discomfort experienced interrupted workflow timing and pacing and experiencing pressure and poor performance more often than those without discomfort (P < .001).
Person(al) Factors [Mean (SD) / Frequency (%)] Compared Between Ultrasound Users Who Do Not (n = 513) and Do (n = 3146) Regularly Experience Work-Related Musculoskeletal (MSK) Discomfort.
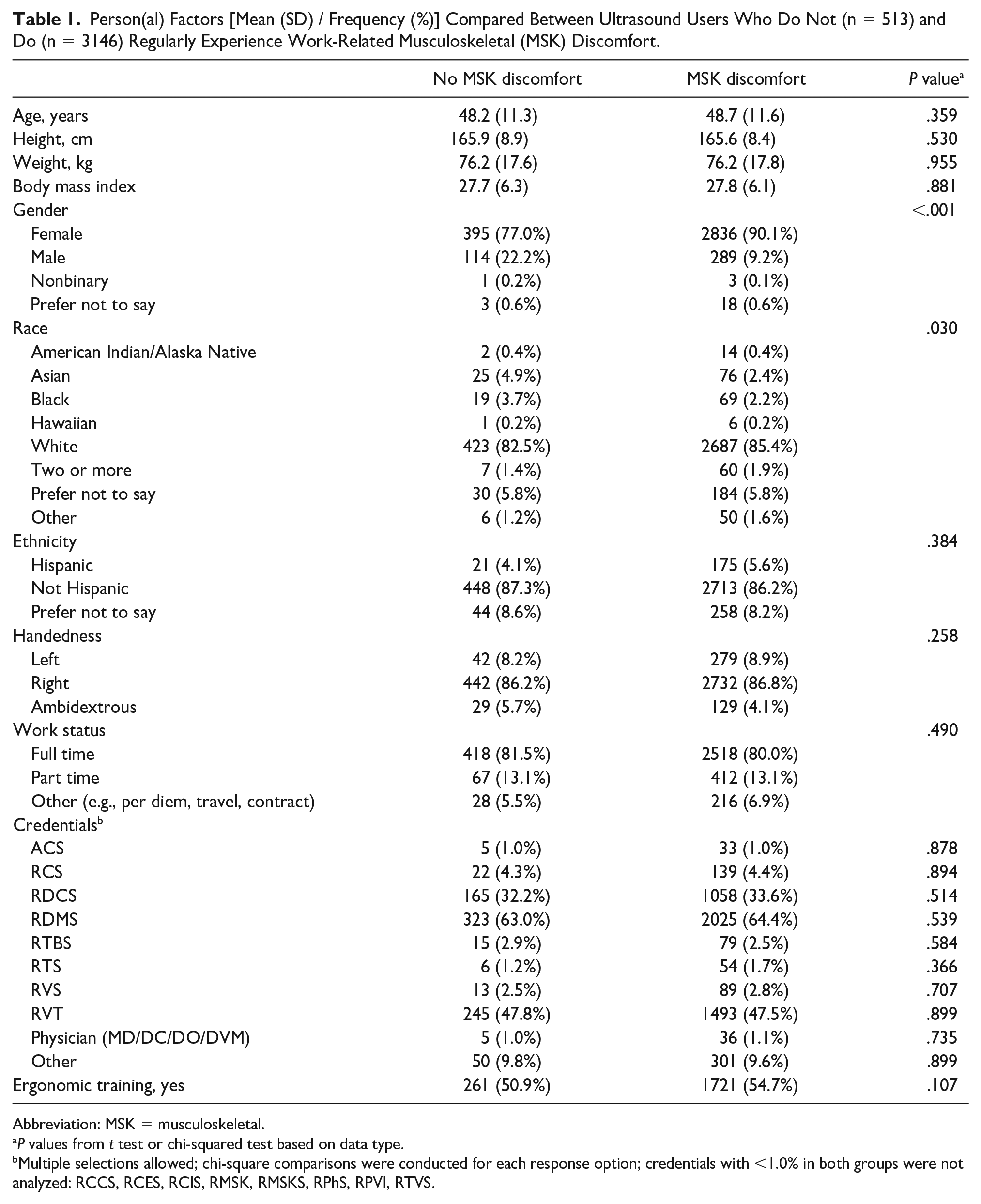
Abbreviation: MSK = musculoskeletal.
P values from t test or chi-squared test based on data type.
Multiple selections allowed; chi-square comparisons were conducted for each response option; credentials with <1.0% in both groups were not analyzed: RCCS, RCES, RCIS, RMSK, RMSKS, RPhS, RPVI, RTVS.
Work Systems (Other Than Person(al) Factors), Process, and Outcome Variables [Mean (SD) / Frequency (%)] Compared Between Ultrasound Users Who Do Not (n = 513) and Do (n = 3146) Regularly Experience Work-Related Musculoskeletal Discomfort.
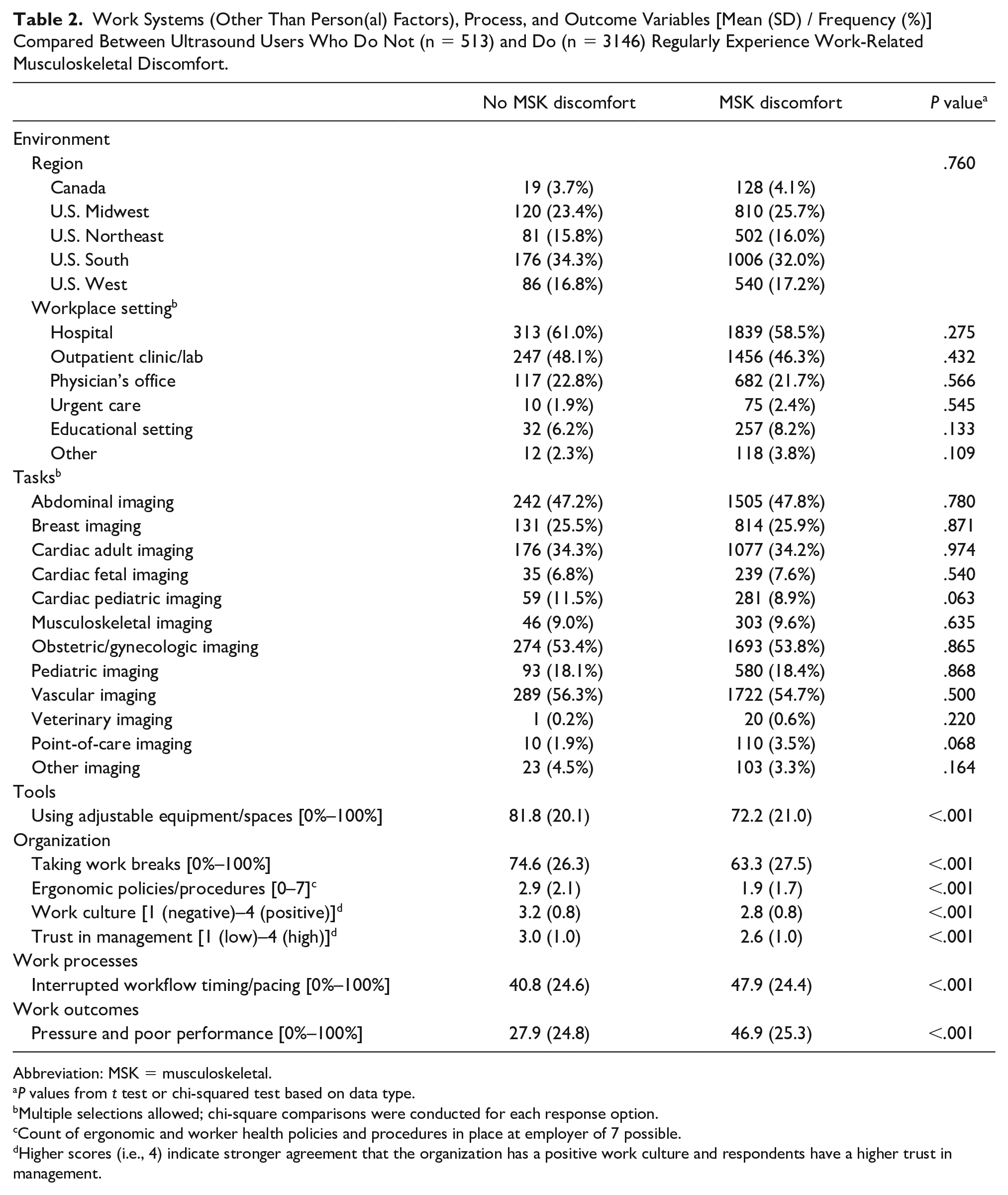
Abbreviation: MSK = musculoskeletal.
P values from t test or chi-squared test based on data type.
Multiple selections allowed; chi-square comparisons were conducted for each response option.
Count of ergonomic and worker health policies and procedures in place at employer of 7 possible.
Higher scores (i.e., 4) indicate stronger agreement that the organization has a positive work culture and respondents have a higher trust in management.
Factors Associated With Work-Related Discomfort
Table 3 presents the findings of individual regression models examining the variables within each SWS construct relative to the three primary outcomes of regularly experiencing work-related musculoskeletal discomfort, visual discomfort, and headaches. Among person(al) factors, identifying as female resulted in being 1.6 to 2.7 times more likely to report regularly experiencing one of the types of work-related discomfort (P < .001). Specific workplace environments or types of sonographic examinations performed were generally not related to experiencing work-related discomfort, except for individuals conducting breast examinations having a 25% higher likelihood of experiencing headaches (odds ratio [OR]: 1.25, 95% confidence interval [CI] [1.03–1.51], P = .027), and individuals conducting pediatric cardiac examinations being less likely to report regularly experiencing musculoskeletal discomfort (OR: 0.66, 95% CI [0.47–0.93], P = .018).
Odds Ratios of Reporting Experiencing Work-Related Musculoskeletal Discomfort, Visual Discomfort, or Headaches Within Each Work System Component and Work Processes Factor Categories Are Examined Separately in These Analyses; Note That Number of Respondents Varies Due to Some Incomplete Responses.
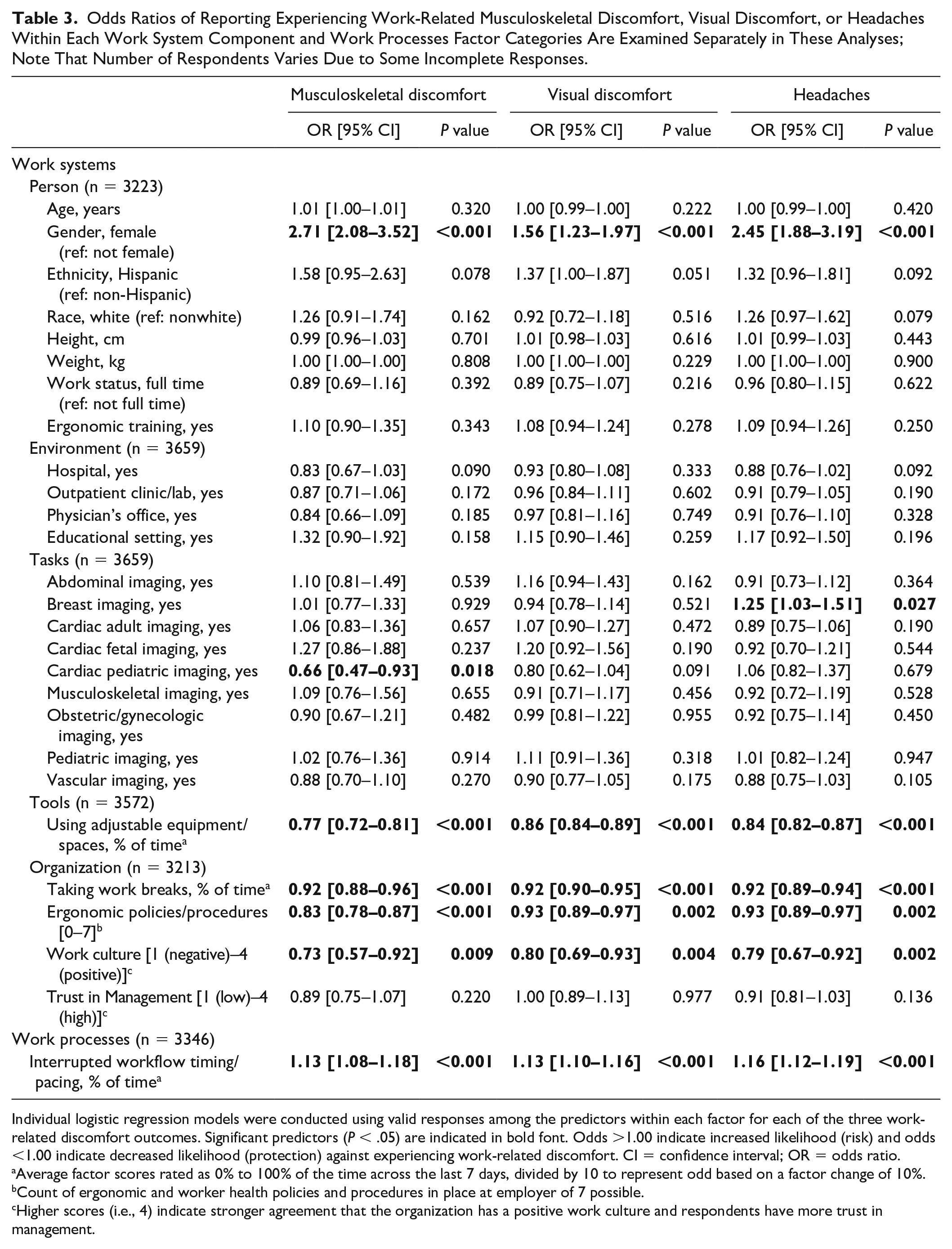
Individual logistic regression models were conducted using valid responses among the predictors within each factor for each of the three work-related discomfort outcomes. Significant predictors (P < .05) are indicated in bold font. Odds >1.00 indicate increased likelihood (risk) and odds <1.00 indicate decreased likelihood (protection) against experiencing work-related discomfort. CI = confidence interval; OR = odds ratio.
Average factor scores rated as 0% to 100% of the time across the last 7 days, divided by 10 to represent odd based on a factor change of 10%.
Count of ergonomic and worker health policies and procedures in place at employer of 7 possible.
Higher scores (i.e., 4) indicate stronger agreement that the organization has a positive work culture and respondents have more trust in management.
Regardless of environment or examination type, more frequently conducting examinations with adjustable equipment and workspaces was associated with a lower likelihood of experiencing work-related symptoms across all three work-related discomfort outcomes (P < .001). At the organizational level, more ergonomics policies and practices (P < .003), a more positively perceived work culture (P < .01), and a higher percentage of time taking adequate work breaks were each “protective” (i.e., odds ratios < 1), indicating a lower likelihood of associations with regularly experiencing all three types of work-related discomfort. More interruptions in workflow pacing were associated with a greater likelihood of reporting work-related symptoms across all three discomfort outcomes (P < .001), while trust in management was not associated with experiencing any of the work-related physical discomfort symptoms.
The final multi-factorial models combining critical factors across the SWS framework are presented in Table 4. First, the likelihood of regularly experiencing work-related musculoskeletal discomfort was higher for white females who reported more frequent interruptions to the timing and pacing of workflow, whereas those who were working in cardiac pediatric settings, were more frequently able to adjust equipment or workspaces, were working for employers with more ergonomics policies or practices, and were engaging in workplaces with more positive work cultures were less likely to report experiencing work-related musculoskeletal discomfort.
Odds Ratios of Reporting Experiencing Work-Related Musculoskeletal Discomfort, Visual Strain, or Headaches Across All Work System and Work Process Factors.
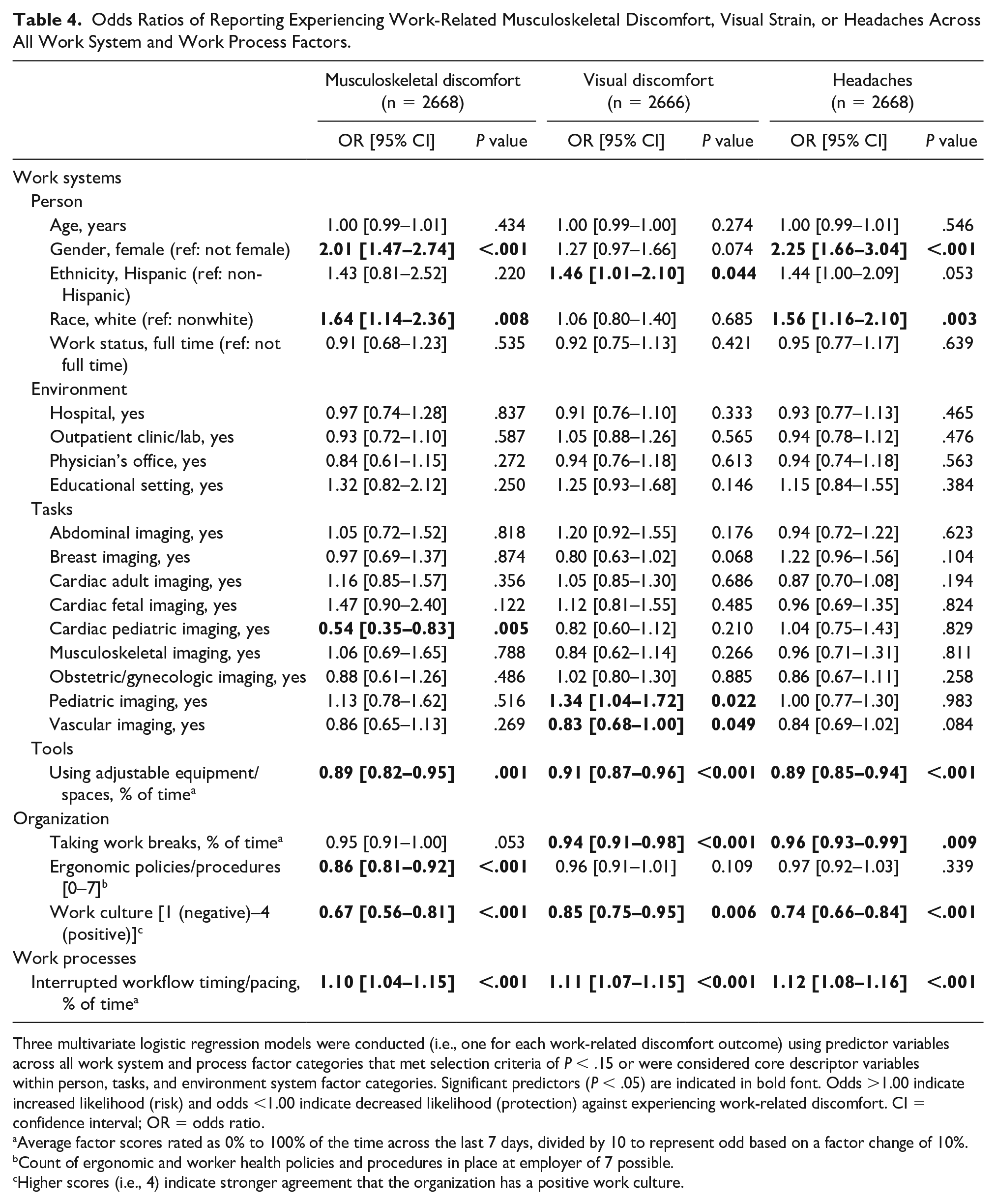
Three multivariate logistic regression models were conducted (i.e., one for each work-related discomfort outcome) using predictor variables across all work system and process factor categories that met selection criteria of P < .15 or were considered core descriptor variables within person, tasks, and environment system factor categories. Significant predictors (P < .05) are indicated in bold font. Odds >1.00 indicate increased likelihood (risk) and odds <1.00 indicate decreased likelihood (protection) against experiencing work-related discomfort. CI = confidence interval; OR = odds ratio.
Average factor scores rated as 0% to 100% of the time across the last 7 days, divided by 10 to represent odd based on a factor change of 10%.
Count of ergonomic and worker health policies and procedures in place at employer of 7 possible.
Higher scores (i.e., 4) indicate stronger agreement that the organization has a positive work culture.
Similarly, the likelihood of regularly experiencing headaches was also increased for white females who reported more frequent interruptions to the timing and pacing of workflow, and the likelihood of regularly experiencing headaches was lower for individuals working in positive workplace cultures, who were able to adjust their equipment, and who took appropriate breaks. No workplace environments or specific imaging procedures were associated with reporting of headaches when considering all factors. Finally, reports of experiencing work-related visual discomfort had a similar negative association with higher interrupted workflow and protective associations with good workplace culture, adjustable equipment, and work breaks. Visual discomfort differed from the other outcomes in that identifying as Hispanic and completing pediatric examinations were factors that increased the likelihood, while conducting vascular examinations decreased the likelihood of regularly experiencing work-related visual discomfort.
Discussion
This prospective survey research study was conceived, at the outset, as an important opportunity to build upon previous related work by gathering longitudinal data from a large cohort of ultrasonography users. This survey of 3659 ultrasonography users surpassed the sample size of previous studies by approximately 700 respondents, but the demographics of the participants in the current cohort are comparable to the most recent representative cross-sectional study of ultrasonography users completed in 2009.21,22 The findings of this study demonstrate the persistently high prevalence of work-related physical discomfort among ultrasonography users, highlight key work systems factors associated with increased likelihood of regularly experiencing work-related discomfort, and provide an impetus for action at the organizational and employer level.
State of Ultrasonography User Health
This study differentiated experiences of general musculoskeletal discomfort from work-related musculoskeletal discomfort and regular experiences of other work-related physical discomforts. Compared with the previous representative study that indicated 89.1% of sonographers experience musculoskeletal discomfort while scanning, 21 findings of the current study indicate a slightly lower prevalence with 86.0% of ultrasonography users regularly experiencing work-related musculoskeletal discomfort. In addition, slightly fewer than half of the ultrasonography users in this study regularly experience work-related visual discomfort and headaches. Barros-Gomes et al. 23 found a similar prevalence of headaches among cardiac sonographers (36%), which was greater than the prevalence of 20% in a reference group of nurses, administrative assistants, physicians, technicians, and others working in the same cardiology departments. Importantly, several factors including more time using adjustable equipment, consistently being able to take a variety of breaks each workday (i.e., mid-shift meal break, a short break during the first and second halves of a shift, and brief stretch breaks between examinations), a positive work culture, and reduced workflow interruptions were all found to be associated with a lower likelihood of experiencing these three types of work-related physical discomfort.
Nearly all respondents had experienced musculoskeletal discomfort within at least one body region with the last 12 months, and 92.5% experienced discomfort within the most recent week. Body regions with the areas of highest discomfort prevalence were the shoulder (71.7%), neck (61.1%), and the wrist/hand (57.5%), which remain the top three regions of discomfort with similar prevalence to previous reports of 74.6%, 65.8%, and 49.7%, respectively. 21 These persistent and consistent prevalence findings across time are concerning, particularly because of the other consistent finding that work activities exacerbate discomfort for many respondents. In nearly all body regions, >75% of those who experienced discomfort reported that work activities exacerbated that discomfort; yet, depending on the part of the body, fewer than about 15% of respondents took time off work or changed their job duties due to their discomfort.
These findings indicate that the majority of ultrasonography users are working in pain, a finding common among health care workers.23,24 Although the questionnaire did not differentiate between types of medication (e.g., over-the-counter, prescription), up to two-thirds or more of individuals with musculoskeletal discomfort take medication to alleviate their symptoms. This finding is similar to a recent study of echocardiographers that found about 65% reported taking over-the-counter medication for their work-related discomfort, and 15% reported taking prescription medications. 23 In other sectors of health care, there are concerns for reducing worker injuries and reducing the number of workers performing health care tasks while taking pain medication.25,26 These studies addressed work-related pain in these same body regions; however, they found that pain in these workers was related to higher levels of absenteeism, as opposed to working while taking medication.
Sonography Work Systems Factors Associated With Work-Related Physical Discomfort
Significant efforts have been made in recent years to increase ergonomic training for sonographers. Such training, which is categorized as administrative control, aims to improve workers’ knowledge of existing hazards, available control measures, safe work practices, and user-centric prevention techniques (e.g., stretching). Surveys conducted prior to 2017 by Scholl and Salisbury, 27 Peterson et al., 28 and Al-Rammah et al. 29 indicated that only one-quarter to one-third of sonographers had participated in sonography-related ergonomics training. Approximately half of the respondents in the current survey indicated that they had completed sonography-related ergonomics training with most indicating that training had occurred within 3 to 5 years. This finding seems to indicate that the emphasis on ergonomics training for ultrasonography users has increased. Respondents overwhelmingly reported that they were able to apply the ergonomics training and that it was helpful, which supports ongoing efforts to provide ergonomic training. However, between those who had training and those who did not, there was no differential experience of work-related musculoskeletal discomfort nor any association with the prevention of other types of physical discomfort. Safe work practices are constrained by the work environment and work organization; as such, training, while important and useful as indicated by this study’s participants, is not sufficient to reduce the prevalence of WRMSD in ultrasonography users.
In addition to training, employers must invest in other administrative and engineering controls that directly mitigate hazards, such as substitution with user-centered equipment and safety initiatives (i.e., policies and procedures). Findings in this study support these concepts as a greater percentage of the work time that respondents were able to use adjustable equipment (including ultrasound machines, examination tables, and chairs) and take breaks was associated with a reduced likelihood of experiencing work-related musculoskeletal discomfort, visual discomfort, and headaches. Conversely, participants who reported regularly experiencing work-related physical discomfort reported a higher percentage of time experiencing interruptions in workflow (due to extended shifts, adjusting schedules due to patient or administrative factors) and time working under pressure (i.e., feeling pressured to perform more examinations, feeling rushed when performing examinations, feeling that the quality of one’s work was less than one’s best). In addition to detrimental effects on worker health, such disruptions in workflow can result in physical and mental errors that lead to diminished patient outcomes. 30
In the current study, work culture was generally viewed as positive; however, other workplace factors were problematic. The positive view of the work culture was found to be protective of regularly experiencing work-related musculoskeletal discomfort, visual discomfort, and headache. Prior studies also found positive effects on worker well-being, health, and safety in connection with positive (supportive) work cultures. 31 Alternately, the mean level of trust in management was neutral, a finding similar to studies completed with radiographers, 32 nurses, 33 and other health professionals. 34 Although trust in management was higher among those who did not report regularly experiencing work-related musculoskeletal discomfort, management trust was not considered a significant predictor of physical discomfort when combined with other organizational factors. Of note, individuals working for employers who had fewer policies in place were more likely to regularly experience all three types of physical discomfort. In fact, a troubling finding was the significant lack of recommended ergonomics policies and procedures within the respondents’ workplaces at an average of only two out of seven policies. This finding coupled with more than two-thirds of individuals who reported ergonomic concerns indicating that their issue was not properly addressed and 6% reporting retaliation for reporting an ergonomics issue is concerning.
Need for Organizational Support, Inviting Employer Action
Solutions to reduce the risk of WRMSD are needed urgently; this clarion call appears in many prior studies of sonographers.5 –9,21,22 Yet, progress on reducing the prevalence of WRMSDs in ultrasonography users appears to be minimal, based on ongoing elevated WRMSD prevalence found in this study. The current study’s findings are consistent with 30 years of prior surveys: The prevalence of work-related musculoskeletal discomfort has been and is still quite high in ultrasonography users. This is a fact that ultrasonography users recognize and it must also be recognized by administrators and managers of ultrasonography workers in order to reverse this ongoing elevated trend.12,35 –37 Analyses in the current study demonstrated that work-related musculoskeletal discomfort, visual discomfort, and headache are connected to organizational factors that are addressable: using adjustable equipment, taking adequate breaks, implementing ergonomics policies and procedures, minimizing workflow interruptions, and providing a positive work culture.
Effective safety programs are multifaceted 38 and successfully establish a safety culture within the workplace. Safety culture is recognized as an important component of organizational (work) culture focused on “people’s perceptions about the extent to which the organization values safety (for workers, patients, and/or the environment), commits resources to safety-related initiatives and equipment, and promotes safe behaviors.” 39 Within health care workplaces, participatory ergonomics approaches provide workers with the opportunity and power to advocate for positive safety cultures and solutions to problems affecting their day-to-day working activities.40,41 Participatory ergonomics strategies that address risks to workers and potential errors in patient care can be time-intensive to develop, but the approach offers several advantages, including buy-in across all levels of the organization, avoidance of unexpected obstacles, opportunities for outside expertise (e.g., consultants), and integration of solutions acceptable to individuals across the organization. 42
As described on OSHA’s website and in numerous publications, management commitment and worker participation are two of the most important and essential elements of a successful safety management system.43 –45 Management establishes the culture of the organization and is the source of financial support for investments in equipment, space, adequate staffing, training, and all the other factors that affect worker health and well-being. Adopting a participatory approach, in which management and workers collaborate on hazard identification and intervention ideation, selection, and introduction will be more successful than a strictly top-down approach or training alone.
There is evidence of health care professionals gaining traction in combating WRMSD with administrative support, particularly in nursing, and associated with safe patient handling initiatives.46 –49 Published evidence aimed at administrators can support decisions for workplace change.50 –54 Most interventions, including education and training, adjustable equipment, and scheduling, start with management leadership (supervisors, managers, and hospital administrators) and a workplace culture that prioritizes employee safety, health, and well-being as much as patient safety and satisfaction. This holistic, systems approach is what is needed to reverse this unabated trend of elevated work-related disorders in ultrasonography users.
Limitations
A primary limitation of this study is that it is cross-sectional; because work factors and outcomes data were collected at the same time, causal inferences cannot be made. Second, although efforts were made to encourage participation across all specialties and among a variety of ultrasonography users, the survey methodology has the potential for selection bias in that the study participants may be different from the population of interest in one or more ways (e.g., in the prevalence of work-related discomfort, in the distribution of specializations). Efforts were made to minimize potential selection bias by providing a comparison of the demographic characteristics between those reporting work-related musculoskeletal discomfort and those who do not experience discomfort and controlling for these factors by including them as part of the final associational models. In addition to methodological limitations, the timing of this survey occurred during the second year of the COVID-19 pandemic. The pandemic and its effects on work and other aspects of life likely influenced responses to several questions in the survey. Subsequent surveys in this longitudinal study include questions about the effects of the pandemic on ultrasonography users’ work experiences and perspectives.
Conclusion
A new Sonography Work Systems framework, modeled after the SEIPS model, informed the contents of a first survey in a longitudinal research effort designed to explore factors impacting the health and well-being of medical ultrasound users. Regularly experiencing work-related musculoskeletal discomfort, visual discomfort, and headache were the three primary outcome measures of the study. Despite evidence of increased participation in ergonomics training among ultrasonography users, the prevalence of work-related discomfort was found to be similar to prior studies. Using adjustable equipment, taking work breaks, engaging in a positive work culture, and minimizing interruptions to workflow were key factors associated with reduced likelihood of work-related discomfort. Furthermore, ultrasonography users working in organizations with more ergonomic policies and procedures are less likely to report experiencing regular work-related musculoskeletal discomfort; yet, on average, organizations are only incorporating two of seven commonly recommended ergonomic policies and procedures. These findings highlight the need for action at the organizational level in which management and ultrasonography users collaborate to identify and implement evidence-based solutions to improve the health and well-being of medical ultrasound users.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793231170016 – Supplemental material for Cross-disciplinary Prevalence and Associated Factors for Work-Related Discomfort in Users of Ultrasonography: Implications for Sonography Professionals and Health Care Administrators
Supplemental material, sj-docx-1-jdm-10.1177_87564793231170016 for Cross-disciplinary Prevalence and Associated Factors for Work-Related Discomfort in Users of Ultrasonography: Implications for Sonography Professionals and Health Care Administrators by Shawn C. Roll, Yoko E. Fukumura, Carolyn M. Sommerich, A. Nicole Stigall-Weikle and Kevin D. Evans in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors thank the following individuals and organizations for their input and contributions to this project: Member Organizations of the WRMSD Grand Challenge Alliance; Yusef Sayeed, MD, MPH, MEng, CPH, CMRO, CME, COHC, MSKME, RMSK, DABPM, FAIUM; Kate Sayeed, MD; Samantha Yo, OTD; and Isaiah Bloom, BS.
Peer Reviewer Guarantee Statement
The Editor / Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor / Associate Editor had no involvement in the decision-making process.
Ethics Approval
The project was approved by the Ohio State University’s social and behavioral institutional review board (2021B0113).
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study has been provided by the following members of the WRMSD Grand Challenge Alliance with additional financial support from Biodex, part of Mirion Technologies. The views presented in this study are the authors and do not necessarily represent those of the supporting organizations: American Institute of Ultrasound in Medicine, American Registry for Diagnostic Medical Sonography and Inteleos, American Society of Echocardiography, Intersocietal Accreditation Commission, Joint Review Committee on Education in Cardiovascular Technology, Society for Vascular Ultrasound, Society of Diagnostic Medical Sonography, and Society of Diagnostic Medical Sonography Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.